Article Text

Abstract
Objectives: To determine whether rheumatoid factors (RFs), measured as continuous variables by time resolved fluoroimmunoassay, reflect disease activity in rheumatoid arthritis (RA). Further, to study the association of RFs and other disease activity parameters with radiological joint damage, especially in individual patients.
Methods: In active, early RA, IgM and IgA RFs, as well as erythrocyte sedimentation rate (ESR), C reactive protein (CRP), tender joint score, and swollen joint score were assessed regularly. At the study start and at 56 and 80 weeks, radiographs of hands and feet were assessed by the Sharp score (van der Heijde modification). Associations between RFs and disease activity parameters were studied. In addition, associations between radiographic damage and disease activity parameters (baseline and time integrated) were analysed by non-parametric tests and multiple regression analysis. The relation between time integrated disease activity parameters and radiological damage in individual patients was analysed and visualised.
Results: 155 patients were included. RF levels were strongly associated with the disease activity parameters (especially ESR and CRP) and with each other. All disease activity parameters, at baseline as well as time integrated parameters, were associated with (the progression of) radiographic damage. Moreover, in individual patients, a linear relationship between time integrated disease activity parameters and progression of radiological damage was seen.
Conclusion: RFs, measured as continuous variables, can be considered as disease activity parameters in patients with RA. The level of RF at baseline and the exposure to RF over time is associated with radiological damage. In individual patients, there is a constant relation between disease activity and radiological damage.
- rheumatoid factor
- disease activity
- outcome
- fluoroimmunoassay
- AUC, area under the curve
- CRP, C reactive protein
- ELISA, enzyme linked immunosorbent assay
- ESR, erythrocyte sedimentation rate
- RA, rheumatoid arthritis
- RF, rheumatoid factor
- SHS, Sharp score, modification van der Heijde
- SJC, swollen joint count
- TJC, tender joint count
Statistics from Altmetric.com
- AUC, area under the curve
- CRP, C reactive protein
- ELISA, enzyme linked immunosorbent assay
- ESR, erythrocyte sedimentation rate
- RA, rheumatoid arthritis
- RF, rheumatoid factor
- SHS, Sharp score, modification van der Heijde
- SJC, swollen joint count
- TJC, tender joint count
Rheumatoid factor (RF) has been the subject of intensive study, but definite conclusions on its role in rheumatoid arthritis (RA) have not been drawn.1 Prospective studies on the role of RF as a disease activity parameter show significant correlations with C reactive protein (CRP)2–4 and with swollen joint counts (SJC),4 but not with the erythrocyte sedimentation rate (ESR).3
Various prospective studies showed a clear association between RF at baseline and the later development of erosions.2,4,5 Moreover, in one of these studies, baseline RF also correlated with the elapsed time until the first erosion.2,5 These data suggest that RF predicts radiological outcome. Van Leeuwen et al found a moderate association between time integrated RF as well as time integrated CRP and the development of erosions in patients with RA.4,6 In a later study, she demonstrated a linear relation between time integrated CRP and radiological damage in individual patients.7 However, RFs have not been studied in individual patients.
In the above-cited studies RFs were measured by qualitative or semiquantitative methods (such as Waaler-Rose and latex fixation tests) or by more quantitative immunoassays. However, these immunoassays (such as enzyme linked imunosorbent assay (ELISA) and nephelometry) still apply several dilutions. Recently, time resolved fluoroimmunoassay, a highly sensitive method for the determination of IgA and IgM RF, has become available.8 This method measures RF as a continuous variable, with a wide range of measurement, in one single dilution. As a result, a matrix effect caused by different dilutions of patient serum can be avoided and reliability is improved. Because of its technical advantages, such as low background signal, high precision even at low positive concentrations (coefficient of variation <5%), large working range, and easy handling, time resolved fluoroimmunoassay provides a new possibility for investigating the role of RF in RA.8
In this study three questions on RF are examined:
•Can RFs be considered as parameters for disease activity in RA?
•What is the relation between RF and radiological damage due to RA, in groups of patients?
•Is there an individually determined relation between RF and radiological damage in single patients?
PATIENTS AND METHODS
This study is based on data from a large clinical trial comparing the combination of step down prednisolone, methotrexate, and sulfasalazine with sulfasalazine alone in early RA (the COBRA trial). This was a randomised, double blind, 56 week trial, with extended follow up. Nine centres in the Netherlands and one in Belgium participated. The study design has been reported extensively elsewhere.9 The relevant information for our study is summarised below.
Patients
Patients with RA (fulfilling the American College of Rheumatology criteria10) with disease duration of less than two years were selected. Included were patients with active disease, defined as the presence of at least six swollen joints and the presence of at least two of the following: nine or more tender joints, 45 minutes or longer early morning stiffness, or an ESR of at least 28 mm/1st h. Exclusion criteria were the use of corticosteroids or disease modifying antirheumatic drugs other than hydroxychloroquine, serious comorbidity, or recent major surgery. Patients were randomly split into two groups to receive either of the two treatment regimens.
Evaluation
A research nurse assessed patients first weekly, then every four weeks. An independent assessor evaluated them at baseline and then at 16, 28, 40, 56, and 80 weeks. Clinical measurements included ESR and CRP, SJC, tender joint counts (TJC),11 and doctor's and patient's global assessment (visual analogue scale). The original disease activity score was calculated from the TJC, SJC, ESR, and the patient's overall assessment.12
Radiographs of hands and feet were obtained at baseline and in weeks 28, 56, and 80. For this study the 28 week films were not used. Two independent observers scored the films according to the Sharp score, modified by van der Heijde (SHS).13 This method scores erosions and joint space narrowing in 44 joints of the hands and feet; the resulting total score is the sum of the erosion count and the joint space narrowing count (range 0–448).
Assessment of rheumatoid factor
Blood was drawn for determination of IgA RF and IgM RF at baseline and at 16, 28, 40, 56, and 80 weeks. All samples were tested with time resolved fluoroimmunoassay in a single laboratory. The IgM RF assay has been extensively described previously8; the IgA RF assay is performed identically. In summary, the assays are performed as follows: polystyrene microtitre plates are coated overnight with 2.5 μg rabbit IgG per well. Each well is incubated with 100 μl diluted serum (IgA RF 1:500, IgM RF 1:1600). Then 100 μl diluted tracer solution per well is added containing F(ab`)2 fragments of rabbit IgG against human IgA and IgM respectively, labelled with europium. After incubation for two hours, 200 μl of the so-called enhancement solution is added and time resolved fluorescence measured with the 1232 Delfia Fluorometer (Wallac, Finland). Between all steps the wells are washed with Tris buffer. For calibration the Dutch National Reference Preparation is used, which is calibrated against the International Reference Preparation of Rheumatoid Arthritis Serum (World Health Organization (WHO)). The cut off point for both IgM RF and IgA RF is 20 IU/ml. The range of measurement is 0–1500 IU/ml.
Analysis and statistics
Data are expressed as means (SD). Time integrated IgM RF and IgA RF, ESR, and CRP were determined by calculating the area under the curve (AUC). Variables without a normal distribution (CRP, RF, SHS, TJC, SJC) were normalised taking their natural logarithm (ln (x+1)). Differences between the two treatment groups were studied by t tests or Mann-Whitney tests, where appropriate. Pearson correlation coefficients (with 95% confidence intervals) expressed the relationships between disease activity parameters. To study the similarities between the disease activity parameters, they were visualised graphically as well. The relation between the baseline values (IgM RF, IgA RF, ESR, and CRP) and radiological joint damage (SHS) after 56 and 80 weeks was assessed by Pearson's correlation coefficients. The AUC of each disease activity parameter was correlated with SHS after 56 and 80 weeks and with the progression of SHS over 56 and 80 weeks. Multiple linear stepwise regression analysis assessed the contribution of each disease activity parameter to the final radiological outcome and to the progression of SHS. For this analysis, ESR, CRP, IgM RF, IgA RF, SJC, and TJC were included as independent variables.
The relation between time integrated RF and radiological progression in individual patients was assessed every six months. For each patient the slopes of this relation for each time period were calculated by dividing progression of SHS by time integrated RF. Non-parametric correlation coefficients between different time periods were determined.
Analyses were made for all patients, regardless of whether their RF levels were above or below the cut off point (20 IU/ml). In addition, all analyses were repeated comparing both treatment groups.
RESULTS
One hundred and fifty five patients were included in the trial. The results of the clinical trial have been discussed previously.9 Serum for laboratory assays was not available for all patients at all moments, owing to logistic reasons, but these were unrelated to centre or treatment group. ESR and CRP measurements were not available after 56 weeks.
The means and standard deviations of all disease activity parameters and radiological joint scores at baseline are shown. Randomisation led to prognostically similar treatment groups (table 1). IgM RF and IgA RF concentrations were slightly higher in the group receiving combination treatment, but the percentages of RF positive patients were similar in both treatment groups.
Clinical variables at baseline in the two treatment groups (mean (SD) unless indicated otherwise). There are no significant differences between the treatment groups
Levels of both RF assays were clearly associated with the other laboratory based disease activity parameters, (table 2, figs 1 and 2). The association between RFs and the clinical variables (TJC and SJC) was weaker. IgA RF and IgM RF performed equally well and were strongly interrelated. Correlation coefficients were similar in the two treatment groups (data not shown).
Correlation coefficients between clinical variables (95% confidence interval) at all times; p<0.01. Values are given for the whole group (n=155) because no differences were found between the two treatment groups

Pattern of changes over time of laboratory based disease activity parameters. Aggregated result of all patients receiving combination treatment (sulfasalazine, methotrexate, and prednisolone). IgM and IgA RF, IgM and IgA rheumatoid factor; ESR, erythrocyte sedimentation rate; CRP, C reactive protein.

Pattern of changes over time of laboratory based disease activity parameters. Aggregated result of all patients receiving sulfasalazine treatment. IgM and IgA RF, IgM and IgA rheumatoid factor; ESR, erythrocyte sedimentation rate; CRP, C reactive protein.
The correlation between laboratory based disease activity parameters at baseline and SHS at 56 and 80 weeks was moderate but statistically significant; the correlation of these disease activity parameters at baseline with the progression of radiological damage from baseline was stronger than with the absolute radiographic score (table 3). Exposure to disease activity, as measured by time integration (AUC) of laboratory based disease activity parameters, was significantly correlated with the SHS; correlations with progression of SHS were even stronger (table 4). These associations were less pronounced for both RF tests than for ESR and CRP, as is shown by the lower correlation coefficients in tables 3 and 4; time integrated (but not baseline) IgA RF tended to perform slightly better than IgM RF, but this was not statistically significant.
Correlation coefficients between clinical variables at baseline and radiological scores; p<0.05, *p<0.01, †not significant. Values are given for the whole group (n=155), except wherever significant differences were found between the two treatment groups
Correlation coefficients between time integrated clinical variables and radiological scores; p<0.05, *p<0.01, NS=not significant. Values are given for the whole group (n=155) because no differences were found between the two treatment groups
Nearly all associations were similar in the two treatment groups; only baseline ESR correlated more strongly with (progression of) SHS at 56 weeks in the sulfasalazine group than in the combination group. In the determination of the relative contribution of disease activity parameters to the SHS in the whole group, ESR was the most predictive, in addition to treatment modality, and time integrated SJC (explained variance of the SHS value at 56 weeks and of the progression of SHS from baseline until 56 weeks: 22.8% and 37.0% respectively (multiple linear backward stepwise regression analysis)). For the SHS at 56 weeks baseline ESR was more important, whereas time integrated ESR was more important for the SHS progression from baseline until 56 weeks. The determinants of the SHS were identical in the sulfasalazine and combination treatment groups, although the explained variances differed: 33.3% v 11.1% for the SHS at 56 weeks, and 37.9% v 28.7% for the SHS progression from baseline until 56 weeks, respectively.
For each individual patient, the relation between time integrated RF and x ray progression was visualised at six-monthly intervals (fig 3). Every patient seemed to follow an individual line. The calculated slopes of the individual lines in every six-month time interval were highly correlated with each other (0.57–0.68; p<0.01). The same analysis was done for the other disease activity parameters. Comparable results were found for every disease activity parameter (correlation coefficients 0.61–0.62; p<0.01), suggesting a relatively constant, individual relationship between the exposure to disease activity and the progression of radiological damage.
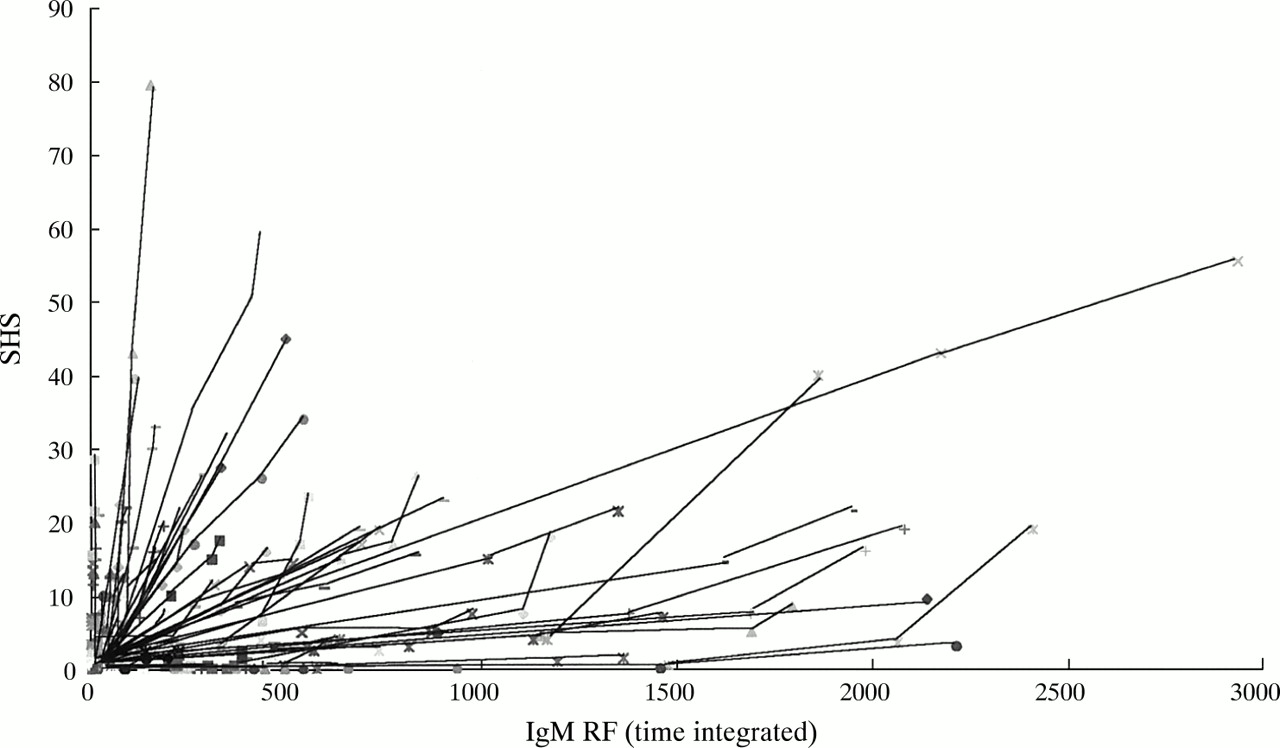
Individual relation between exposure to disease activity (time integrated IgM rheumatoid factor (IgM RF)) and radiological damage (Sharp score, modification van der Heijde (SHS)). Every patient has his/her own line, composed of the consecutive six month values for time integrated IgM RF in relation to the SHS.
DISCUSSION
This study shows that RF levels reflect disease activity in patients with RA. Moreover, a linear relation between time integrated RFs and progression of radiological damage exists in individual patients. A similar, fairly constant slope between exposure to disease activity over time and radiological progression was found for other laboratory based parameters also.
Preceding studies have provided conflicting results as to whether RF is a parameter for disease activity in RA. Cross sectional studies showed stronger correlations between RF and disease activity parameters14–19 than prospective studies.3,4,20 Two of the prospective studies measured RF titres and disease parameters simultaneously. Van Leeuwen et al found good correlations between RF titres and both the CRP and the number of swollen joints.4 In contrast, Eberhardt et al demonstrated a significant correlation between RF and CRP, but not ESR.3 In most of the studies, the interrelation between IgM and IgA RF was highly significant,2–4,14–16 as in the present study. Our data show a correlation between RF and various disease activity parameters, especially the laboratory based parameters. Moreover, the changes over time of RF and laboratory based disease activity parameters were comparable. In addition to the abovementioned studies, this further illustrates the value of RF as disease activity parameter.
The association of disease activity parameters with radiological outcome in patients with RA was demonstrated in two ways. Firstly, baseline RF (as well as CRP and ESR) turned out to be related to subsequent radiological damage, in accordance with earlier studies.4,5 Secondly, time integrated disease activity parameters were even more strongly related to radiological damage than the baseline disease activity parameters. Disease outcome is thought to be the result of the exposure to disease activity over time, rather than the result of initial disease activity. In one preceding study, time integrated IgM RF correlated significantly with radiological progression after three years (correlation coefficient 0.29).4 Our study showed comparable, though slightly lower, correlation coefficients for IgM RF and IgA RF; this is probably explained by the shorter follow up. Additionally, our data showed that time integrated CRP as well as ESR had a stronger association with radiographic damage than did time integrated RFs, emphasising the comparable results in Van Leeuwen's study. In accordance, multivariate analysis showed that ESR is the most important determinant of SHS. The SJC was found to be a moderately additive determinant for the SHS progression. Thus, for clinical practice, RF values do not add information to that received from the ESR.
In the present study, the values of IgA RF and IgM RF as disease activity parameters were comparable. However, IgA RF tended to be more correlated with radiographic damage than IgM RF. Only a few studies have directly compared both RFs, with some of them favouring IgA RF,2,20 but others IgM RF.4,15,17
The individual, linear relation between time integrated disease activity parameters and progression of radiological damage is in accordance with the earlier demonstrated relation between time integrated CRP and radiographic damage in individual patients.7Although the slope of the line can vary between patients, it is constant for the individual. Our hypothesis, based on the results of our study, is that treatment can change the position on the line, but not its slope. The imaginary patient in fig 4 illustrates that exposure to disease activity A1 in a given time period will lead to radiological damage A2; however, if disease activity were reduced (B1) in the same period (for example, by intensive treatment), radiological damage would be less (B2). Thus, the slope of the curve does not change for the individual but his/her position on the curve will be different with different exposure to disease activity. Knowledge of the slope (α) of the individual line would identify those patients who will need aggressive treatment to suppress disease activity (high slopes=large α) from those who will do well with mild treatment (low slopes=small α). Our hypothesis that treatment does not change the slope of the curve is supported by the comparable correlation coefficients in the two treatment groups.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Relation between exposure to disease activity and radiological damage in the individual patient. The slope of the curve (α ) is individually constant but can vary between patients.
Most previous studies on the possible role of RF as a disease activity parameter used qualitative (positive v negative) RF tests or semiquantitative tests. Even with the ELISA technique, several dilution steps are necessary for the determination of RFs in the higher ranges. Fluoroimmunoassay has two major advantages over ELISA.8 Firstly, it is a very sensitive method, allowing the sera to be diluted strongly only once. The influence of other immunoglobulins that react with rabbit IgG is thus limited to the minimum. Secondly, a wide range of RF values can be determined in one assay, so it is not necessary to use different solutions. This makes the assay more reliable. In an earlier study, the results of an ELISA corresponded well with those of fluoroimmunoassay.8 The improved properties of this RF assay have helped in the examination of the relation between RF concentration and disease activity and also the relation between RF concentration and disease outcome.
In conclusion, both IgA RF and IgM RF can be considered as disease activity parameters. All disease activity parameters, including RFs, are associated with radiological damage. Most importantly, there seems to be an individually determined, linear relationship between exposure to disease activity and progression of radiological damage. Understanding this relation between disease activity and outcome in individual patients is relevant for the management of patients with RA.