Article Text

Abstract
Objective: To identify variables that can predict a progressive outcome after one year of follow up in patients presenting with undifferentiated polyarthritis (UPA) at an early arthritis clinic.
Methods: New patients with arthritis in two or more joints of less than three years' duration were categorised at entry as UPA or as rheumatoid arthritis (RA) based on the clinical diagnosis of the rheumatologist. Outcome variables after one year were radiographic damage (Sharp/van der Heijde score) and functional status (Health Assessment Questionnaire: HAQ score). A progressive disease at one year was defined as radiographic progression ≥4, or one year radiographic damage ≥10, or HAQ score ≥1. The baseline variables of patients with UPA with a progressive or mild outcome were compared.
Results: 280 patients (70% women; median age 56 years (range 18–90), median duration of symptoms 3.5 months) were included. 203 (72%) patients were clinically diagnosed as having RA and 77 (27%) as having UPA. The group of patients with progressive UPA (n=32 (42%)) had a significantly higher mean age, prevalence of arthritis of the hands, and disease activity (DAS28) at the first visit compared with the patients of the mild UPA group (n=45 (58%)). The RA group had significantly more frequent serum IgM-RF positivity, higher mean disease activity (DAS28) and mean C reactive protein concentration, more frequent symmetric arthritis, and arthritis in more than three joint groups than the progressive UPA group. Six (19%) of the progressive UPA group versus eight (4%) of the RA group did not receive disease modifying antirheumatic drugs during the first year.
Conclusions: After one year of follow up, 32 (42%) of the patients with UPA had a progressive disease. A progressive outcome was associated with older age, higher disease activity, and arthritis of the hands at baseline. To avoid undertreatment of patients with UPA, treatment should be based on severity rather than on diagnosis.
- undifferentiated polyarthritis
- prognosis
- outcome
- ACR, American College of Rheumatology
- CRP, serum C reactive protein
- DAS28, disease activity score
- DMARD, disease modifying antirheumatic drug
- HAQ, Health Assessment Questionnaire
- IgM-RF, serum rheumatoid factor
- RA, rheumatoid arthritis
- UPA, undifferentiated polyarthritis
Statistics from Altmetric.com
- ACR, American College of Rheumatology
- CRP, serum C reactive protein
- DAS28, disease activity score
- DMARD, disease modifying antirheumatic drug
- HAQ, Health Assessment Questionnaire
- IgM-RF, serum rheumatoid factor
- RA, rheumatoid arthritis
- UPA, undifferentiated polyarthritis
Rheumatoid arthritis (RA) is a chronic inflammatory joint disease of unknown cause with a large variation in the severity of inflammation and joint destruction. Joint damage starts in an early phase of the disease.1,2 To prevent joint destruction, there is growing consensus that optimal management of RA requires both early diagnosis and early aggressive treatment. However, therapeutic decisions are often difficult to make because of the non-specific early clinical features of RA.3
The 1987 revised criteria for RA of the American College of Rheumatology (ACR; formerly, the American Rheumatism Association) have a limited value (a low sensitivity and specificity) in early arthritis, because they were developed in patients with established disease.4–8 In contrast, an experienced rheumatologist can make a reliable clinical judgment on the presence or absence of RA after two weeks.9 Most patients with diseases such as psoriatic arthritis, sarcoidosis, or reactive arthritis can easily be separated from patients with RA. In the remaining patients with undifferentiated oligoarthritis and polyarthritis (UPA), defined as arthritis of more than one joint without fulfilment of the ACR criteria for RA, the diagnosis may change in the first years of follow up. Some patients will enter remission, some will progress to RA, and some to another rheumatic disease such as spondyloarthropathy. There is a scarcity of studies on the outcome and prognostic factors of patients with UPA in an early phase10–16 in comparison with studies of early RA.1–3,17–20 Also, patients with a diagnosis of UPA may be perceived as not in need of disease modifying antirheumatic drug (DMARD) treatment to the extent that patients with RA do.
The purpose of this study was (1) to find prognostic factors at entry for progressive UPA after one year; (2) to investigate the outcome after one year in patients with progressive UPA compared with the outcome after one year in patients with a clinical diagnosis of RA at entry.
PATIENTS AND METHODS
Patients
In a prospective study of patients with early arthritis seen at a large rheumatology outpatient clinic, The study comprised patients who were referred between September 1995 and April 1998, aged 18 years or older, with peripheral arthritis of at least two joints and less than three years of symptom duration. Patients who had previously been treated with a DMARD, patients with bacterial, psoriatic, or crystal induced arthritis, and patients with reactive arthritis, osteoarthritis, sarcoidosis, or systemic autoimmune diseases were excluded. Patients were diagnosed as having RA based on the clinical diagnosis of an experienced rheumatologist at the second visit to the clinic (one to three weeks after the first visit); the remainder of the patients were considered as having oligoarthritis or polyarthritis (UPA).
Disease variables
A trained investigator performed a structured interview and physical examination within two weeks of the first visit to the rheumatologist. Follow up assessments were performed at three, six, nine, and 12 months.
Variables assessed were demographic characteristics, time of onset of complaints (defined as persistent pain, swelling, or both), duration of morning stiffness, serum rheumatoid factor (IgM-RF), serum C reactive protein (CRP), disease activity score (DAS28: a composite score based on erythrocyte sedimentation rate, number of painful joints and number of swollen joints (both by 28 joint count), and patient global assessment by visual analogue scale,21 the number of painful and the number of swollen metatarsophalangeal joints, the physician's global assessment of disease activity, and pain by visual analogue scale.
Outcome variables at one year were the radiographic damage and functional status.
Radiographs of the hands and feet were obtained at baseline and after one year. Joint space narrowing and the number of erosions were scored by the Sharp/van der Heijde method),20 with a maximum possible score of 448. All radiographs were scored by a trained researcher who was blinded to the clinical data of the patients. The radiographs were read in pairs with an unknown time sequence. Radiographic progression, expressed as the delta damage, was computed by subtracting the initial Sharp/van der Heijde score from that at one year. Functional status was determined at entry and after one year by a validated Dutch version of the Health Assessment Questionnaire (HAQ)22 with a range of 0 to 3 (good functional status to maximally disabled).
The clinical diagnosis of RA or UPA was revised by the rheumatologist at one year.
Analysis
Because there are no criteria available to define the severity of UPA, the UPA group was divided arbitrarily into a progressive disease and a mild disease group at the one year follow up; UPA was defined as progressive if one or more of the following criteria were present: radiographic progression ≥4 within one year, radiographic damage ≥10, or HAQ score ≥1 at one year.
Baseline variables of patients with progressive and mild UPA were compared by Student's t test. Subsequently variables significantly different (p<0.05) between the mild and progressive UPA group were entered into a forward stepwise logistic regression to find the best combination of variables distinguishing both groups. Odds ratios for variables significantly associated with baseline characteristics for a progressive UPA were computed. Finally, the effect on outcome variables of a transition from UPA at baseline to RA at one year was evaluated.
All analyses were carried out with SPSS 9.0.
RESULTS
Three hundred and twenty three patients were eligible for the study. Seven patients were excluded because they refused to participate (n=6), or had moved (n=1). The remaining 316 patients were included in the study, of whom 280 (89%) completed the one year follow up. Of these 280 patients, 203 (72%) were clinically diagnosed by the rheumatologist as RA and 77 (27%) as UPA at baseline. Forty five (58%) of these patients with UPA had polyarthritis and 32 (42%) had oligoarthritis.
The reasons for loss to follow up after one year were death (n=3; from malignancy (n=2), from renal failure (n=1)), moving home (n=7), and non-compliance (n=27). Of the 37 (13%) patients who were lost to follow up, 22 (59%) were clinically diagnosed as RA and 15 (41%) as UPA. The baseline characteristics of the 15 patients with UPA lost to follow up were similar to those of the 77 completers (data not shown). However, the 22 patients with RA lost to follow up had a significantly higher mean baseline DAS28 score (p<0.05) than the 203 completers. The mean follow up of the UPA non-completers was 5.6 months and the mean of their last DAS score was 3.5 (the mean DAS score of the completers at six months was 2.9).
The first analysis was performed to determine prognostic factors for a progressive course of UPA. Of the patients qualified as “progressive UPA”, 21 (66%) fulfilled the criterion of radiographic damage ≥10, 15 (47%) had a delta damage ≥4, and 16 (50%) had an HAQ score ≥1 at one year. Based on the one year outcome, 32 (42%) patients with UPA were categorised as progressive and 45 (58%) as mild. Comparison of the baseline characteristics between the mild and progressive UPA groups showed significant differences. The progressive UPA group had a significantly higher mean age, prevalence of arthritis of the hands (p<0.01), and higher disease activity (DAS28; p<0.05) than the mild UPA group (table 1).
Comparison of baseline characteristics between mild UPA, progressive UPA, and the RA groups
The next step was to search for differences between the progressive UPA and RA groups. At baseline, the RA group showed a significantly higher percentage of serum IgM-RF positivity, higher mean disease activity (DAS28) and mean CRP concentration (p<0.001), more frequent symmetric arthritis (p<0.01), and arthritis in more than three joint groups (p<0.05) than the progressive UPA group (table 1).
There was a gradual increase from mild to progressive disease between patients with mild UPA, progressive UPA, and RA in the following characteristics: age, involvement of at least three joint groups, symmetric arthritis, and disease activity (DAS28) (table 1).
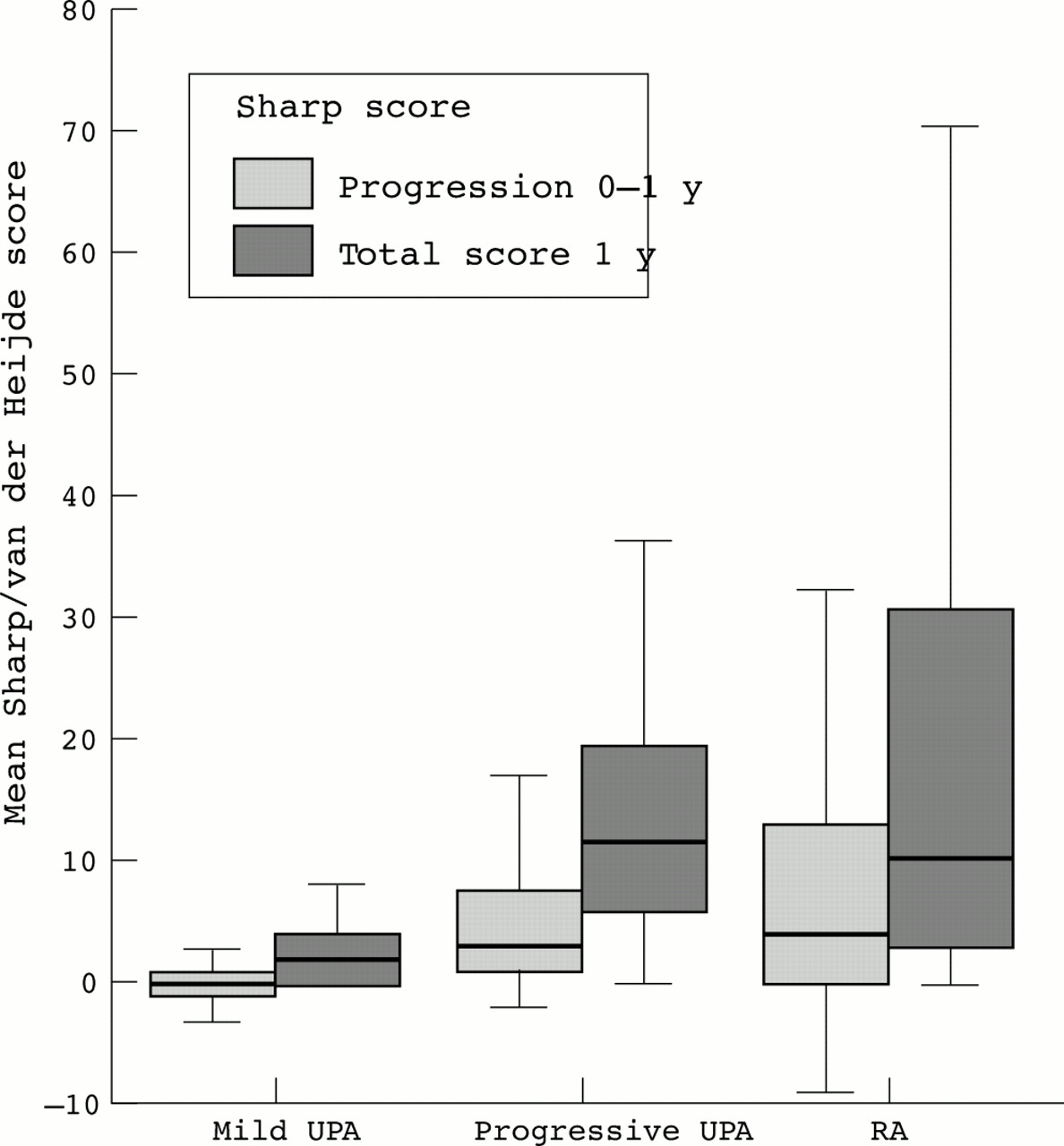
The radiographic damage and radiographic progression at one year was least in the mild UPA and highest in the RA group (fig 1). The mean one year HAQ score was highest in the progressive UPA group (fig 2).
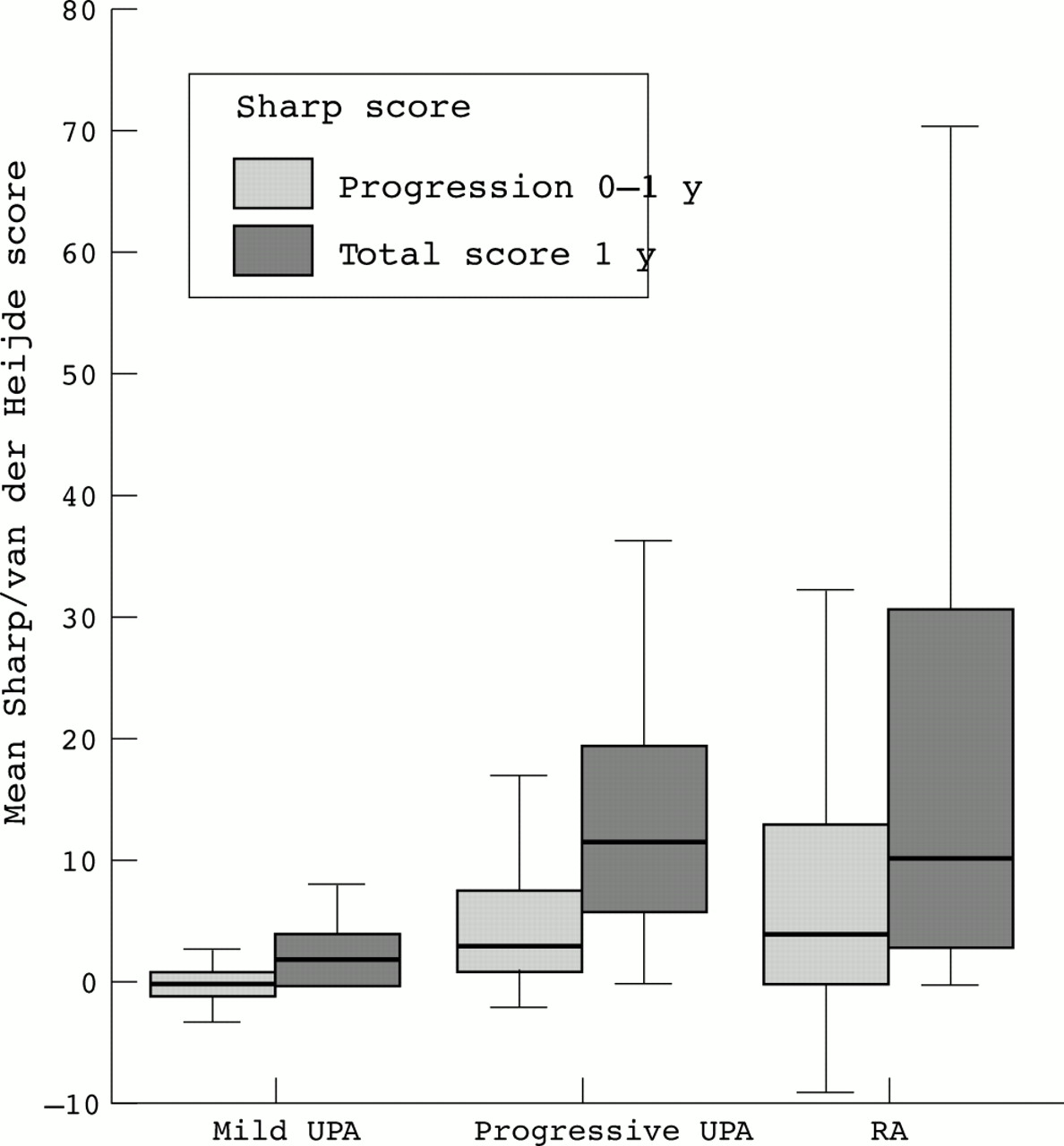
Radiographic progression at one year.

{kind=link}
{kind=link}
One year HAQ score.
To identify independent prognostic variables of progressive UPA, a stepwise logistic regression analysis was performed. Among the 77 patients with UPA, age (odds ratio=1.05; p<0.01; 95% confidence interval (95% CI) 1.01 to 1.09) and arthritis of the hands (odds ratio=4.2; p<0.05; 95% CI 1.04 to 17) proved to be the optimal predictors for progressive disease. In other words, for every additional year of age there was a 1.05-fold higher risk of having a progressive disease and patients with arthritis of the hands were 4.2-fold more likely to have a progressive disease than patients without arthritis of the hands.
To evaluate the effect of a transition from the diagnosis of UPA at baseline to the diagnosis of RA after one year, patients were categorised again after one year. In the patients clinically diagnosed by the rheumatologist as having UPA at baseline and classified as progressive at one year, 5 (16%) were diagnosed as having RA by the rheumatologist after one year and 10 (31%) fulfilled the ACR criteria for RA. There was no significant difference between the patients with UPA diagnosed as having RA at one year and the patients diagnosed as having UPA in terms of radiographic damage or disease activity.
The proportion of patients that had ever used DMARDs during the first year was larger in the RA group than in the progressive UPA group (96% v 81%, p<0.05; table 2). Moreover, the mean (SD) period of DMARD use was longer for the RA group than for the progressive UPA group (8.0 (3.2 ) v2 5.7 (4.3) months). After one year of follow up, patients with RA used sulfasalazine and methotrexate more often and hydroxychloroquine less often than patients with UPA (table 2).
Prescribed DMARDs during the first year of follow up
DISCUSSION
In this study almost half of the patients with early UPA had a poor functional status, progressive radiographic damage, or both at one year. However, only 81% of these patients were treated with DMARDs. Patients with a progressive disease were older and had involvement of the hands more often than patients with mild disease.
The investigation of early arthritis is hampered by the lack of a clear definition of RA. The ACR criteria for RA have several shortcomings in early arthritis. For example, sensitivity and specificity are too low5,10,11,23,24; synovitis has to be present for six weeks; and the criteria are no longer fulfilled when synovitis subsides in response to treatment. Also, individual criteria cannot be studied as predictors for the development of RA, because these factors are part of the criteria set. This disadvantage is not present when RA is defined as the clinical diagnosis of an experienced rheumatologist. Diagnosis of an experienced rheumatologist seems to be more subjective but has been found to be reliable.9 Because the final goal of classification of patients with early arthritis is to predict the prognosis, the focus should be shifted from classifying patients into RA and non-RA categories, towards different outcome categories.
The few available studies of the outcome of early undifferentiated arthritis and rheumatoid arthritis have used different outcome variables, such as the persistence of arthritis,10 functional ability,11 and, as in the present study, a combination of functional ability and radiographic damage.15 The comparison of these studies is further complicated by differences in the definition of UPA. In the present study, patients with progressive UPA could be differentiated from patients with a mild disease by an older age and more frequent involvement of the hands at baseline than in patients with a mild disease. This accords with a study12 of patients with palindrome rheumatism in which older age, early involvement of hand joints, and also female sex and a positive IgM-RF predicted the subsequent development of RA. Others10,14,16 confirmed the finding that IgM-RF positivity was associated with the onset of RA and persistence of arthritis. Tunn and Bacon10 examined predictors for persistence of arthritis after one year in a cohort of 65 patients with early UPA. They showed that the combination of IgM-RF positivity with an increased erythrocyte sedimentation rate carried a high relative risk for persistent arthritis. In a study by Wolfe et al14 IgM-RF positivity also was the best predictor of development of RA. The association of a positive rheumatoid factor with progressive UPA was not found in our study (table 1).
Green et al16 studied predictors for disease outcome at six months in patients with early arthritis. They concluded that predictors for persistent disease were a longer disease duration, IgM-RF positivity, and the presence of the shared epitope. In the present study, it was also found that a short disease duration was associated with a mild disease outcome, but the correlation was not strong. Furthermore, Green et al concluded that a baseline CRP is not predictive in very early inflammatory arthritis, which accords with our finding for patients with UPA.
Harrison et al,11 focusing on the prediction of future disability in 277 patients with early inflammatory polyarthritis, found that female sex, longer disease duration, large joint involvement, and high baseline HAQ were associated with a high HAQ score after one year. In this cohort, HLA-DRB1 alleles had no influence on the likelihood of disease persistence and only a modest association with functional disability. In the subgroup of seronegative patients however, HLA-DRB1 did have an influence on the development of erosions.15 In the present study, genetic tests were not performed, which makes comparison difficult.
The study of UPA may seem irrelevant if it is assumed that patients with progressive UPA actually have RA. However, only 16% of the patients with progressive UPA were clinically classified as having RA by the rheumatologist at one year and only 31% fulfilled the ACR criteria. From the total UPA group, 10% were clinically classified as having RA by the rheumatologist at one year and 17% fulfilled the ACR criteria. There was no significant difference in outcome (radiographic damage) between patients changing after one year from the diagnosis of UPA into RA and patients retaining the diagnosis of UPA.
According to Hülsemann et al13 the outcome of patients with UPA seems to be less severe compared with those with RA. Complete remission occurred in 54% of the patients with UPA and only 7% of them developed RA after two years. A difference from our study was that 11% of their population had reactive arthritis, which was an exclusion criterion in our study. The same high percentage of patients reaching complete remission in UPA was found by Wolfe et al.14
In the present study more aggressive treatment was prescribed for patients with RA compared with patients with progressive UPA. Whereas 4% of the patients with RA did not receive a DMARD during the first year, 19% of the patients with progressive UPA were not treated with DMARDs, which suggests insufficient treatment.
In conclusion, in this study 42% of the patients with UPA showed a severe functional status, progressive radiographic damage, or both after one year which could be predicted by age, a high disease activity score, and arthritis of the hands at baseline. These patients developed a progressive disease that may not be recognised and treated adequately in time. A considerable number of the progressive UPA group were treated with a mild—that is, an antimalarial, drug—or were not treated with a DMARD at all. Therefore, treatment strategy should be focused more on disease severity than on diagnosis alone.
Acknowledgments
We thank Janneke de Bruin for the scoring of the radiographs and Anne-Marie Abrahams for the collection of data.