Article Text

Abstract
Background: Systemic lupus erythematosus (SLE) is characterised by the presence of antibodies to double stranded DNA (dsDNA), which are involved in the pathogenesis of SLE. Previous studies showed that at least two thirds of patients develop a clinical relapse within six months after a significant rise in the anti-dsDNA level, and most relapses were prevented by the administration of corticosteroids at the time of the rise.
Objective: To determine whether mofetil mycophenolate (MMF) can prevent a clinical relapse without the side effects associated with corticosteroids.
Methods: 36 patients with SLE were examined monthly to determine whether a rise in anti-dsDNA level had occurred. A rise was defined as an increase of 25% of the level of the previous sample of at least 15 IU/ml within a four month period. After a rise patients were treated with MMF 2000 mg daily for six months. Patients were monitored monthly for the occurrence of a clinical relapse and to assess the serological activity and state of activation of CD4+, CD8+, and CD19+ lymphocyte subsets.
Results: Anti-dsDNA rose in 10 patients. Treatment with MMF was started in all these patients, and after six months no clinical relapse had occurred. Side effects were minimal. Antibodies to dsDNA decreased during the treatment (p<0.001), associated with a decrease in the state of activation of CD19+ lymphocytes. No changes were found in the state of activation of CD4+ or CD8+ lymphocyte subsets.
Conclusion: Administration of MMF after a rise in antibodies to dsDNA is well tolerated, decreases anti-dsDNA and B cell activation, and seems to prevent the occurrence of a clinical relapse in patients with SLE.
- systemic lupus erythematosus
- anti-dsDNA antibodies
- treatment
- mofetil mycophenolate
- dsDNA, double stranded DNA
- FITC, fluorescein isothiocyanate
- IMPDH, inosine 5′-monophosphate dehydrogenase
- MMF, mycophenolate mofetil
- PE, phycoerythrin
- SLE, systemic lupus erythematosus
- SLEDAI, SLE disease activity index
- VAS-Pa, visual analogue score of the patient
- VAS-Ph, visual analogue score of the treating physician
Statistics from Altmetric.com
- dsDNA, double stranded DNA
- FITC, fluorescein isothiocyanate
- IMPDH, inosine 5′-monophosphate dehydrogenase
- MMF, mycophenolate mofetil
- PE, phycoerythrin
- SLE, systemic lupus erythematosus
- SLEDAI, SLE disease activity index
- VAS-Pa, visual analogue score of the patient
- VAS-Ph, visual analogue score of the treating physician
Systemic lupus erythematosus (SLE), a multisystem autoimmune disease, is characterised by the occurrence of a multitude of autoantibodies, among which antibodies to double stranded DNA (dsDNA) are both sensitive and specific for active disease.1 The evidence suggests that antibodies to dsDNA are involved in the pathogenesis of SLE. For example, a rise in the level of anti-dsDNA is followed by a clinical relapse in most cases.2 One of the goals in treating patients with SLE is to prevent relapses. Previously, our group published the results of a long term follow up study, which showed that temporary treatment with corticosteroids started at the moment of a rise in anti-dsDNA levels significantly reduced the number of relapses in SLE.3 Nevertheless, such treatment did not reduce the cumulative dose of corticosteroids used compared with treatment based on clinical disease activity only. Additionally, we have investigated peripheral blood lymphocyte activation in patients with SLE longitudinally. Even during clinically quiescent disease a significant level of B and T lymphocyte activation was noted.4 Development of disease activity was paralleled by an increase in the percentages of activated CD4+ T cells and CD38 expressing (that is, activated) B cells. Those increases correlated with the specific increase in anti-dsDNA levels, suggesting that they are reflecting the ongoing specific immune response at a cellular level. Therefore, a therapeutic intervention interfering with T and B cell activation might replace the use of corticosteroids in preventing disease relapses.
Mycophenolate mofetil (MMF) is a prodrug of mycophenolic acid, a non-competitive, reversible inhibitor of eukaryotic inosine 5′-monophosphate dehydrogenase (IMPDH). It thereby blocks the de novo synthesis of guanosine nucleotides, which are required as building blocks for RNA and DNA synthesis.5 T and B lymphocytes are highly dependent on a functioning de novo pathway for the generation of guanosine nucleotides.5 Other cells can use the salvage pathway for the generation of these compounds. MMF acts at the late stage of lymphocyte proliferation, beyond the steps where either corticosteroids or cyclosporin have inhibitory activity. Theoretically, the selective inhibition of IMPDH by MMF may inhibit the proliferative responses of T and B cells with fewer side effects than other immunosuppressive drugs. Indeed, MMF has been shown to be as effective as oral cyclophosphamide in the treatment of diffuse proliferative lupus nephritis, but without producing severe side effects.6
Previous studies from our group have shown that a rise in the anti-dsDNA level predicts a clinical relapse of the disease.2 A significant rise in anti-dsDNA was shown to be followed by the occurrence of a relapse within six months in 16/24 patients.3 Administration of corticosteroids at the moment of a significant rise of anti-dsDNA can prevent relapse in the majority of cases.3 We suggest that administration of MMF after a rise in anti-dsDNA also prevents disease exacerbations without the side effects of corticosteroids.
PATIENTS AND METHODS
Patients
Consecutive patients were recruited from our cohort of patients with SLE who fulfilled at least four American College of Rheumatology criteria for SLE.7 Those eligible for the study had levels of antibodies to dsDNA at the time of inclusion as measured in the Farr assay >10 IU/ml, were at least 18 years old, and were not pregnant. Thirty six patients were included in the study. From these patients blood samples in EDTA were taken monthly for detection of antibodies to dsDNA. During the study, between January 1998 and April 2001, a significant rise in anti-dsDNA occurred in 10 patients. All these patients started with the study drug as soon as this rise was confirmed. As control, data from our previous study were used.3 In that study 24 patients with SLE with a significant rise in anti-dsDNA were followed up monthly thereafter without any change in immunosuppressive treatment. Sixteen of these patients relapsed within six months after a significant rise of antibodies to dsDNA. Criteria for a flare as well as the methods applied in the present study were the same as those of the previous one. Table 1 gives the characteristics of the patients and the historical control patient group, which were not statistically different. The local ethics committee approved the study. All patients gave written informed consent.
Characteristics of patients with systemic lupus erythematosus with a significant rise of antibodies to dsDNA either treated with MMF or untreated
Treatment
When a significant rise in anti-dsDNA was established, treatment was immediately started with MMF 2000 mg daily for the six month study period. Concomitant drugs were left unchanged during the whole study period with the exception of azathioprine, which was discontinued. In the historical patient control group medication was not changed after a significant rise in anti-dsDNA.
Follow up
During the six month treatment period, patients were seen every month at the outpatient clinic. At each visit signs and symptoms were recorded and it was decided whether or not a relapse was present according to previously defined criteria.2 The SLE disease activity index (SLEDAI) score was calculated.8 Special attention was given to side effects of treatment and the occurrence of infections. In the MMF treated patients the visual analogue score of the patient (VAS-Pa) and the treating physician (VAS-Ph), for lupus disease activity in the previous month, both on a scale from 0 to 100, were additionally recorded. At each visit blood was drawn for a full blood count and for the detection of anti-dsDNA, total IgG, complement components C3 and C4, and lymphocyte activation state.
Laboratory assessment
Anti-dsDNA antibodies were detected by the Farr assay using 125I labelled recombinant dsDNA (Diagnostic Products Corporation, Los Angeles, USA), which is uncontaminated with ssDNA. The Farr assay was performed according to the manufacturer’s instruction, and positive samples were measured at different dilutions in normal plasma to obtain measurements within the range of the assay. Results of this assay were expressed in IU/ml using Wo/80 as the ultimate standard.9 The normal value of this Farr assay in our laboratory is <10 IU/ml (which is the mean + 3 standard deviations for 50 healthy subjects); intra- and interassay variations are both <10%. A significant rise in anti-dsDNA levels was defined as exceeding 25% of the level of the previous sample of at least 15 IU/ml within a four month period, as has been defined before.2 To exclude rises due to interassay variation pairs of samples were always retested within one assay to ascertain the rise. For definite confirmation another plasma sample was obtained within one week of detection of the significant rise and analysed simultaneously with the two previous samples in which the rise was detected. A significant rise in anti-dsDNA level was considered established when the last sample confirmed the significant rise in anti-dsDNA.
Total IgG concentrations and complement C3 and C4 concentrations were measured by nephelometry (Behring).
FACS analysis of lymphocyte subsets was performed on a Coulter Epics-Elite equipped with a gated amplifier (Coulter Electronics, Mijdrecht, The Netherlands). Staining was done on whole blood samples for B (CD19) and T (CD3) cells, CD4 and CD8 subsets, and their activation markers (CD38 for B cells and CD25 and HLA-DR for CD4 and CD8 T cells, respectively). In brief, 5 μl (IQProducts, Groningen, The Netherlands) or 10 μl (Becton-Dickinson, Mountain View, CA) of phycoerythrin (PE) or fluorescein isothiocyanate (FITC) conjugated monoclonal antibody was added to 100 μl of whole blood. We used CD3(FITC)/CD25(PE)/CD38(PE)/HLA-DR(PE) from Becton-Dickinson. The monoclonal antibodies CD4(PE/FITC)/CD8(FITC)/CD19(PE/FITC) were obtained from IQProducts. B cells expressing CD38 at high intensity (CD38++) were regarded as activated.4 A total of 104 cells per sample were measured on the FACS. The list-mode data were analysed by the Lysis Stat software package (Becton-Dickinson) for the calculation of percentages of populations. All analyses were performed consistently by the same person.
Statistics
After a significant rise in the level of anti-dsDNA antibodies, 67% of the patients developed a clinical relapse of the disease within six months as shown in a previous study.3 When treatment with prednisone is started at the moment of a rise in anti-dsDNA antibodies the development of a relapse can be prevented.3 If it is assumed that a similar effect occurs when mycophenolate mofetil is given instead of prednisone then 10 patients are needed to demonstrate this effect (power 80%, two sided). Comparisons between patients and the historical control group of patients were made by χ2 test. Within the MMF treated group differences between time points were analysed using repeated measures analysis of variance with Bonferroni’s post-test for correction for multiple analysis. Correlations were calculated using Pearson’s correlation coefficient. A p value <0.05 was considered significant.
RESULTS
During the study, between January 1998 and April 2001, 36 patients gave their informed consent and were analysed monthly for levels of anti-dsDNA. One clinical relapse occurred that was not preceded by a rise in anti-dsDNA level. This patient had a minor relapse, characterised by pericarditis and fever, did not respond to non-steroidal anti-inflammatory drugs, and was negative for antibodies to dsDNA in the months before the relapse and at the moment of relapse. Ten patients started treatment with MMF as soon as a rise in anti-dsDNA was confirmed. None of the patients developed a clinical relapse in the six month study period, in which 1000 mg MMF was taken twice daily. MMF was tolerated well. Hypertension was reported in one patient with pre-existent hypertension. She was already being treated with angiotensin converting enzyme (ACE) inhibitors and responded to an increased dose. One patient reported a short period of fever, treated by her general practitioner with ofloxacin. This suspected infection, however, was not proved. No other periods of fever or infections were reported. Leucocyte counts remained stable, as did the absolute numbers of lymphocytes, erythrocytes, and platelets (table 2).
Effect of MMF institution on immunological and clinical disease parameters in patients with SLE after a significant rise of antibodies to dsDNA (n=10). Data are expressed as mean (SE)
During the study SLEDAI scores remained stable for all participating patients, except after two months (fig 1A). At that point the mean (SE) SLEDAI score was significantly lower than at the start of the study (2.8 (0.3) v 4.4 ± 0.5, p<0.05), owing to normalising complement levels in individual patients. Furthermore, patients judged their disease activity lower after two months of treatment (VAS-Pa 42.9 (7.7) v 20.1 (7.7), p<0.001), an effect that was maintained up to the end of the six month treatment period (fig 1B). No differences in VAS as scored by the treating physicians were found (fig 1C). In the historical control group 16/24 patients developed a relapse in the six month period after a significant rise in anti-dsDNA (p=0.0004 compared with the MMF treated patient group).

(A) SLEDAI score of 10 patients during a six month period of treatment with MMF after a significant rise in the level of antibodies to dsDNA. (B) VAS-Pa and (C) VAS-Ph represent the impression of the patient and the treating physician, respectively, of disease activity during the month before the visit to the outpatient clinic. *p<0.05, comparing different time points of evaluation with that at the start of treatment at time 0 (repeated measures analysis of variance with Bonferroni’s post-test). Data are presented as mean (SE).
After MMF was started a gradual drop in the level of antibodies to dsDNA could be shown in all patients, reaching its maximum at the end of the treatment period (fig 2A, table 2). The decline in antibody levels was selective, as total IgG levels were not significantly influenced during the treatment period (fig 2B, table 2). To obtain more insight into the effect of MMF on disease activity parameters, complement C3 and C4 levels were also measured monthly (figs 2C and D, table 2). No changes in the level of C3 nor in C4 were seen in the six month treatment period with MMF.

Levels of antibodies to dsDNA of each patient are shown from two months before the significant rise was established at t=0, until six months thereafter. MMF was started at t=0 and continued for six months (A). For each participant, levels of total IgG (B), complement C3 (C), and complement C4 (D) are also shown. In the graphs each individual patient is represented by a different symbol.
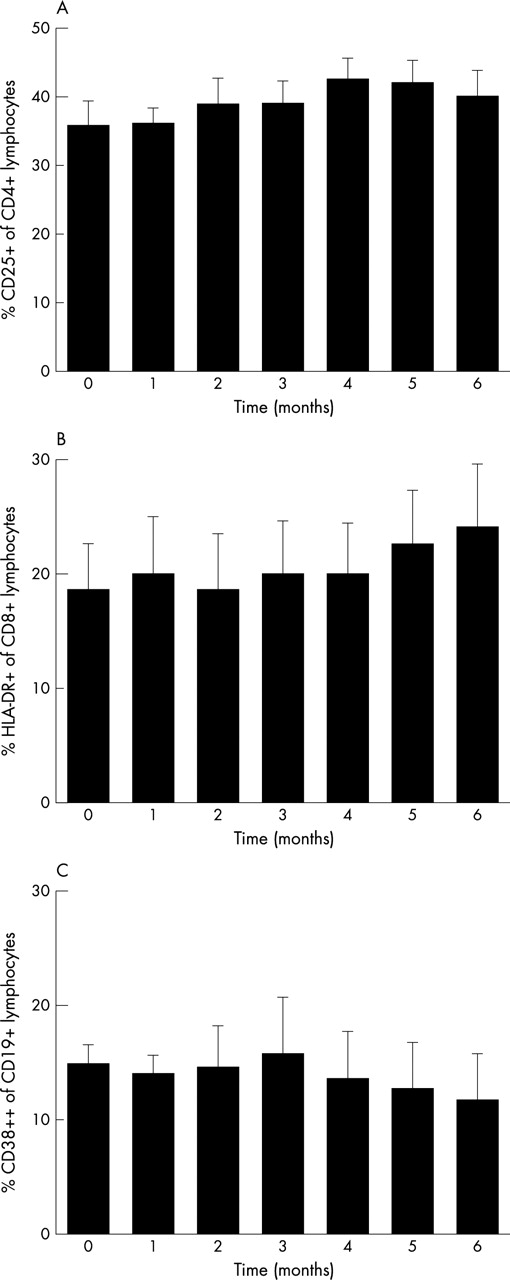
MMF specifically acts on activated lymphocytes. Therefore, activation markers on lymphocyte subsets were monitored during the study. Membrane expression was analysed for CD25 on CD4+ lymphocytes, HLA-DR expression on CD8+ lymphocytes, and CD38 expression on CD19+ lymphocytes, respectively, to assess the state of activation of these cells. The patient who probably had a non-documented infection showed an increase in the percentage HLA-DR positive CD8+ lymphocytes. Excluding this patient from the analysis of the state of activation of CD8+ lymphocytes did not influence the results. One patient showed a significant and sustained increase of CD19+CD38++ cells after two months of treatment that could not be explained. No changes in the state of activation of CD4+, CD8+, and CD19+ lymphocytes were found (fig 3). After excluding the patient with the unexplained rise in the percentage CD19+CD38++ cells, however, there was a decrease in the percentage of activated lymphocytes (p<0.01 at five months and p<0.001 at six months comparing different points of the evaluation with that at the start of treatment at time 0). The decrease in the percentage of activated CD19+ lymphocytes in these remaining nine patients was weakly associated with a decline in the level of antibodies to dsDNA (r=0.26, p=0.04).
{kind=link}
{kind=link}
{kind=link}
Activation state of lymphocytes during six months of treatment with MMF. (A) Activation state of CD4+ lymphocytes depicted as the percentage of these cells staining positive for the activation marker CD25. (B) Activation state of CD8+ lymphocytes depicted as the percentage staining positive for HLA-DR. (C) Activation state of CD19+ lymphocytes expressed as the percentage of CD38++ lymphocytes. Data are presented as mean (SE).
DISCUSSION
In this open pilot study we demonstrate that mycophenolate mofetil can prevent a clinical relapse in patients with SLE at risk for relapse and with no major side effects. In addition, we demonstrate an effect on B cell activation and antibody levels to dsDNA.
In recent years, following increasing survival of patients with SLE, the goal of treatment has extended from preventing mortality to reducing morbidity. It has been appreciated that recurrent disease activity and the use of immunosuppressive drugs have long term negative effects. In particular, the use of corticosteroids, the cornerstone of treatment of lupus, has been recognised as a major risk factor for many long term complications such as osteoporosis and increased incidence of cardiovascular disease.10 It is therefore of benefit to the patient to reduce episodes of disease activity and the use of corticosteroids. The present study combined both items by pre-emptive treatment with MMF.
We realise that our study has some methodological shortcomings. Although we and others could demonstrate that a rise in anti-dsDNA, especially as measured by Farr, is predictive of a future lupus flare,2,3,11,12 this finding is still a matter of debate. Studies from Canada and America could not confirm our findings.13–15 Walz LeBlanc et al suggested that serological activity was followed by a clinical relapse only in a subset of patients with SLE. In their paper, however, serological activity was not defined as a rise in antibodies to dsDNA, as we defined it, but as either persistently raised levels of anti-DNA antibodies or low complement levels.14 Recently, a prospective study from the Hopkins lupus cohort did show that an increase in anti-dsDNA is somewhat predictive of flares.16 However, in that study, the majority of rises were not followed by a flare.16 Differences in methodology, such as the time interval between blood sampling and between the rise in antibodies and clinical flare, in definitions for a significant rise and flare, and for serological activity, and differences in the included patients may well account for the discrepancies mentioned.
Another drawback of the study is its uncontrolled design. We deliberately chose such a design as we have shown in previous studies that after a significant rise of antibodies to dsDNA, 67–89% of patients have a relapse.2 Many of these patients did not want to volunteer for a randomised controlled study in which no treatment was given after a rise of anti-dsDNA in one of the two arms. In addition, we considered such an approach unethical. Because of these limitations we were faced with an “unblinded” study in which we had to compare results with those from a previous study. We used the “no treatment arm” from that study for comparison. The unblinded design made the patient and physician VAS less reliable. Nevertheless, the SLEDAI score did not increase and even significantly decreased after two months of treatment, in accordance with the patients’ perception of disease activity. A second limitation might be that patient groups were, probably, not fully comparable. Although no statistical differences were present between patients and historical controls, proteinuria tended to be more prevalent in the historical control group (p=0.06). Thus, the possibility that the patients in the present study had a less severe course of the disease cannot be excluded. Despite these limitations, we feel that most of the data presented, especially for the Farr assay and lymphocyte activation, will not have been influenced by the unblinded design of the study, and allow some conclusions.
MMF is a promising new immunosuppressive drug which has been shown to be effective in the treatment of lupus nephritis in an open label trial and in one controlled trial.6,17 It has also been reported to be useful in the treatment of extrarenal relapses of the disease.18 The effect of MMF at a cellular level can be demonstrated in vitro by flow cytometry.19 The drug primarily acts on activated T and B lymphocytes.19 Our results are in line with these data. As published previously, patients with SLE show increased percentages of activated lymphocytes, B lymphocytes in particular.20,21 The rise of antibodies to dsDNA, which occurs before disease activity in most patients, is paralleled by further activation of B lymphocytes. These B cells, expressing high levels of CD38, spontaneously produce IgG class anti-dsDNA in vitro.4 The present study intervenes at a moment that a significant rise of antibodies to dsDNA occurs and, thus, B cells are activated. Conceivably, therefore, a selective effect of MMF occurs on these cells.
In conclusion, our study shows that the occurrence of a clinical relapse in patients with SLE at risk for relapse is prevented by the use of MMF, and that the drug is well tolerated. Whether this treatment is as effective as a tapering course of corticosteroids has yet to be proved in a prospective controlled trial.
Acknowledgments
Roche Pharmaceuticals B.V. is kindly acknowledged for their support of the study drug.