Article Text

Abstract
Objectives: To investigate the effect of prolonged neutralisation of tumour necrosis factor α (TNFα) on the radiological course in rheumatoid arthritis (RA). To assess whether the radiological course can be predicted by clinical variables or biological markers of cartilage and synovium turnover and of endothelial activation.
Patients and methods: Forty seven patients with active RA enrolled at our centre in monotherapy trials with adalimumab (D2E7), a fully human anti-TNFα monoclonal antibody, were studied for two years. Radiographs of hands and feet obtained at baseline and after one and two years were scored in chronological order by a single, blinded observer using the modified Sharp method. Radiological course was classified as stable or progressive using the smallest detectable difference as cut off point. The relation between radiological course and serum markers of cartilage and synovium turnover (metalloproteinases (MMP-1 and MMP-3), cartilage oligomeric matrix protein (COMP), human cartilage glycoprotein-39 (HC gp-39)), endothelial activation (soluble E-selectin and intercellular adhesion molecule (ICAM-1)), and integrated measures of disease activity were assessed using univariate and multivariate analysis.
Results: Radiological evaluation was performed in 36 patients with paired sets of radiographs at baseline and two years. After two years a total of 15/36 (42%) presented no radiological progression. More patients with stable radiological course were still receiving anti-TNFα treatment after two years (13/15 (87%) v 11/21 (52%); p=0.03) and had lower baseline COMP and sICAM-1 levels (p=0.01 and 0.04, respectively) than those in the group with progressive disease. In a logistic regression model the combination of sustained TNF neutralisation and baseline COMP and sICAM-1 levels was predictive for radiological outcome (p=0.03). C reactive protein and disease activity score area under the curve were significantly correlated with changes in radiological scores after two years (r=0.40 and 0.37, p<0.05). Long term TNFα neutralisation decreased the levels of COMP, sICAM, MMPs, and HC gp-39, but not sE-selectin.
Conclusion: The results suggest that long term monotherapy with anti-TNFα has a positive effect on radiological outcome and modulates cartilage and synovium turnover as measured by biological markers. Baseline serum sICAM-1 levels and COMP levels may be helpful to identify patients with progressive or non-progressive radiological outcome.
- rheumatoid arthritis
- tumour necrosis factor blocking agents
- radiological course
- biological markers
- COMP, cartilage oligomeric matrix protein
- CRP, C reactive protein
- DAS, disease activity score
- DMARD, disease modifying antirheumatic drug
- ELISA, enzyme linked immunosorbent assay
- FCS, fetal calf serum
- HC gp-39, human cartilage glycoprotein-39
- ICAM-1, intercellular adhesion molecule-1
- mAb, monoclonal antibody
- MMP, matrix metalloproteinase
- PBS, phosphate buffered saline
- PBST, PBS-Tris
- RA, rheumatoid arthritis
- RF, rheumatoid factor
- SDD, smallest detectable difference
- TNFα, tumour necrosis factor α
Statistics from Altmetric.com
- COMP, cartilage oligomeric matrix protein
- CRP, C reactive protein
- DAS, disease activity score
- DMARD, disease modifying antirheumatic drug
- ELISA, enzyme linked immunosorbent assay
- FCS, fetal calf serum
- HC gp-39, human cartilage glycoprotein-39
- ICAM-1, intercellular adhesion molecule-1
- mAb, monoclonal antibody
- MMP, matrix metalloproteinase
- PBS, phosphate buffered saline
- PBST, PBS-Tris
- RA, rheumatoid arthritis
- RF, rheumatoid factor
- SDD, smallest detectable difference
- TNFα, tumour necrosis factor α
Rheumatoid arthritis (RA) is characterised by a chronic polyarthritis leading to irreversible cartilage damage. In the past decade therapeutic options for the treatment of RA have been broadened by the development of specifically targeted biological agents. Among these, strategies aimed at specific neutralisation of proinflammatory cytokines, such as tumour necrosis factor α (TNFα) and interleukin 1, seem the most promising. Studies with monoclonal antibodies (mAb) against TNFα and with TNF receptor fusion proteins have proved the clinical efficacy of TNFα neutralisation in RA,1, 2 and these treatment modalities have been introduced in clinical practice.
Adalimumab (D2E7) is a fully human IgG1 anti-TNFα mAb developed using phage display techniques.3 Studies in more than 1200 patients have demonstrated the efficacy and safety of prolonged administration of this compound either alone4–7 or in combination with methotrexate.8
Adalimumab and other TNFα blocking agents have a very short lag time to clinical response and induce a rapid decrease in non-specific acute phase reactants such as C reactive protein (CRP) and erythrocyte sedimentation rate.9, 10 Based on the short term effects of TNFα neutralisation on several other biological markers, it has been proposed that this treatment reduces endothelial activation11, 12 and angiogenesis13 and may be chondroprotective.14, 15 Whether these effects are maintained during long term anti-TNFα treatment and whether they correlate with outcome variables has not been elucidated yet.
The first reports with one year's follow up indeed suggest that TNF neutralisation retards radiological progression.16–18 Molecular markers derived from tissue have been suggested as possible prognostic factors for future joint damage.19 If this can be verified, such markers may be attractive tools for treatment decisions and patient selection and also for monitoring of treatment aimed at slowing joint damage progression.
In this study the influence of long term anti-TNFα treatment with adalimumab on the radiological course was assessed. Furthermore, early and long term effects of this treatment on biological markers of cartilage and synovium turnover (cartilage oligomeric matrix protein (COMP), metalloproteinases (MMPs) 1 and 3 and human cartilage glycoprotein-39 (HC gp-39, also known as YKL-40)) and on markers of endothelial activation (sE-selectin and intercellular adhesion molecule-1 (sICAM-1)) were examined. The interrelationships and potential prognostic value of these markers on the radiological outcome after two years were also investigated.
PATIENTS AND METHODS
Patients
All patients with RA included in phase I clinical studies with adalimumab monotherapy at our centre were studied. Patients fulfilled the 1987 American College of Rheumatology criteria,20 had an active disease, defined by a disease activity score (DAS)21 >3.2 at baseline, and underwent a washout period for disease modifying antirheumatic drugs (DMARDs) of at least three weeks before the start of the study. Stable dosages of non-steroidal anti-inflammatory drugs and steroids (dose <10 mg/day prednisone equivalent) were allowed during the study. The two year follow up encompassed a short six to eight weeks placebo controlled, randomised, dose ranging (0.5 – 10 mg/kg) trial followed by an ongoing open label phase. In the latter, all patients, including those initially randomised to receive placebo, received adalimumab, at dosages of 3 mg/kg intravenously biweekly5, 6 or 1 mg/kg subcutaneously weekly.4 In the present analysis, these two dosage schedules were pooled because previous studies have shown a plateau in dose-response at a dose of 1 mg/kg biweekly and because the pharmacokinetics of subcutaneously and intravenously administered adalimumab are similar after an initial period of some weeks.4–7
Anti-TNFα treatment was withheld in cases of adverse events or lack of efficacy. The latter was defined as a DAS decrease of less than 1.2 in the placebo controlled study and according to the judgment of the clinical rheumatologist in the subsequent open phase. When patients were withdrawn they were treated with the best available choice of DMARDs, taking previous treatments into account.
Methods
Radiological and clinical assessments
Standard radiographs of hands and feet were obtained at baseline and after one and two years. Erosions, joint space narrowing, and total scores (erosion plus narrowing) were evaluated in sequential order by a single observer (AdB) who was unaware of the treatment and clinical response measured by the Sharp/van der Heijde method.22 Readings were performed in chronological order because this method has been shown to be more sensitive to change than random readings.23 Moreover, instead of using an arbitrary cut off point, the radiological course of each patient was classified as stable or progressive using the smallest detectable difference (SDD) calculated according to Lassere et al.24, 25 The SDD is the smallest change a measuring instrument can detect, taking the measurement error (in our case the intraobserver variation) into account. The SDD was calculated using a set of 75 radiographs from 25 patients assessed twice by the same observer within an interval of nine months.
The area under the curve for DAS and CRP was calculated using measurements obtained at baseline and every 12 weeks during the two year follow up period. For patients who dropped out before study completion, data were collected during additional post study visits. If these did not extend for a two year follow up, data collected at the last clinical observation were carried forward. Radiographs were obtained at baseline in all patients and repeated after one and two years in all available patients.
Markers of cartilage and synovium turnover and endothelial activation
Serum samples had been collected during the study and stored at –80°C until assay. For all markers, short term changes after the first administration of anti-TNFα mAb or placebo were analysed in samples collected at baseline, day 1, and day 14. Long term changes were assessed using samples collected after a two year follow up for all markers with exception of the MMPs. The latter were assessed at month 6 for technical reasons. All samples from the same patient were analysed simultaneously to minimise interassay variations.
Systemic levels of COMP were measured using a previously described enzyme linked immunosorbent assay (ELISA) with an intra-assay variation of <5%.26, 27 The concentrations of collagenase (MMP-1) and stromelysin-1 (MMP-3) were measured by ELISA according to the manufacturer's instructions (Binding Site, Birmingham; intra-assay variation <13%).28 The adhesion molecules sE-selectin and sICAM-1 were measured by ELISA as previously described.29, 30 Intra-assay variation for both essays is <10%.
HC gp-39 levels were assessed as follows. Polystyrene 96 well microplates (Nunc Maxisorb C12) were coated overnight at 4°C with 150 μl/well of 1.0 μg/ml mouse anti-HC gp-39 capture antibodies (HC gp-39 8B) in coat buffer. The supernatant was discarded and the wells were incubated for one hour at room temperature with 200 μl phosphate buffered saline (PBS) and 1.0 % bovine serum albumin to block excess free binding sites. Subsequently, plates were washed three times with 500 μl PBST and incubated for one hour at room temperature with 100 μl sample, 100 μl recombinant HC gp-39 standard in assay buffer (PBS, 10% fetal calf serum (FCS)), 100 μl reference in assay buffer (10 times the highest SD), and 100 μl recombinant HC gp-39 control samples (at 5.0, 25.0, and 75.0 ng/ml) in assay buffer. Plasma samples were diluted 1:10 in assay buffer (10% FCS, 0.1% Triton-X, 0.2% Kathon CG in PBS) After this incubation the plates were washed three times with 500 μl PBST and incubated for one hour at room temperature with horseradish peroxidase labelled with mouse anti-HC gp-39 detection antibodies (HC gp-39 10B) at a dilution of 1:10 000 in assay buffer. Then, the plates were washed three times with 500 μl PBST and incubated for five minutes with 100 μl tetramethylbenzidine/ureum peroxide substrate solution (Organon Teknika). The enzyme reaction was stopped by addition of 50 μl 4 M sulphuric acid to each well. The A450-A690 absorbencies were measured with a microplate reader. Calibration curves (0.15–24 ng/ml) for recombinant HC gp-39 were constructed using four parameter logistic regression, and HC gp-39 concentrations in study samples and quality control samples were calculated with the data reduction package PhIRSt (Phoenix International Reporting System, version 2.1). The lowest limit of measurement was 0.15 ng/ml. The assay has been validated and the accuracy of the quality control samples was higher than 94.7% and the coefficient of variation was lower than 9.7%.
Statistical analysis
Within-group comparisons were made using paired Student's t test and Wilcoxon's signed rank test. For comparisons between groups Mann-Whitney U tests and χ2 tests were used as appropriate. Correlations were tested with Pearson or Spearman correlation tests. The use of a parametric or non-parametric test was dependent on the data distribution. The p values are reported without adjustments for multiple comparisons.
Multiple logistic regression analysis was performed to elucidate whether markers of cartilage and synovium turnover and endothelial activation had prognostic value using the radiological progression from baseline to two years and from one to two years as dependent variable. Additional independent variables considered were treatment status at study completion (0, receiving treatment; 1, withdrawal), IgM rheumatoid factor (RF) (0, negative; 1, positive), and the DAS and Sharp scores at baseline. Potential interactions between independent variables were tested before inclusion in the model. Analysis was performed using the Astute Base Module version 1.50 package and SAS version 6.12.
RESULTS
Clinical course
A total of 47 patients were studied whose characteristics are shown in table 1. At inclusion, patients had active disease, long disease duration, and had been refractory to a large number of DMARDs before anti-TNFα treatment. No significant differences between patients randomly allocated to receive adalimumab or placebo were seen in the blinded study. Figure 1 depicts the course of the follow up. As shown, a total of 41 (87%), 33 (70%), and 26 (55%) patients were still receiving treatment and maintained responder status after six months, one and two years' follow up, respectively. Two patients died during the follow up period; one of them had experienced an acute myocardial infarction in the placebo controlled phase.
Patient characteristics at baseline; patients with and without radiological progression. Data expressed as mean (SD) unless otherwise stated

Scheme of patients receiving treatment, primary reasons for drop out, and treatments used thereafter (box) during the two year follow up. *Patients who did not respond after three administrations of adalimumab were withdrawn according to the study protocol.
Clinical improvement occurred rapidly after the start of treatment. At two weeks from baseline 16/35 (46%) patients treated with adalimumab but none in the placebo group had achieved responses according to the EULAR definitions. Figure 2 shows the course of the DAS and CRP during the follow up.

Course of the median DAS and CRP during the two year follow up. Intention to treat analysis.
Radiological course
As expected from the long disease course, most patients had high radiological scores at baseline (table 1). Paired radiographs were available at baseline, one, and two years in 36 patients. The median changes in radiological scores after one and two years were 5 and 9 for erosions and 3 and 5 for narrowing, respectively.
For this study, the SDDs in total Sharp/van der Heijde scores were 8 and 13 after one and two years, respectively. When these cut off points were used, 19/36 (53%) and 15/36 (42%) patients presented no signs of radiological progression after one and two years' follow up, respectively. Comparison between the groups with stable radiological course and those with radiological progression showed that the former group encompassed more patients still receiving treatment at study completion than the latter (13/15 (87%) v 11/21 (52%), respectively; p=0.03). The Sharp scores at baseline tended to be lower and the percentage of women higher among patients with stable radiological course, but this did not reach statistical significance (table 1).
Characteristics of patients who still received anti-TNFα treatment at study completion were similar to those who had switched to other treatments (data not shown), with the exception of the radiological course, which was stable in 13/24 (54%) of the former but in only 2/12 (17%) of the latter (p=0.03).
Relationship between radiological course, disease activity, and biological markers
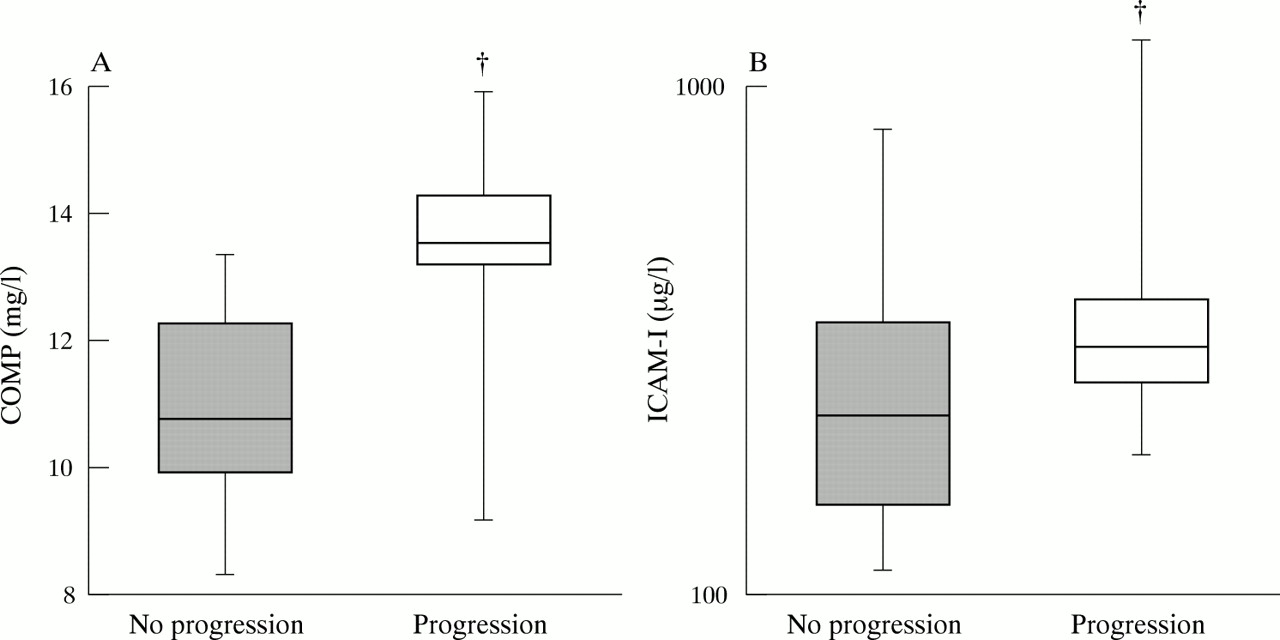
The serum levels of the biological markers at baseline were compared between patients with stable and progressive radiological course. These groups only differed in baseline COMP and sICAM-1 levels, which were higher in the progressive group (p=0.01 and p=0.04, respectively). After two years, COMP and sICAM-1 had decreased in patients with radiographic progression (p=0.0003 and p=0.03 compared with baseline for COMP and sICAM-1, respectively) and remained low and unchanged in patients with stable radiological course.
Table 2 outlines the correlations between baseline radiological and clinical variables and biological markers. As shown, the classical acute phase reactant CRP correlated with both MMPs, HC gp-39 and, to a lesser extent, also with sICAM-1 but, importantly, not with COMP levels. COMP and HC gp-39 correlated significantly with age and this was not because of a confounding effect of disease duration (data not shown).
Correlations between radiological score, acute phase, and markers at baseline
We performed a univariate analysis to assess which variables might be prognostic for changes in radiological scores over time. The changes in total Sharp/van der Heijde scores between baseline and two years showed modest correlations with the area under the curve for CRP and DAS (r=0.40 and 0.37, respectively; p<0.05) and with baseline COMP and sICAM-1 levels (r=0.30 and 0.37; p=0.06 and 0.04, respectively). None of the biological markers or clinical parameters at baseline showed a significant correlation with the radiological changes between one and two years' follow up (data not shown). Similar results were found when the analysis was performed separately for the subgroups who were receiving treatment and dropped out (data not shown).
Multiple logistic regression analysis
Two models, using the radiological changes between 0 and two years and between one and two years respectively as dependent variable, were initially considered. The latter was abandoned after the negative results of the univariate analysis. The final logistic regression model using presence/absence of radiological progression from 0 to two years as dependent variable included the following independent variables: treatment status (receiving treatment or drop out; 0 or 1), baseline sICAM-1, and baseline COMP. RF was not included as an explanatory variable, because all but one patient were RF positive. The DAS and CRP at baseline were also left out of the model because they did not differ between patients with stable and progressive course (table 1). Although baseline Sharp scores were not associated with progression using univariate tests (r=0.28, p=0.09), this variable was tested in the model, because differences—although not significant—were found at baseline between patients with and without progression (table 1).
Table 3 shows the logistic regression model. Patients continuing to receive anti-TNFα treatment had a fourfold higher chance of having a stable radiological course. Higher COMP and to a lesser extent sICAM-1 at baseline were associated with worse radiological outcome independently from the effect of the treatment. As shown, none of these three individual variables reached significance, but the complete model had a significant explanatory effect on the radiological progression as indicated by the p value for the χ2 for covariates (0.03). Inclusion of baseline Sharp values in the model scores did not change these results (data not shown).
Multiple logistic regression results of predictors for radiological progression
Markers of endothelial activation and cartilage turnover
Figure 3 outlines the short and long term changes in the marker levels during anti-TNFα treatment. Short term measurements within two weeks after the first dose, allowed comparison between anti-TNFα and administration of placebo. As observed, none of the markers showed significant changes after placebo. In contrast, the levels of MMP-1, HC gp-39, and the adhesion molecules sE-selectin and sICAM-1 decreased significantly (p<0.05) and MMP-3 also tended to drop (NS) within two weeks after starting anti-TNFα treatment. This was not the case for COMP levels, which remained stable during the first two weeks.

Short and long term changes in markers of synovium turnover (metalloproteinases MMP-1 (A), MMP-3 (B), endothelial activation (sE-selectin (C), sICAM-1 (D)) and cartilage and COMP (E), and HC gp-39 (F)). Short time changes: changes seen within two weeks (D=0 to D=14) after the first dose of anti-TNFα (continuous line) or placebo (dashed line) in the double blind phase. Long term changes: changes occurring between baseline and the two years follow up. The boxes illustrate the mean (horizontal bar), 25th and 75th centiles (box) and 5th and 95th centiles (bars). Significance is shown as p<0.05, tested within groups (*) and between groups (†).
Long term measurements allowed comparison between patients still receiving anti-TNFα treatment and those who dropped out and were treated with DMARDs. HC gp-39 and COMP levels were significantly decreased after two years (p<0.0001 and <0.001, respectively) irrespective of the treatment that patients received at this time point (figs 3E and F). The levels of sICAM-1 values showed a modest decrease only in patients who were still receiving anti-TNFα treatment (p<0.05) but not in those patients who had switched to other treatments (fig 3D). In contrast, the final concentrations of sE-selectin did not differ from baseline values (fig 3C). Further reductions in MMP-1 and MMP-3 concentrations (p<0.05) were found after six months of treatment in the whole patient group (figs 3A and B). At that time the number of patients who had switched to other treatments was too small to allow for comparisons with those still receiving anti-TNFα.
DISCUSSION
Radiological assessment remains the cornerstone of outcome assessment in RA, but has important drawbacks such as the extensive lag time to change after therapeutic interventions. This has resulted in an intensified search for predictors of outcome in RA in recent years. The need for better monitoring of clinical decisions and aspects of cost effectiveness is especially high for new and expensive biological agents such as those directed against TNFα. Potential predictors for outcome could be used a priori for adequate patient selection or for adjustment of treatment.
This is, to our knowledge, the first long term follow up study on both the effect of anti-TNFα monotherapy on radiological course and on the prognostic value of biological markers of cartilage and synovium turnover and endothelial activation. For the radiological assessments, our findings support the notion that sustained TNFα neutralisation can positively modulate the outcome in advanced RA. Firstly, roughly 55% of the patients still receiving anti-TNFα treatment after two years showed a stable radiological course compared with only 17% of the patients who had to stop anti-TNFα during the same observation period. It should be pointed out that a selection bias cannot be excluded in this comparison and that patients who dropped out had a more refractory or severe RA. Nevertheless, switching was mostly due to reasons other than lack of response (fig 1). Moreover, patients who dropped out from anti-TNF were treated thereafter with the best available choice of antirheumatic drugs and this might also have affected the radiological course positively. Secondly, our results also show that blocking TNFα resulted in a rapid and sustained reduction of CRP and DAS and that radiological progression is associated with time integrated measures of these variables. Such a relationship has been previously described in patients with RA receiving conventional DMARD treatment31 but not in patients with longstanding disease treated with anti-TNFα.
Recently published reports on random x ray readings after one year's treatment with this18 and other anti-TNFα strategies in patients with advanced disease17 and early RA16 have suggested that blocking TNFα can arrest radiological progression in RA. Our findings show that this may also be the case in most patients continuing to receive treatment for prolonged periods. It should be emphasised that the follow up in our study was longer than in previous reports and that radiographs were scored chronologically as originally described and recently recommended.32 In contrast with random readings, this method assumes that radiological damage is irreversible and thus detects more progression but is also more sensitive to change.23 Moreover, we addressed recent OMERACT recommendations33, 34 by taking intraobserver reproducibility into account.
For the effect of anti-TNFα treatment on biological markers, we observed a rapid and sustained down modulation of non-specific acute phase reactants such as CRP. With the notable exception of COMP, all markers studied correlated positively with CRP levels and most of them fell within two weeks of treatment initiation. This is in line with previous data on the kinetics35, 36 and on the effect of anti-TNFα on these markers in patients with RA.11, 14, 15 COMP levels, in contrast, did not change over the short term and our results confirmed the acute phase independent nature of this marker.37, 38
Our study was directed to identify potential predictors of radiological outcome. Analysis of the relationship between biological markers and radiological course yielded some interesting findings. Among the biological markers studied, univariate analysis showed that only baseline COMP and sICAM-1 had moderate correlations with radiological course over the two years' follow up. This was corroborated by the fact that patients with radiographic progression had significantly higher levels of COMP and sICAM-1 than those with stable radiological course (p=0.01 and 0.04, respectively). These findings are of interest because previous studies have found that high COMP levels were prognostic for large joint destruction in RA.37 Our data suggest that, in contrast with data published concerning early RA,38 COMP levels may also predict small joint damage in RA. sICAM-1 is known to be up regulated in synovial tissue and its soluble form is found in high concentrations in patients with RA.39 Down regulation of the expression of this and other adhesion molecules has also been implicated in the mechanism of action of anti-TNFα11, 12 and other antirheumatic drugs.40, 41 In addition, antibodies that block sICAM-1 have been tested with favourable results in patients with RA.42 The relation of baseline sICAM-1 levels with radiological course has, however, not been previously described, although in a cross sectional study higher sICAM-1 levels have been found in patients with radiological damage than in those without.43
Circulating MMPs were associated with acute phase parameters but not found to be prognostic for radiological course from baseline up to two years or between one and two years' follow up in our study. Such a prognostic value has been previously suggested in patients with early RA.44, 45 The long disease duration of our study group is probably the reason for this difference, as another study including patients with longstanding RA also yielded a negative result.46 Whether differences in treatments used in our study and other studies mentioned above also contribute to this apparent contrast is not clear.
Besides the higher baseline levels of COMP and s-ICAM-1 (fig 4) and the higher drop out rate seen among patients with progressive radiological course, this group tended to have higher baseline x ray scores than those showing no progression (table 1). This difference was, however, not significant and neither disease activity nor radiological damage at baseline were prognostic for radiological course. Inclusion of the latter in the regression model did not change the results of the analysis.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Concentrations of COMP (A) and sICAM-1 (B) in patients with and without radiological progression. The boxes illustrate the mean (horizontal bar), 25th and 75th centiles (box) and 5th and 95th centiles (bars). Significance is shown as p<0.05, tested between groups (†).
Logistic regression using baseline COMP, sICAM-1, and treatment status at completion showed that these independent variables together had significant prognostic value for the radiological outcome after two years, although each individual variable failed to reach significance in this statistical model. This may be because of the size of the sample, and confirmation of these data is therefore needed in a larger cohort. The model, also suggests that both the treatment with anti-TNFα and baseline COMP levels are independently associated with radiological outcome.
Although this was not the main goal of our study, the levels of biological markers at study completion were compared with those at baseline. Interestingly, decreases in COMP levels were seen at study completion, irrespective of the treatment (fig 3E), whereas sICAM-1 levels were lower than baseline only in patients still receiving anti-TNFα treatment (fig 3D). This association with treatment at study end might explain the disappearance of the prognostic value of sICAM-1 in the multivariate analyses. In patients with a stable radiological course COMP and sICAM-1 levels remained low and unchanged. Of note, both MMPs and HC gp-39 levels but not E-selectin showed further decreases in the long term. Earlier studies showed that sICAM-1, but not sE-selectin levels were raised in patients with RA.39 This shows that the endothelial markers sICAM-1 and sE-selectin are differentially regulated and do not possess the same properties as disease markers.
In conclusion, our study indicates that sustained anti-TNFα monotherapy with adalimumab has a positive effect on radiological outcome. This intervention has rapid effects on biological markers of cartilage and synovial turnover and endothelial activation, which are associated with the acute phase reaction, but not on COMP levels. This strengthens the importance of serum COMP as a selective cartilage marker. Besides sustained anti-TNFα treatment, only baseline COMP and to a lesser extent sICAM-1 levels were prognostic of the radiological course. These markers might potentially be used to identify patients at risk for development of radiological damage.
Acknowledgments
We are indebted to B Hendriks and MC Ruijs (Organon, the Netherlands) and to M Lindell (Lund University, Sweden) for their technical assistance.
REFERENCES
Footnotes
-
Professor LFC Breedveld was acting editor for this paper.