Article Text

Abstract
Objective: To investigate whether alleviation of knee pain influences quadriceps function, proprioceptive acuity, and postural stability in patients with knee osteoarthritis (OA).
Methods: A crossover, within-subject, double blind study design involving 68 subjects with painful knee OA. Each subject received an intra-articular injection into one or both knees (both if symptomatic) of either 5 ml 0.5% bupivacaine or 5 ml 0.9% saline. Two weeks later they received an injection of the alternative agent. Subjects and observer were unaware of the order of injection, which was randomly assigned. Knee pain (100 mm visual analogue scale), static postural sway, knee proprioceptive acuity, maximum voluntary contraction (MVC), and percentage activation of the quadriceps were assessed immediately before and one hour after each injection.
Results: Significant pain reduction was achieved one hour post-bupivacaine (mean difference as a percentage change 56.85, 95% CI 31.01 to 73.65; p<0.001) and post-saline (mean difference as a percentage change 41.94, 95% CI 11.57 to 76.66; p< 0.001), with no significant difference between the two. Both MVC and activation increased significantly post-bupivacaine (mean percentage differences 18.83, 95% CI −31.79 to −0.26, and −11.90, 95% CI −39.53 to 2.97, respectively; both p<0.001) and post-saline (mean percentage differences −7.64, 95% CI −21.96 to 4.73, and −10.71, 95% CI −25.19 to 2.60 respectively; both p<0.001). Proprioception worsened after bupivacaine (mean percentage difference −28.15%, 95% CI −83.47 to 19.74; p=0.009), but there was no effect on postural sway; saline injection had no effects. There was no order effect, and comparison of median percentage changes showed no significant differences between injections for change in MVC, activation, proprioception, or sway.
Conclusion: Reduction in knee pain through either peripheral (local anaesthetic) or central (placebo) mechanisms resulted in increased MVC. This increase, however, did not result in improvements in proprioception or static postural stability, suggesting that other mechanisms play a part in these functions, at least in this acute model.
- knee osteoarthritis
- bupivacaine
- postural sway
- quadriceps strength
- MVC, maximal voluntary contraction
- OA, osteoarthritis
- VAS, visual analogue scale
Statistics from Altmetric.com
Knee pain is a major symptom of knee osteoarthritis (OA), and the presence and severity of knee pain are important determinants of disability.1–4 Data from the prospective NHANES-1 study show that knee pain at baseline is associated with increased risk of difficulty with walking later in life, irrespective of baseline radiographic change.5 Pain is also a risk factor for radiographic progression of knee OA and for the need for joint replacement.6
The origin of pain in OA remains unclear, therefore the relationship of pain with other important physiological variables is worthy of exploration. Cartilage is aneural, but other joint tissues possess pain receptors and are potential sites for pain sensation. Kellgren proposed at least three clinical pain patterns that may be associated with different anatomical origins7: ligamentous and muscular pain, synovial pain, and pain resulting from a disordered joint. Histological studies of periarticular tissues confirm the presence of a diffuse network of nociceptors scattered throughout the fibrous capsule, ligaments, tendons, articular fat pads, synovium, periosteum, and muscle.8,9 The afferents of these nociceptors are thin myelinated (Aδ) and non-myelinated (C) fibres (that is, both of relatively fast or slow conduction velocities). Several mechanisms of pain in knee OA have been suggested. These include mechanical strain on nociceptors from heavy local pressure or joint movement, nociceptor irritation by inflammatory mediators,9 muscle contraction, quadriceps weakness, and effusion.10
Muscle has important sensorimotor functions for controlled joint movement. Pain may be detrimental to either the motor (movement, strength, activation) or sensory (proprioception, balance) components of muscle function. Electromyographic studies show that painful knee OA is associated with an increase in quadriceps activity that is thought to result from abnormal discharge of afferents from muscle, tendon, and joint receptors.11,12 Furthermore, young subjects with activity related knee pain but no apparent structural abnormality have been reported to have gait abnormality, striking the floor with greater impact and showing larger angular accelerations during swing through. This “microklutziness” is thought to result from neuromuscular incoordination and, possibly, to predispose to later development of OA.13
We have previously shown that subjects with knee OA have increased static postural sway in both lateral and anteroposterior directions, reduced knee proprioception, and reduced maximal voluntary contraction (MVC) and activation of the quadriceps muscle compared with age matched non-OA controls.14 One of the explanatory factors for the variation of sway in OA subjects was the severity of knee pain. The objectives of the present study were to investigate the effects of short term alleviation of knee pain on the reduced quadriceps function and knee proprioceptive acuity associated with OA. It was suggested that any improvement in one or both of these parameters would improve the impaired static postural stability of these subjects. We selected intra-articular injection of local anaesthetic (5 ml 0.25% bupivacaine) to achieve analgesia because this has previously been shown to reduce knee pain in subjects with knee OA significantly, and sometimes completely, one hour after injection.15 In case the anaesthetic had any direct effects on knee physiology other than the indirect effects that may result from pain alleviation we additionally investigated the effects of intra-articular saline (placebo) injection in the same subjects. There is no theoretical reason why such an injection might influence peripheral nerve fibre function.
METHODS
Approval for the study was obtained from the local research ethics committee. Informed written consent was obtained from all patients.
Patients and study design
Patients were recruited from a knee clinic at the City Hospital, Nottingham. All had symptoms and signs consistent with knee OA and radiographic evidence of definite osteophyte together with definite joint space narrowing affecting at least one compartment (medial tibiofemoral or patellofemoral, or both) viewed on standard radiographs (standing extended anteroposterior and skyline 30° flexion views). No patient had symptoms, signs, or x ray findings to suggest coexistent inflammatory or other locomotor disease, and no patient had a history of faints, vertigo, diabetes mellitus, Parkinsonism, or other condition that may impair balance. Patients had to have current pain in at least one knee measuring at least 20 mm on a visual analogue scale (VAS) for usage, rest, or night pain, where 0 mm = no pain and 100 mm = worst pain imaginable.
A crossover, within-subject, double blind design was employed. Each patient received intra-articular injection of either 5 ml 0.5% bupivacaine or 5 ml 0.9% saline into one or both knees (both if both painful). Two weeks later they were injected with the alternative agent (both knees if painful). The order was randomly assigned (computer generated, blocks of 10) and injections were given by an independent operator to maintain blinding for patients and assessor. At each injection, aspiration was undertaken (to aid confirmation of correct needle placement), but no more than 5 ml of synovial fluid was removed. Assessments were undertaken immediately before (baseline) and one hour after each injection, specifically: static postural sway; proprioception; MVC and quadriceps activation; and self reported knee pain (current knee pain) using a 100 mm VAS.16 During the hour between injection and assessment the patient's activity was not restricted: they were permitted to walk around the unit, though most chose to be relatively inactive and await the second assessment. A third assessment was undertaken two weeks after the second injection to assess the duration of any treatment effect on pain relief.
Assessments
Postural sway
Static postural stability was assessed with the Balance Performance Monitor (SMS Sanders Healthcare, Harlow, Essex CM19 5TL, UK). The machine is designed to assess upright weightbearing status and comprises two foot-plates connected to a feedback unit. For each subject the position of the foot-plates was adjusted to match their normal stance. They were then asked to stand steadily on the foot-plates with their shoes on, arms at their sides, and eyes closed. The procedure was performed twice, the first for acclimatisation and the second for measurement. Data were acquired at 10 Hz over 30 seconds and presented both graphically and numerically. Graphical information presented a trace as the subject's weight shifted in lateral and anteroposterior directions, and as a centre of gravity trace, indicating the movement of the subject's centre of balance about their base of support during the 30 seconds. The Balance Performance Monitor data are recorded in arbitrary units on a scale from 0 to 100, from which it is possible to derive values of weight distribution (balance coefficient) and relative movement (sway coefficient). The balance coefficient is the mean weight that shifts during the 30 seconds of the test in a left-right or lateral direction, and a sway coefficient is the standard deviation of the balance coefficient. Greater balance and sway coefficients indicate greater postural instability. Reproducibility assessed by repeat measurement of postural sway on two occasions one week apart (10 knee OA and 10 normal subjects) was shown to be good (α=0.87; intraclass correlation 0.87, 95% CI 0.68 to 0.95).14
Knee joint proprioception
Proprioceptive acuity was assessed by the ability to reproduce passive positioning of the leg with eyes closed using custom designed apparatus based on published descriptions.17–20 The apparatus comprised a chair with a device that allowed passive positioning of the subject's leg; a protractor with one-degree divisions attached to the side of the chair, a counterbalance to the weight of the subject to ensure that the leg felt weightless during leg movements, and inflatable pneumatic cuffs (Centromed, Ashford, Kent TN24 0SJ, UK) for the thigh and lower leg to eliminate any contribution from cutaneous receptors and to avoid skin contact with clothing. Each subject was seated on the chair with hips and knees at 90° flexion. The upper pneumatic cuff was placed around the whole thigh from just above the knee and the lower cuff around the whole foot and calf from just below the knee. The following procedure was then performed with eyes closed and hands folded across the chest. The leg was moved passively to a randomly determined position (the criterion angle) and held there for five seconds. The leg was then returned passively to the original position and the subject asked to actively reproduce the criterion angle. Criterion angles were randomly selected between 90° flexion and full extension. The difference between the criterion and reproduced angle was taken as a measure of proprioceptive acuity. The procedure was performed four times, the first purely for acclimatisation. The average of the last three trials was regarded as the proprioceptive acuity for that limb. Reproducibility assessed by repeat measures on two occasions one week apart (10 knee OA and 10 normal subjects) was shown to be good (α=0.90; intraclass correlation 0.89, 95% CI 0.74 to 0.96).14
Maximal voluntary contraction (MVC) and percentage activation of the quadriceps
Quadriceps strength was measured isometrically using a modified Tornvall chair. Each subject sat on the chair with hips and knees flexed to 90°. Restraining straps across the pelvis and chest minimised unwanted pelvic and trunk movements. A non-extensile strap was placed just above the medial malleolus with the other end connected by a chain to a strain gauge (TKA load cell Techni Measure, Studley) attached to the back of the chair giving a horizontal line of pull. The strain gauge output was amplified by an amplifier and digital reader (Techni Measure, Studley) and relayed onto a chart recorder (Recorderlab, Surrey SM2 5PS). Each subject was asked to push as hard as possible against the strap to try to straighten the leg. This was performed three times with a few seconds rest between, and the highest value was taken as the MVC. The degree of activation was estimated by superimposing an electrical current given through two aluminium foil electrodes covered in cloth dampened in 0.9% saline and placed on the anterior thigh.21,22 Stimulation was achieved using a Digitimer High Voltage Stimulator (DS7-H, Digitimer Ltd, Welwyn Garden City) set to deliver a 1 A current of 50 ms duration. The voltage was adjusted to achieve about 20% activation and the subject was given a set of three stimulations at rest (baseline “twitches”) and was then asked to sustain a maximal contraction while three further currents were delivered at one second intervals. The percentage activation was calculated according to Bigland-Ritchie et al.23 Reproducibility of this instrument for quadriceps MVC and activation has previously been established in our unit.21
Statistical analysis
For a crossover study design we calculated that a sample size of 68 would have 90% power to show an improvement of postural sway at 0.05 significance. This was chosen as a function measure rather than the reduction of pain because it is known that pain reduction can be obtained through placebo.15 It was not the intention of the study to predict the change in postural sway from the other variables measured. Values for proprioceptive acuity, MVC, quadriceps activation, and knee pain were given as the mean of the values for right and left knees if both knees were injected, or as the value for the single knee if only one knee was injected (that is, one value for each person). Statistical analysis was performed using SPSS, version 10.1. All tests are two tailed. For non-parametric variables, data are presented as medians and interquartile ranges, and the Mann-Whitney U test used to assess differences. Carryover effect was calculated according to Hills and Armitage.24
RESULTS
Although 72 patients with knee OA were recruited into the study, four were unable to complete the study owing to illness or election to leave the study. The remaining 68 patients completed the protocol (49 women, 19 men; mean age 66.6 (range 36–87); mean weight 80.5 kg (range 53–134); mean height 165.6 cm (range 150–187)), though four declined to have twitch superimposition. Bilateral injections were given, on both occasions, to 48 of the 68 patients because of bilateral symptoms. Table 1 shows the distribution of anthropometric data. Table 2 shows the data for pain, postural sway, proprioception, MVC, and percentage activation. The data obtained from the study were analysed in the following steps.
Descriptive statistics for age, weight, and height of participants (n=68) and for men (n=19) and women (n=49) separately
The results (median and IQR) for each of the test variables before and after each intervention
Pain reduction by bupivacaine and placebo
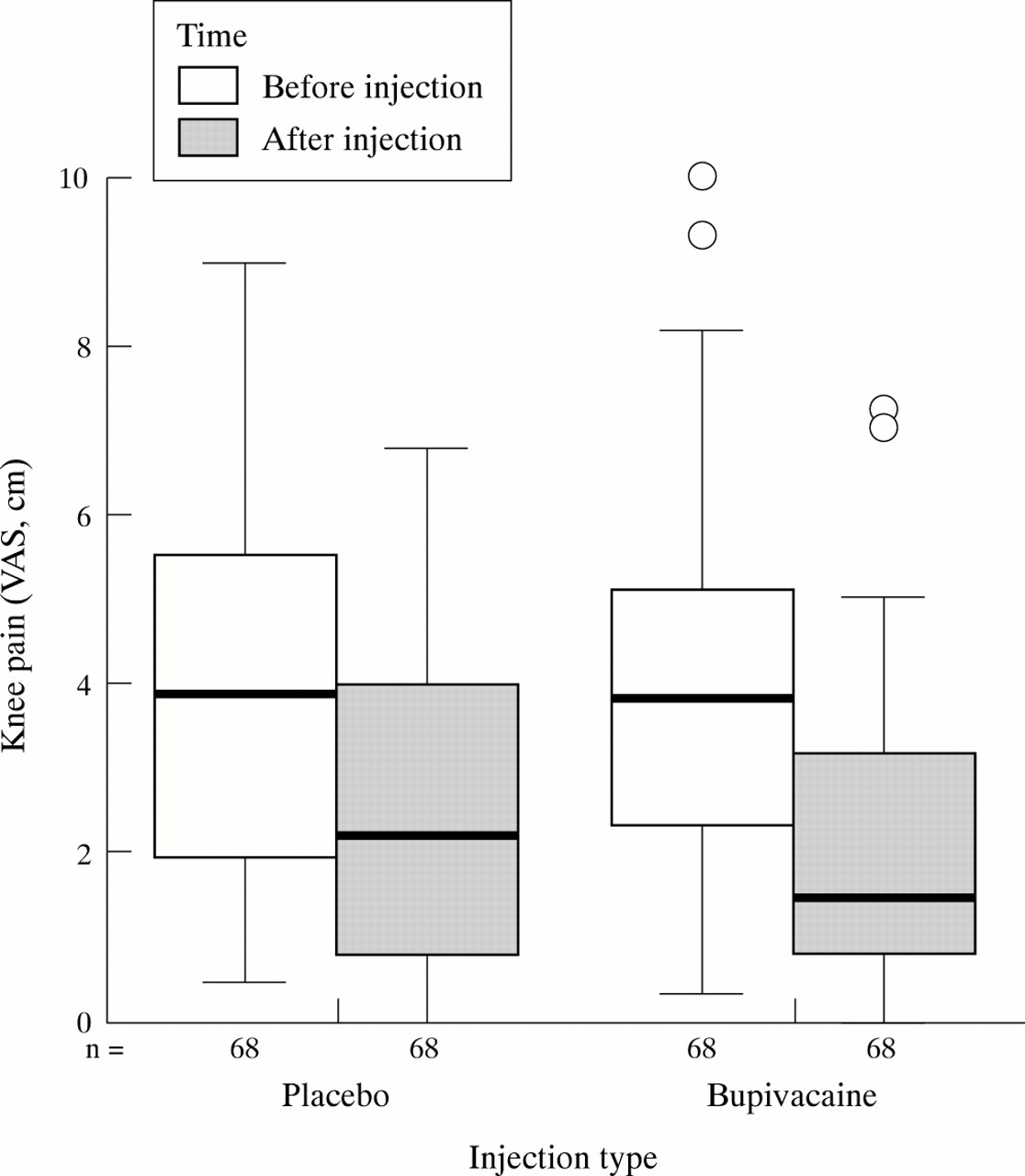
We first examined whether injection of bupivacaine or placebo reduced knee pain and whether there was a significant difference between them. Injection of either agent resulted in marked reduction in pain (both p<0.001), bupivacaine giving a median of 56.85% and placebo a median of 41.94% reduction in pain one hour after injection (fig 1, table 3). There was no significant difference between the two.
The percentage change (median and IQR) for each of the test variables for placebo and bupivacaine interventions

Knee pain (median VAS, cm) immediately before and one hour after intra-articular injection of placebo and bupivacaine.
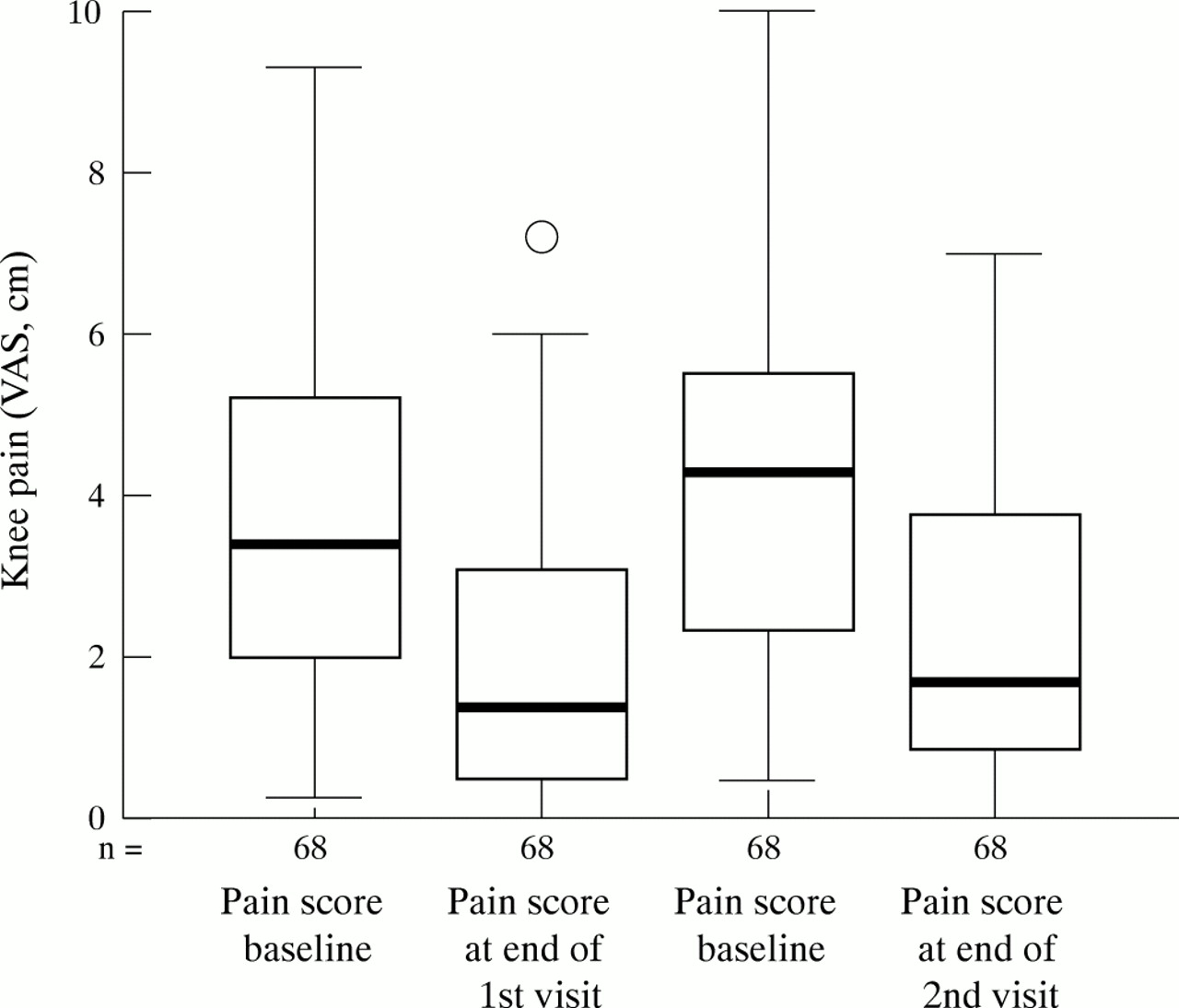
One concern with analysis of crossover trials is the possibility of a carryover effect between the two visits (period effect). The other concern is that there may be an effect of order of intervention (treatment period interaction). None of the data were normally distributed so non-parametric tests were used to investigate either of these possibilities before any further investigation of the data.
Because the abolition of pain was a primary intervention, change in pain was used as the variable to assess these potentially confounding factors. If there were a period effect then the change in pain reduction on the second visit would be different from the pain reduction on the first visit irrespective of the actual intervention. There was found to be no significant difference (Z=−0.42, p=0.966) (fig 2).

Knee pain before and after intervention for the first and second visit, irrespective of the intervention received.
To investigate the possibility of treatment period interaction the mean changes in pain scores irrespective of intervention were compared with intervention order. Again no significant interaction was found (Z=−0.798, p=0.425).
The scores are therefore independent and the effect of the two interventions can be safely compared. To appreciate the effects of the intervention the extent of change is shown as percentage change from the baseline measurement (tables 3 and 4).
Comparison of the percentage change between interventions for each of the test variables
Bupivacaine and placebo models
We next examined the changes in postural sway, proprioception, MVC, and quadriceps activation that were associated with injection of either bupivacaine or saline (tables 3 and 4).
Neither intervention produced a significant alteration in postural sway. In fact placebo produced a greater effect (median −9.90, IQR −27.99 to 22.24; p=0.41) than bupivacaine (median 0.00, IQR −27.03 to 23.33; p=0.81), though there was no significant difference between the two effects (table 4, fig 3).
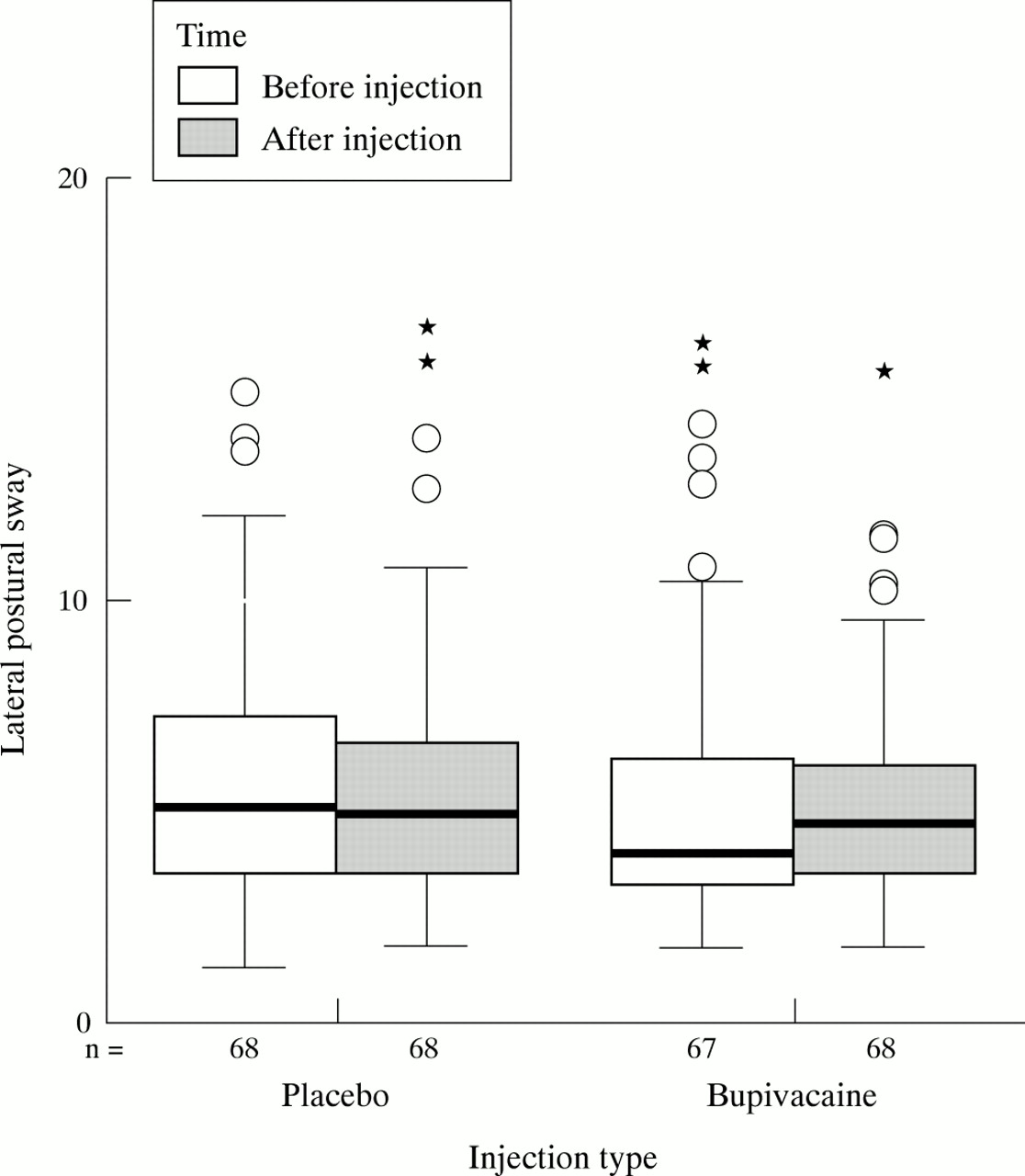
Lateral postural sway immediately before and one hour after intra-articular injection of placebo and bupivacaine.
Proprioceptive acuity was adversely affected by both interventions but only the effect of bupivacaine was significant (median for placebo −10.26, IQR −35.91 to 24.82, p=0.18; median for bupivacaine −28.15, IQR −83.47 to 19.74, p= 0.009). However, there was no significant difference in percentage change between the two (table 4, fig 4).

Proprioceptive acuity (degrees) immediately before and one hour after intra-articular injection of placebo and bupivacaine.
MVC improved for both interventions (table 3, fig 5). The improvement for placebo (median −7.64, IQR −21.96 to 4.73) was significant (p=0.004), as was the bupivacaine (median −18.83, IQR −31.79 to −0.26, p<.001). The difference between the two interventions was substantial, but only approached significance (p=0.057).

Maximum voluntary contraction (kgF) immediately before and one hour after intra-articular injection of placebo and bupivacaine.
The extent of activation of the quadriceps groups showed a significant improvement (p<0.001) (table 3) in both interventions (placebo: median −10.71, IQR −25.19 to 2.60; bupivacaine: median −11.90, IQR −39.53 to 2.97), but there was no significant difference in effect between the two (table 4, fig 6).
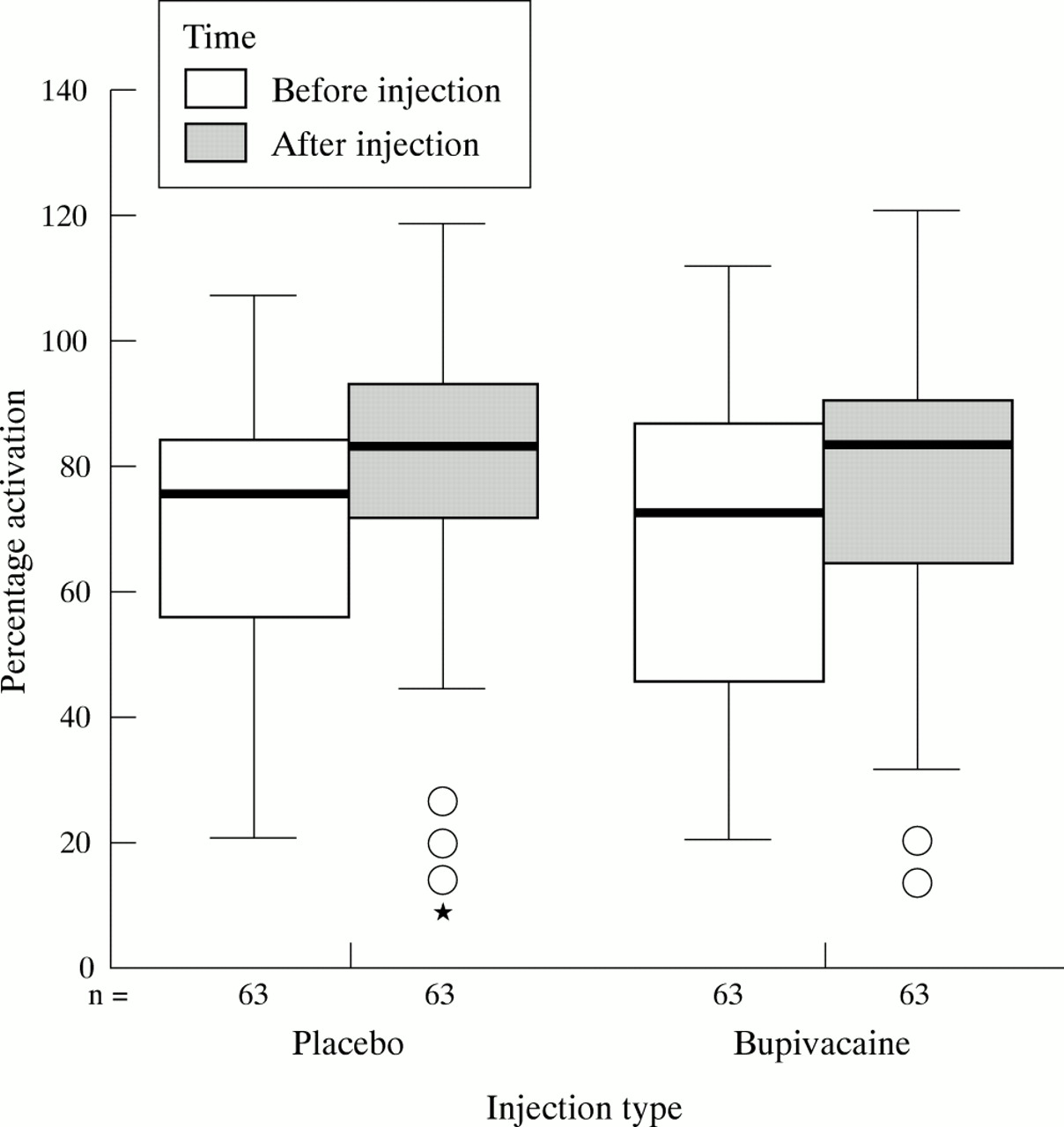
Percentage activation immediately before and one hour after intra-articular injection of placebo and bupivacaine.
Final versus baseline assessments
At the final (third) visit knee pain had returned to approximately the same as at baseline for the first and second visit, irrespective of which intervention was performed, and was not significantly different from either the first or second visit (p=0.18 and p=0.98, respectively) (fig 7).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Knee pain (median VAS, cm) at baseline assessment for each of the three visits, irrespective of intervention.
DISCUSSION
An important requirement for this study was the successful alleviation of knee pain. This was achieved through intra-articular injection of both placebo and bupivacaine. Although not specifically designed for this purpose, our study incidentally confirms the dramatic short term benefit of bupivacaine. This accords with one previous study comparing bupivacaine with placebo in 20 patients with bilateral painful knee OA.15 In contrast with that study, however, we also obtained dramatic pain relief by injection of placebo (saline) which was not significantly different from that obtained by bupivacaine. However, neither pain relieving effect was long lasting. This discordance between studies may relate to differences both in patient characteristics and trial design. There exists the possibility that a portion of the pain relief may be attributable to the aspiration of the joint at the time of injection, but we think that this is unlikely given the very small amounts of fluid aspirated and the low number of patients to whom this applied. Although age and sex distribution were similar in both studies, initial pain severity was greater in the previous study, perhaps making a placebo response harder to achieve. We also used a within-patient rather than parallel group design, included a larger number of patients, and gave injections to both knees, if symptomatic, rather than to the single most painful knee. This last approach, though rarely used, has been recommended for OA studies using local rather than systemic methods of pain relief because pain experience on one side may modify pain reporting on the other.25 The placebo response, including for pain, is a well recognised phenomenon,26,27 its prevalence and magnitude varying according to factors such as diagnosis, treatment modality, route of administration, and expectations of the patient and doctor. Although ill understood it is thought to involve central, not peripheral, mechanisms of pain modulation, with release of endogenous opioids being particularly implicated.26 For the purposes of our study, however, the striking effects of both injected agents allowed us to study the physiological consequences of pain alleviation achieved through either peripheral (local anaesthetic) or central (placebo) mechanisms.
Temporary reduction in knee pain after injection of either bupivacaine or saline was clearly associated with an increase in quadriceps MVC and activation. Patients therefore exerted more force and used more fibres when their pain was less. There are two principal explanations for such an association. Firstly, patients might consciously push harder when their pain is less severe. Secondly, reduction in pain may reduce pain-induced reflex inhibition of the quadriceps. Such “reflex arthrogenous muscle inhibition” is said to account for the selective quadriceps dysfunction and weakness seen in subjects with knee OA or other knee disease.28–34 Although arthrogenous inhibition can occur independently of pain,31 it appears to relate primarily to pain in the situation of knee OA. Jones demonstrated quadriceps inhibition in approximately one third of subjects with knee OA and found local joint line tenderness and anxiety to be the only independent predictors of such inhibition.21 Apart from any effects mediated through analgesia it is conceivable that an anaesthetic effect of bupivacaine on α motor neurones might diminish arthrogenous inhibition. Such an effect, however, seems unlikely. Small pain fibres are preferentially blocked by bupivacaine before larger fibres for cold, heat, touch, and deep pressure,31 and intra-articular injection of 10 ml 1% lidocaine or 10 ml 0.5% bupivacaine31 both reduce knee pain without affecting arthrogenous inhibition. Furthermore, the similar findings in the placebo model strongly support the interpretation that reduction in knee pain, by either peripheral or central mechanisms, is primarily responsible for the improvement in muscle function observed.
Pain relief through intra-articular bupivacaine resulted in a worsening of proprioception (increase in disparity from criterion angle), whereas pain relief from saline had no obvious effect on proprioception, even though muscle strength was improved in all subjects. The worsening following bupivacaine injection presumably resulted from direct inhibition of the intra-articular neuroreceptors that convey proprioception. Thus although bupivacaine is thought to act preferentially on pain fibres, it still exerted a measurable inhibitory effect at the dose used. A further possibility is that some subjects may use pain sensation to gauge the position of the criterion angle, and alleviation of pain might thus impair proprioceptive acuity. Against this, however, is the lack of effect from similar, though less dramatic, pain relief after saline injection. The fact that proprioception did not improve after pain reduction and improvement in muscle (motor) function suggests that impaired proprioception in knee OA primarily results from factors other than pain—for example, reduction in numbers or damage to mechanoreceptors as a result of the OA process. A similar explanation has been proposed for the impaired knee proprioception seen in asymptomatic elderly patients compared with younger subjects.19,35
In neither the bupivacaine nor placebo models were we able to demonstrate any effects on postural sway through reducing pain and increasing strength. Muscle strength is clearly important for balance control. The fact that an increase in quadriceps MVC was not coupled with increased postural stability suggests either that our measure of sway was insensitive (resulting in a β error) or that other mechanisms that are uninfluenced by pain and are independent of quadriceps strength are more important in postural control. Control of both static and dynamic balance requires the coordinated action of multiple muscles. Possibly, subjects with knee OA have weakness of other muscles, such as hamstrings, calf, or trunk muscles, which is less influenced than the quadriceps by the reduction in pain obtained in this study. Furthermore, certain dysfunction caused by the OA process may not be readily reversed by pain alleviation but require retraining over a prolonged time for any improvement in function to occur.
There are several caveats to our study. Firstly, the pain relief we obtained was relatively short and longer periods of pain relief might allow better accommodation of pathophysiological changes associated with knee OA and thus different observed outcomes. Secondly, all our subjects had radiographic changes of knee OA so it was not possible to differentiate the effects of pain from the structural effects of the OA process. Further studies of subjects with knee pain with a range of radiographic structural change, some even with no structural change, are warranted. Also, although muscle weakness is reported to be a localised phenomenon,21 it would be interesting to examine the strength of calf muscles in subjects with knee OA, their role in the maintenance of static postural control, and whether their strengthening leads to improvement in postural stability. Whether quadriceps exercise improves knee proprioception and postural sway in patients with knee OA, as has been shown in subjects with anterior cruciate ligament insufficiency,36,37 also merits study.
In conclusion, reduction in knee pain through either peripheral (local anaesthetic) or central (placebo) mechanisms resulted in a rapid improvement in MVC of the quadriceps muscle in patients with knee OA. This improvement, however, was not accompanied by any improvement in the impaired proprioception and static postural stability that occurs in such subjects. Further studies are required to determine the more relevant and possibly reversible factors that cause impaired postural sway in patients with knee OA.
Acknowledgments
We are indebted to all the patients who participated in the study and to Drs Adrian Jones and Richard Hubbard for advice on statistical analysis.