Article Text

Abstract
Background: Rice bodies can occur in the joints in many rheumatic conditions, but they are most common in rheumatoid arthritis. They are generally believed to occur rarely in patients with osteoarthritis, but one study reported rice bodies with apatite crystals.
Objective: To report on a series of joint fluids with rice bodies containing apatite clumps and examine their clinical pictures.
Methods: All synovial fluid analysis reports for 10 years were reviewed for rice bodies and eight patients were reported on. A series of patients with a variety of diseases with synovial fluid rice bodies found to contain calcific material is described. All were examined by compensated polarised light and alizarin red stain, and four were examined by electron microscopy.
Results: The eight patients all had alizarin red S chunks embedded throughout the rice body. Transmission electron microscopy disclosed the presence of a matrix of collagen, fibrin, and amorphous materials containing typical apatite crystals. Clinical diagnoses, radiographic findings, and leucocyte counts varied, but six of the eight patients had had previous repeated corticosteroid injections into the joints.
Conclusion: Aggregates of apatites may be more common than previously recognised in rice bodies as they are not routinely sought. Whether they are a result of joint damage or depot steroid injections and whether that might contribute to further joint injury now needs to be investigated.
- calcium apatite
- synovial fluid
- rice bodies
- CPPD, calcium pyrophosphate dihydrate
- OA, osteoarthritis
- RA, rheumatoid arthritis
- SF, synovial fluid
Statistics from Altmetric.com
Grossly visible bodies resembling polished rice in synovial fluid (SF) have been called rice bodies. These were originally associated with tuberculous arthritis about a century ago. Subsequently, several reports have described their occurrence in juvenile rheumatoid arthritis,1 septic arthritis,2 hypocomplementaemic arthritis,3 subacromial bursitis,4,5 and, most commonly, in rheumatoid arthritis (RA).2,6–9 Rice bodies are rare in patients believed to have only osteoarthritis (OA).
There has been one report on four patients with OA who all presented with non-inflammatory synovial fluid and rice bodies containing calcium apatite crystals, with two of the patients also having calcium pyrophosphate dihydrate (CPPD) crystals.10 No other reports on synovial fluid rice bodies have thus far mentioned the presence of crystals. Previous reports on rice bodies have either not examined them for calcium crystals or not commented on this. We have begun to determine how often these rice bodies contain crystals and what implications this may have for disease pathogenesis or clinical features.
We report our experience with eight patients, in whom synovial fluid rice bodies were associated with calcium hydroxyapatite crystals seen on light and electron microscopy and/or x ray powder diffraction studies.
METHODS
These eight synovial fluids were all sent to the rheumatology service at the Hospital of the University of Pennsylvania or Philadelphia VA Medical Center for evaluation. The fluids described were seen over 10 years and represent about 50% of all fluids with rice bodies and less than 0.1% of several thousand joint fluids examined. The specimens were all promptly evaluated on the same day they were received. Cells were counted using a standard leucocyte counting chamber.11 All specimens were likewise examined using compensated polarised light microscopy and stained with alizarin red S.12 Electron microscopy was performed in four cases using standard techniques in use in our laboratory.11–13
RESULTS
Table 1 summarises the clinical characteristics of the eight patients. Six patients were male and two female, with a median age of 55 years (range 5–75 years). Diagnoses included were RA (n=5), camptodactyly arthritis syndrome (n=1), OA (n=1), and septic bursitis (n=1). The most commonly involved joint was the knee, which was affected in four cases, the shoulder joint in two cases, and subacromial bursa and proximal interphalangeal joint in one case each. Six patients had a history of multiple intra-articular steroid injections of the affected joint because of refractory pain and swelling. Radiographic findings available for some of the patients were mostly compatible with changes of OA (table 1).
Clinical summary of patients with synovial fluid calcium crystals in rice bodies
In these fluids with apatite containing rice bodies, synovial fluid leucocyte counts ranged from 0.05 to 45.8×109 cells/l with a mean count of 11.0×109 cells/l. Patients 4 and 5 had undergone arthroscopic lavage of their knees from which the synovial fluids with the rice bodies were obtained.
All rice bodies in these eight specimens contained shiny irregular 1–15 μm chunks that stained strongly with alizarin red S and were thus highly suggestive of clumps of apatite crystals (fig 1). Calcium stains such as alizarin red S, have been used to screen for hydroxyapatite and other calcium containing crystals in synovial effusions and joint tissues. Although the method is sensitive, it is non-specific for calcium phosphate, and may give false positive results with CPPD, calcium oxalate, and other calcium containing compounds12 and, occasionally, with other metals. Smaller amounts of alizarin positive clumps were seen outside the rice bodies in three cases; these were not analysed further. Routine light microscopy in two of the cases showed additionally, the presence of rod-shaped crystals which were positively birefringent under polarised light and thus characteristic of CPPD.

Alizarin red S staining clumps of probable apatite among the fibrils of a rice body in patient No 8 (400×).
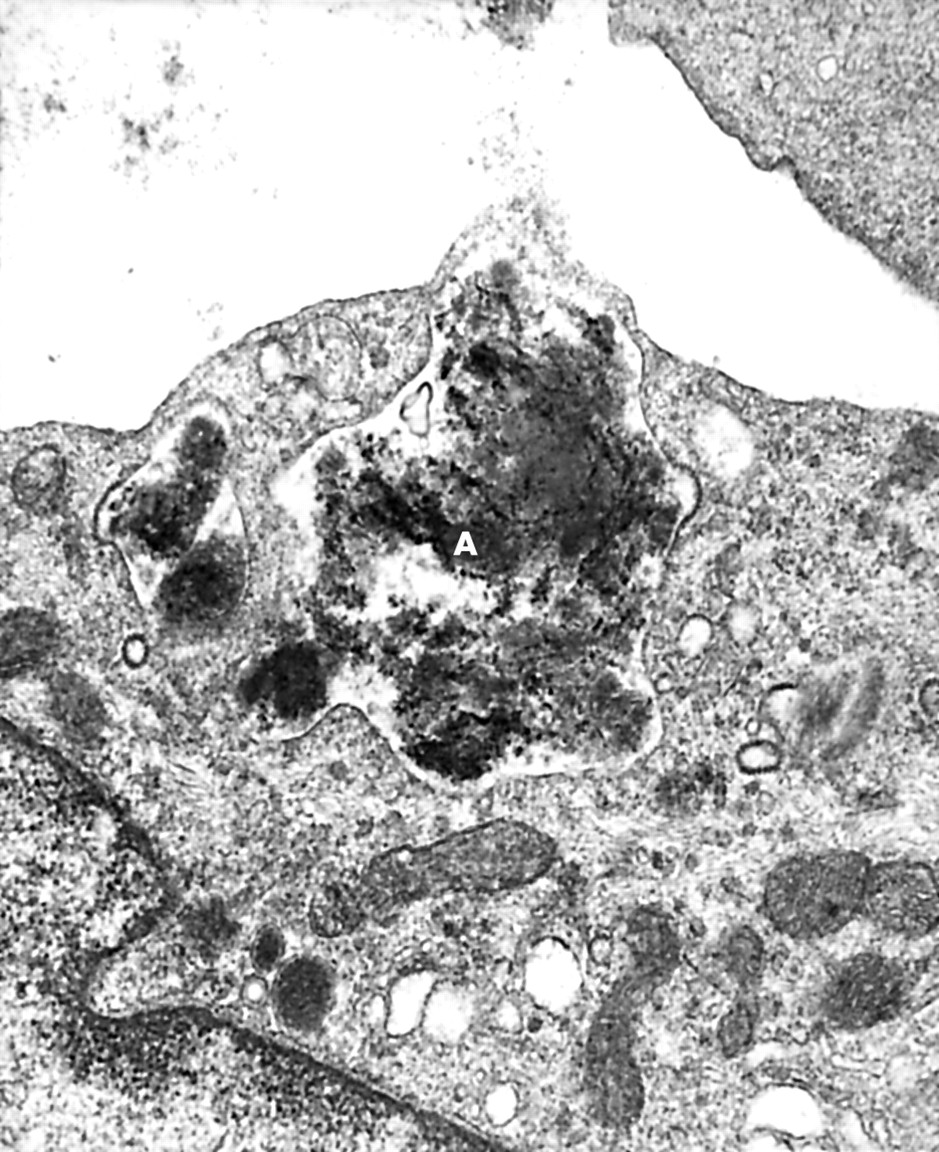
Electron microscopic studies of the rice bodies performed in patients 1–4 all confirmed the presence of typical tiny apatite-like crystals of 100–250 Å length (figs 2A and B). Some of the crystals were in finely granular electron dense material in vacuoles of macrophages; others were enfolded by cell processes as if about to be phagocytosed (figs 2 and 3). The rice bodies were composed of coarse and fine strands of fibrin with typical striations. Some areas exhibited collagen fibres embedded in amorphous material. There were, likewise, occasional viable appearing or degenerated cells scattered within the fibrin (fig 4). Cells were mononuclear, mostly macrophages, and occurred on the surface or within the fibrinous network. Features suggestive of CPPD crystals (fig 3) were seen in two patients by electron microscopy.

Apatite crystals (A) in granular materials being enfolded into a mononuclear cell vacuole within a rice body of patient No 1. Electron micrograph 40 000×.

Electron micrograph of tiny dark apatite crystals in granular materials (A) but not among collagen fibres (C) of patient No 1 rice body. Note a suspected small CPPD crystal apparently forming along a collagen fibre (arrow) (40 000×).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Electron micrograph showing profuse fibrin (F), clumps of collagen (C), and sparse cells (arrows) characteristic of the rice bodies. No apatite is seen in this area. Patient No 4 (6000×).
One patient (No 1) had both electron microscopy and elemental analysis performed on the electron microscopic specimen as noted above. This patient's crystals had calcium:phosphorus (Ca:P) molar ratios of 1.4:1 and 1:1 on electron probe elemental analysis, consistent with some being carbonate substituted apatite and others CPPD. x Ray diffraction studies of the crystals in this patient confirmed the presence of both calcium hydroxyapatite and CPPD crystals.10,11
Patient No 4 merits further description. This 5 year old Hungarian boy was brought to a paediatric rheumatologist for a second opinion because of swelling of his joints and flexion contractures of fingers since infancy. His knees began to swell at age 18 months. There was flexion deformity of the fifth fingers, with some nodules along the flexor tendons of the fingers. A trial of indometacin was apparently given, with no benefit noted. His mother recalled that injections of steroids had been given, although details were not clear.
Pertinent joint examination showed his left thumb to be fixed in a flexed position. The right sternoclavicular joint was slightly swollen, with some degree of synovial thickening of the left shoulder. The synovium at the right elbow was thickened, with limitation in extension. Both wrist joints had moderate swelling with full range of motion. Both knees had considerable swelling, particularly at the left knee, with proliferative synovium and very little fluid. Flexion was limited on both sides, especially the left which was unable to pass 90–100° flexion. Both ankles had synovial hypertrophy with limitation of extension. Blood tests, including complete blood counts, liver, renal, and thyroid function tests, and angiotensin converting enzyme levels, were all normal. Erythrocyte sedimentation rate was only 4 mm/1st h. Antinuclear antibody was negative; immunoglobulin levels and rheumatoid factor were both negative.
Radiographs showed no destructive changes in the knees; there was soft tissue swelling in his ankles. There was a little beaking of the dorsal part of the talus. His wrists showed soft tissue swelling. Both hips had cystic changes in the acetabulum and in the femoral neck.
Synovial fluid aspiration of his left knee disclosed rice bodies on gross inspection, with a non-inflammatory count of 92×106 leucocytes/l. Synovial biopsy showed fibrin over a thin layer of synovial lining cells, with other areas having no lining cells at all. The deeper synovium contained giant cells, some fibrin, and diffuse fibrotic reaction. These findings were felt to be characteristic of the camptodactyly arthritis syndrome.13 He eventually underwent left knee synovectomy. Pertinent family history disclosed an uncle who had flexion contractures of toes from birth and was operated on at age 20. Two older siblings had died from an apparent “inborn error of metabolism”; one died at 8½12 months old and the other at 3 months.
DISCUSSION
Many studies have reported the presence of rice bodies in joint fluid specimens from patients with inflammatory diseases, and especially in RA. Bucki et al first detected rice bodies in joint fluid specimens of four patients with non-inflammatory joint disease and identified apatite deposits in these.10 We likewise found evidence of apatite crystal clumps in rice bodies but, as noted, also found these in a variety of cases in addition to OA.
The origin of rice bodies is almost certainly from the synovium, and their clinical significance has always been obscure. It has most frequently been proposed that microvascular disease within the rheumatoid synovial tissue leads to synovial microinfarcts. Subsequent sloughing of the infarcted tissue into the joint cavity with the surface then covered by fibrin layers may lead to the classical appearance of rice bodies.14,15 Others more generally regarded rice bodies as end products of synovial inflammation, proliferation, and degeneration.8 One fascinating aspect is the persistence of rice bodies in the joint as seen in our patient No 3 on repeated arthrocenteses. In general, there is a paucity of inflammatory cells noted within the rice bodies as also seen in our cases.
Factors involved in development of apatite in these rice bodies need consideration. Repeated local steroid injections appear to be a factor worth investigating as this was reported in six and possibly in a seventh case. Local steroids have previously been reported to cause apatite deposits.16,17 OA is another known cause for apatite presence in SF and was reported by Bucki et al.10 Apatite crystals are also common in SF of patients with OA who have no rice bodies.8–20 Although only one of our patients had OA as the primary diagnosis, five had changes of OA on x ray examination.
Whether apatite and other basic calcium phosphate crystals contribute to joint damage in the arthritides or merely represent an epiphenomenon remains unknown. Apatite crystal clumps or CPPD maybe more common in rice bodies than previously recognised. These occur not only in OA but also in some inflammatory arthritis. Future studies need to consider these crystals as either factors in formation of rice bodies or contributors to the generally more destructive arthritis seen in patients with rice bodies. In conclusion, apatite deposits are a previously underrecognised feature of rice bodies. Might apatite just have been missed in others with RA because it was not considered?