Article Text

Abstract
Objectives: To investigate two questions in a community based population of people with chronic shoulder pain. Firstly, does chronic pain lead to impaired psychological health over time? Secondly, how does restriction of daily activity influence pain perception and psychological health?
Methods: Two postal surveys, two years apart, were carried out to identify a group of subjects with chronic shoulder pain. The first survey was sent to a random sample of adults (n=40026) registered with a primary care practice, and included a pain manikin, demographic information, and the Hospital Anxiety and Depression scale (HAD). The second survey was sent to those subjects who reported unilateral shoulder region pain in the first survey and it included a shoulder-specific disability scale, pain severity score, and the HAD.
Results: 2606 (65.1%) people responded to the initial survey. Of these, 304 (11.7%) reported unilateral shoulder region pain at baseline. In the subsequent survey, there were 234 responders (83.3% adjusted response): 142 of these reported shoulder pain and formed our study group of “subjects with chronic shoulder pain”. Within this group there was no significant change in psychological distress scores between baseline and follow up. Both the disability score and psychological distress scores correlated significantly with pain severity (disability v pain r=0.536, p<0.001; psychological distress v pain r=0.269, p=0.002). When the correlation between disability and pain severity was corrected for possible confounders, it remained significant (r=0.490, p<0.001). This was not the case for the correlation between psychological distress and pain (p>0.05). Disability was significantly correlated with psychological distress on univariate (r=0.445, p<0.001) and multivariate analysis (r=0.341, p=0.002).
Conclusion: In those with chronic shoulder pain the relation between pain and psychological health seems to be linked to disability. Psychological distress was not explained by persistent pain itself.
- shoulder pain
- shoulder disability
- anxiety
- depression
Statistics from Altmetric.com
Most clinicians recognise that psychological health is important in the presentation and prognosis of a painful condition. However, there is only a limited understanding of the mechanisms behind this relationship. It might be suggested that pain is deleterious to psychological health, not only at one particular time but also over the course of time. Alternatively, both pain perception and psychological health may be influenced by other factors such as restricted physical activity and its effect on daily living.
One musculoskeletal condition considered to have a psychological component is the common symptom complex of pain in the neck and shoulder region.1 Rheumatology texts traditionally report this to be a benign and self limiting problem, but several studies have now shown it to be a persistent and often disabling condition,2–5 although underreported.6 Little is known about its long term prognosis, particularly among subjects who do not seek medical help. Most published work comes from primary care or hospital, but in one community based study 50% of subjects had pain at follow up, three years later.3
Our study investigates the interrelationship between shoulder pain, disability, and psychological distress in adults with chronic shoulder pain, and specifically considers two questions: (a) Does chronic pain lead to impaired psychological health over time? (b) How does restriction of daily activity influence pain perception and psychological health?
METHODS
Design
We carried out two postal surveys, two years apart, to identify a group of subjects with chronic shoulder pain; defined according to self reported shoulder pain on both occasions. This group formed our study population.
Baseline survey
As part of a general health survey, 4002 subjects were randomly selected, using Epi-Info version 6.0,7 from a population base of all adults aged between 18 and 75 years registered at a mixed urban/rural primary care practice (total practice size 10 000; 8004 adults aged 18–75 years).
A baseline questionnaire was sent to these subjects, which included a manikin for identifying pain experience in the previous month. The use of this manikin has been described in an earlier population survey.8 Shading within either the left or right areas of the manikin, as indicated in fig 1, was used to define subjects with unilateral shoulder region pain. This method of defining shoulder region pain in postal surveys has been previously validated.8 The baseline questionnaire also included demographic data and the Hospital Anxiety and Depression scale (HAD).9 The latter has been validated for use in the general population.10,11
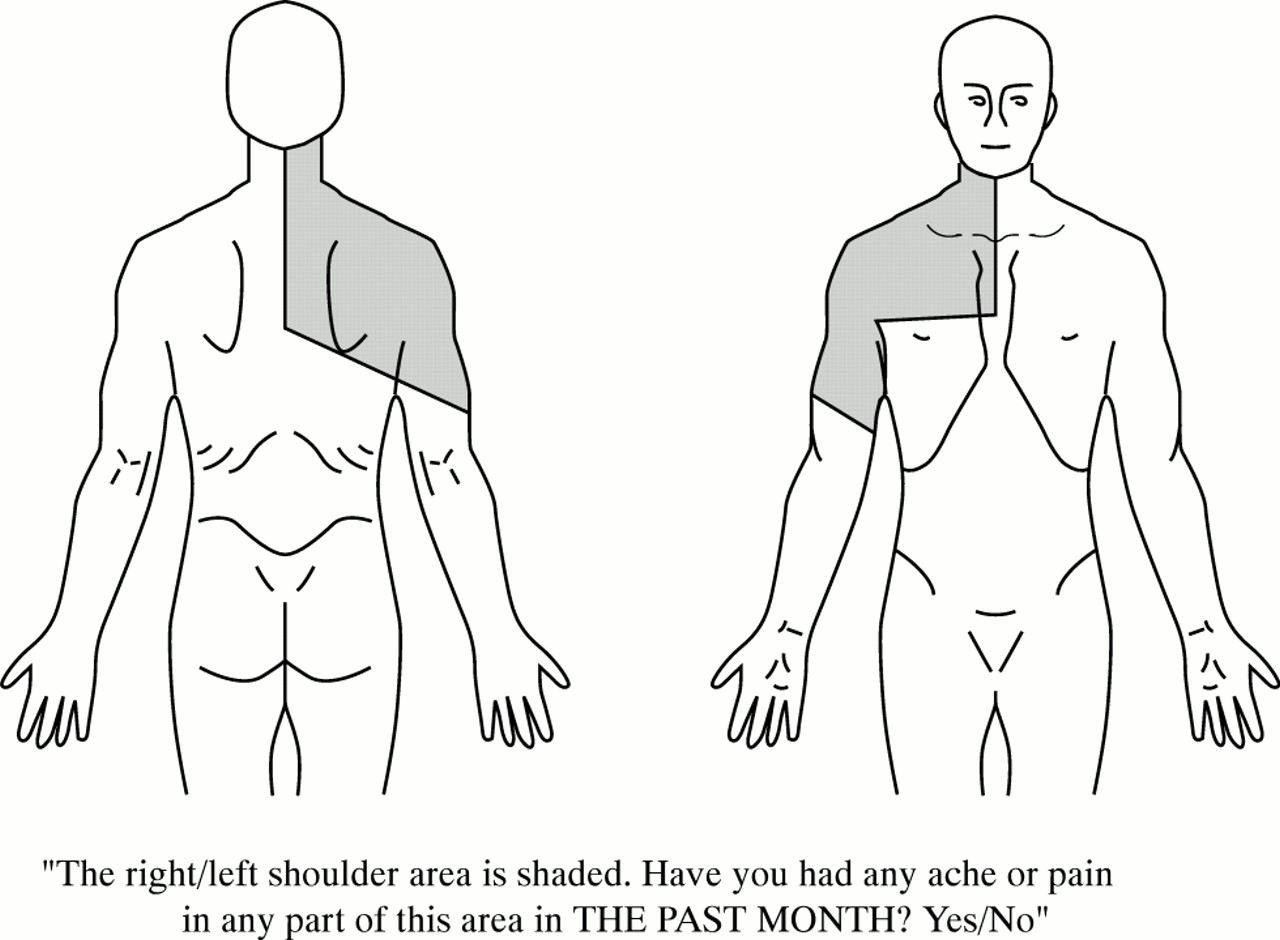
Survey definition of shoulder region pain.
Follow up survey
A follow up questionnaire was sent 24 months after the baseline survey to all subjects who had reported unilateral shoulder region pain at baseline and who were still registered at the practice at the time of follow up. Subjects were defined as having chronic shoulder pain if they answered “yes” to a question asking whether they had had an ache or pain in the previous month in any part of a preshaded manikin (fig 1). Both the right and left sides of the shoulder region were considered.
The follow up questionnaire also determined the subject's global assessment of pain outcome using a five point Likert scale (a lot better, better, same, worse, a lot worse); perceived duration of the current pain episode; pain severity over the previous month measured on a 10 point Likert scale; shoulder-specific disability using a modified 23 item version of a validated scale, on which a score of five or more indicates a significant disability12; HAD scale; and demographic details. A subject's social class was defined according to whether their most recent occupation was manual or non-manual using the classification of the Office of National Statistics.13
Analysis
The HAD scale9 was originally designed to define cases of anxiety or depression according to the total score for a subgroup of questions (<8=non-case; 8–10=probable case; >10=definite case). The use of the actual score as a numerical measure has been validated for anxiety, depression, and a combination of the two (“psychological distress”).10,11 However, these cut off points should not be regarded as the same as a general practitioner's clinical diagnosis of anxiety or depression in an individual patient.
Previous users of the shoulder disability questionnaire had calculated a disability score from the absolute sum of positive responses.12 In our study we included a correction for the total number of completed questions. Recalculation showed that our conclusions from the data would not have changed if the absolute sum had been used.
The analysis involved those who had pain on both occasions—that is, those with chronic shoulder pain. Our first study question was addressed by an analysis of whether there had been any change in HAD scores over the two years of follow up within our study group of patients with chronic shoulder pain. The second study question was addressed by focusing on the association between the HAD score, disability score, and pain severity at the time of the second survey. We used Pearson's correlation to evaluate the individual bivariate relationships between HAD, disability, and pain scores. Multifactorial analyses using partial correlation were carried out to assess bivariate associations after adjustment for potential confounding.
To assess the external validity of the study with respect to non-response, baseline demographic data and HAD scores of responders and non-responders to both baseline and follow up questionnaires were compared to identify any information bias. The χ2 test was used for the analysis of categorical data and the t test for analysing quantitative data.
All statistical tests were two tailed with α=0.05, and were carried out using SPSS version 10.0.14
RESULTS
The study group: response rates and external validity
There were 2606 (65.1%) responders to the initial questionnaire. Responders were representative of both the total sample and the adult practice population as a whole,15 although slightly more women than men responded (percentage females: adult practice population 50.4%; responders 53.8%) and responders tended to be older (mean age: adult practice population 44.6 years; responders 47.7 years). Of these total responders, 304 (11.7%: 95% CI 10.4% to 12.9%) subjects reported unilateral shoulder pain.
At 24 months, 281 of the 304 adults with unilateral shoulder pain at baseline were still registered at the practice and were sent the second survey. There were 234 responders to this follow up survey, representing 77.0% of the original cohort of 304, and 83.3% of the 281 subjects who were sent the follow up questionnaire. Responders to the follow up questionnaire were significantly older (mean age 53.6) than non-responders (mean age 43.7; t=4.2, p≤0.001), but there was no significant difference in sex ratio (females: responders 51%; non-responders 45%; χ2=0.60, p=0.440) or baseline psychological distress score (mean psychological distress score: responders 11.01; non-responders 11.85; t=0.79, p=0.430).
A total of 222 subjects completed the shoulder pain question, which inquired about shoulder region pain in the previous month (fig 1). A total of 142 of these (64.0%: 95% CI 57.6% to 70.3%) indicated that they had had shoulder region pain in the month before the survey and were thus defined as the study group with chronic shoulder pain.
Change in psychological distress over time in the chronic pain group (study question 1)
Within the group with chronic pain there was no significant change in scores for anxiety, depression, or psychological distress between baseline and follow up (table 1).
Change in HAD anxiety/depression scores over two years in patients with chronic shoulder pain
Cross sectional analysis of the chronic pain group at follow up (study question 2)
Table 2 summarises the chronic pain group's global assessment of pain, perceived duration of current pain episode, pain severity, disability, and prevalence of anxiety and depression in the follow up survey. Sleep was the most common difficulty identified by the disability instrument, with 90 (74%) subjects saying they had to change position frequently at night and 79 (69%) saying they slept less well because of their shoulder problem. Other common difficulties were in carrying objects such as shopping (n=62, 54%); doing heavy jobs (n=55, 47%), and reaching for objects (n=52, 46%).
Descriptive data for the group with chronic pain
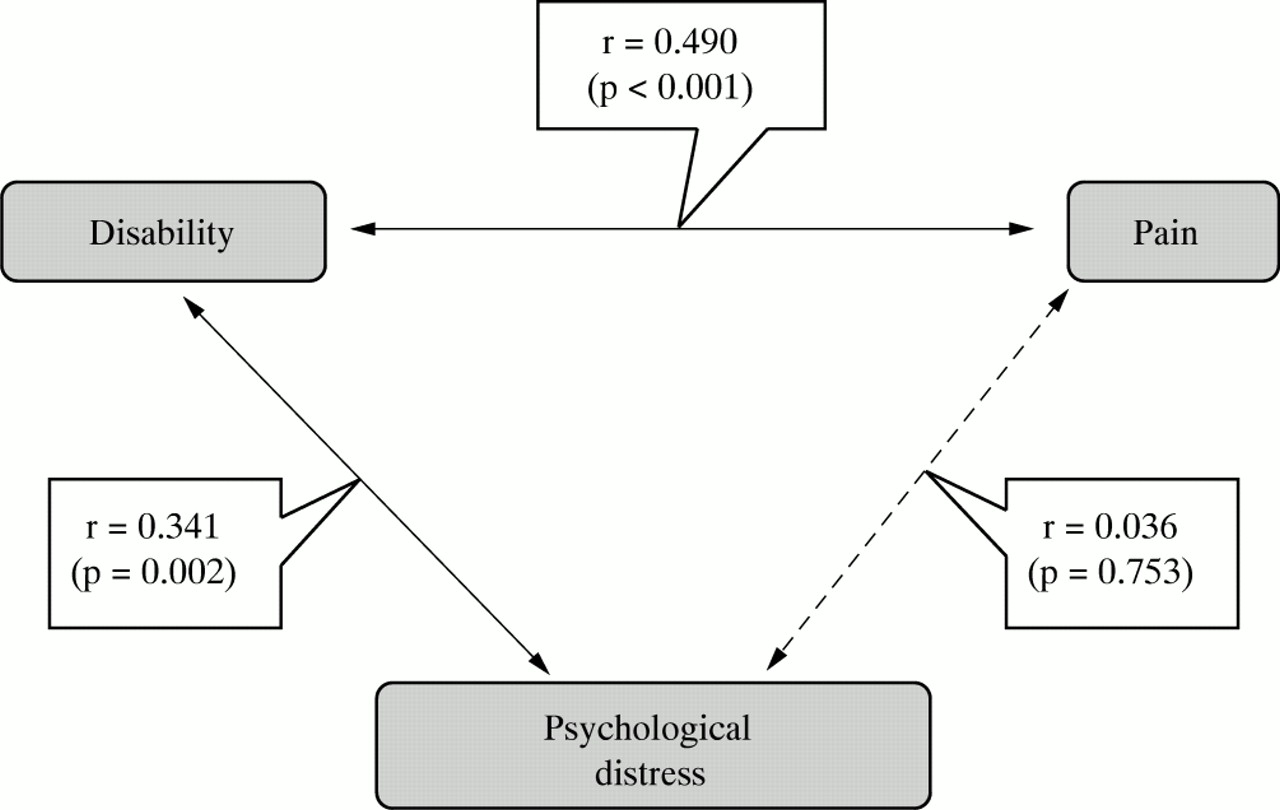
In the group with chronic pain at follow up, both the disability score and the HAD scores (for anxiety, depression, and psychological distress) correlated with pain severity as measured by the Likert 10 point scale (disability v pain r=0.536, p<0.001; anxiety v pain r=0.263, p=0.002; depression v pain r=0.202, p=0.021; psychological distress v pain r=0.269, p=0.002). When the correlation between disability and pain severity was corrected for possible confounders (age, sex, social class, employment status, HAD scores at follow up) it was still significant (r=0.490, p<0.001). In contrast, when the relationships between the HAD scores and pain severity were similarly corrected for confounders (this time including the disability rather than the HAD scores) there was no longer a significant correlation (anxiety v pain r=0.083, p=0.462; depression v pain r=−0.038, p=0.740; psychological distress v pain r=0.036, p=0.753). Disability was significantly correlated with anxiety, depression, and psychological distress and this remained the case after adjustment for pain severity and demographic factors (disability v anxiety r=0.265, p=0.017; disability v depression r=0.372, p=0.001; disability v psychological distress r=0.341, p=0.002)(fig 2).

{kind=link}
{kind=link}
Results of the multivariate analysis of the relationship between pain, disability, and psychological distress.
DISCUSSION
In this study we used a pragmatic description of the well recognised symptom complex of shoulder region pain, but limited ourselves to unilateral symptoms at baseline. Persistent shoulder pain two years later then defined our group with chronic shoulder pain. Community based prevalence estimates for shoulder pain have been reported to be between 7% and 34%,6,16,17 and our prevalence estimate of 11.7% lies within this range. A previous community based study by Macfarlane and colleagues has shown that 50% of subjects with shoulder pain had persistent problems three years later.3 Macfarlane et al used a shaded manikin (among other methods) to determine the presence of shoulder pain at baseline, with bilateral pain included. In our study 64% of subjects stated they had pain after two years, with half of these developing bilateral pain, and 10% unilateral pain on the opposite side.
Our study focused on a group with chronic symptoms and on measurements made after two years of follow up. In this group, pain was associated with significant disability in 50% of subjects. This is higher than that found in the community validation study for this disability instrument,12 in which 34% scored five or more. This is likely to reflect the fact that all our subjects had longstanding pain. Our figure is similar to previous work demonstrating that 40% of workers with daily shoulder/neck pain are seriously hampered or unable to perform ordinary work.6 The outcome study by Macfarlane et al described a similar pattern of disability.3
One might expect that in a group of subjects with chronic pain, the level of depression would increase with time. We could find no evidence to suggest that the persistence of pain itself was associated with worsening depression or anxiety despite the inclusion of subjects who had developed more widespread pain (that is, unilateral to bilateral) over the two years of follow up. In studies of back and other musculoskeletal pain in primary care Von Korff similarly showed that the chronicity of pain itself does not alter the degree of depression.18,19 However, the absence of change may be because any psychological deterioration had “levelled off” before the start of our study.
In this study anxiety and depression were significantly correlated with pain severity, but this relationship was dependent on the level of disability. This is in agreement with work on non-specific musculoskeletal pain showing that it is the extent to which pain interferes with normal activities that predicts depression rather than the pain itself.18 There are a number of possible explanations. Firstly, in our study a problem with sleeping was the dominant disability. This is important because it is likely to reflect nocturnal pain or discomfort, which a patient completed pain severity scale may not reflect. Alternatively, it may be because it is disability rather than pain itself that requires a redefining of self identity, resulting in psychological distress.20 There is a tendency for patients and clinicians alike to focus on pain rather than disability. Pain management programmes incorporate the idea that by concentrating on disability, or more particularly the resulting handicap, rather than focusing on the level of pain itself, there is psychological benefit to the patient. Clinicians, likewise, should be determining ways in which disability may be reduced.
In conclusion, we have confirmed the findings of others that shoulder pain can be a persistent and often disabling condition. We have shown that at a single time point, the relation between pain and psychological health is dependent on disability and that psychological health is not affected by the persistence of pain itself. Thus measuring pain alone is an inadequate means by which to determine the severity of shoulder, and possibly other, musculoskeletal ailments; a measure of associated disability is also required. This has been acknowledged in disability research, but the implication for clinical practice is that it underlines the importance of the clinician determining the extent of functional restriction rather than the degree of pain alone.
Acknowledgments
The following provided invaluable support: Rhian Hughes, Tracy Whitehurst, Juliet Firth, Joanne Bailey, and the doctors and staff of the Wolstanton Medical Practice. We also thank Dr Umesh Kadam for his help with the administration of the baseline survey, and Jonathan Hill for his comments on the manuscript.