Article Text

Abstract
OBJECTIVE To evaluate the efficacy and safety of a long acting somatostatin analogue in a subset of patients with refractory rheumatoid arthritis (RA).
METHODS Ten patients with active, refractory RA, who had failed to respond to at least four disease modifying antirheumatic drugs (DMARDs), were treated with monthly intramuscular injections of 20 mg of a long acting preparation of octreotide (Sandostatin-LAR) for three months. They were evaluated every two weeks in an open label pilot study. The primary measure of clinical response was the American College of Rheumatology criteria for a 20% improvement in measures of disease activity (ACR 20).
RESULTS Eight patients completed the 14 week trial, while two patients received only one or two doses of the somatostatin analogue, but were eligible for evaluation. On an intention to treat basis 6/10 patients responded: four patients met the ACR 20 criteria at weeks 6–10, while two patients continued to improve with time, and met the ACR 50 and 70 criteria respectively, at week 14. On evaluation of the 10 patients as a group, a significant improvement (p<0.05) was noted in the mean visual analogue scales of pain, doctor's and patient's global assessment of disease activity, and in the mean number of swollen joints. Adverse effects were minor: transient bloating and loose stools, an urticarial rash (n=1), and a transient increase of liver enzymes (n=1).
CONCLUSION Treatment with a long acting somatostatin analogue led to significant clinical improvement in a subset of patients with active, refractory RA. The treatment was relatively safe and well tolerated. Further large, placebo controlled studies are required to evaluate this drug as a potential DMARD for patients with RA.
- somatostatin
- rheumatoid arthritis
- immunomodulation
- angiogenensis
Statistics from Altmetric.com
Rheumatoid arthritis (RA) is a chronic, multisystem autoimmune disease characterised by persistent synovitis. The chronic inflammation leads to development of a pannus—an aggressive inflammatory tissue where activated T lymphocytes, macrophages, B cells and the cytokines they produce, as well as active angiogenesis play a major part in the progressive destruction of the joints.1
In addition, neuroendocrine-immune interactions have been shown to contribute to the pathogenesis of autoimmunity.2Somatostatin (SOM) is a widely distributed neuropeptide, first discovered in 1973 as a growth hormone release-inhibiting factor in the hypothalamus.3 Shown to have numerous immunomodulatory effects in vitro, in animal models, and in humans, SOM inhibits the proliferation of human lymphocytes, the production of immunoglobulins by B lymphocytes, and neutrophil chemotaxis.4 ,5 As an antagonist of substance P, SOM modulates neurogenic inflammation and pain perception.5 Receptors for SOM have been demonstrated on lymphocytes and macrophages and on the synovial membrane in patients with active RA.2 ,4 ,6 In vitro physiological concentrations of SOM have been shown to modulate aberrant synovial cell function in RA, inhibiting proliferation of synovial cells, interleukin 6 and interleukin 8 mRNA expression, and synthesis of these proinflammatory cytokines, as well as reducing the production of matrix metalloproteinases, MMP-1, MMP-2, and MMP-9.7 Other effects of SOM relevant to the treatment of RA are its analgesic properties and its ability to inhibit angiogenesis, thus potentially suppressing pannus formation.8 ,9 The native SOM hormone has been given in clinical trials intra-articularly or intravenously, where it suppressed the inflammatory process in RA and psoriatic arthritis, respectively.10 ,11
Owing to the multiple effects of SOM on the immune system and on the function of synovial cells, and its anti-angiogenic and analgesic properties, we suggested that treatment with an SOM analogue might have a beneficial effect in patients with RA.
The present 14 week pilot study was undertaken to evaluate the efficacy and safety of a long acting preparation of the somatostatin analogue, octreotide, in the treatment of 10 patients with longstanding RA who had failed to respond to multiple disease modifying antirheumatic drugs (DMARDs).
Patients and methods
PATIENTS
Inclusion criteria were age 18–70, fulfilment of the 1987 American Rheumatism Association criteria for RA,12 disease duration of ⩾3 years, and active disease with at least three of the following: six or more tender joints, six or more swollen joints, erythrocyte sedimentation rate (ESR) ⩾28 mm/1st h, or morning stiffness of at least one hour. All patients were required to have been treated previously with at least four DMARDs with an unsatisfactory response. Current DMARD treatment was kept stable at least three months before entry and throughout the study. Prednisone use was allowed at a dose of up to 10 mg/day, at a stable dose for at least one month before entry. Non-steroidal anti-inflammatory drugs and analgesics were allowed during the study, and doses were recorded.
Exclusion criteria were chronic renal failure or liver disease and severe deformities or secondary osteoarthritis interfering with clinical evaluation.
PROTOCOL
The protocol was approved by the Israeli Human Research Committee and all patients gave written informed consent before enrolment. Clinical and laboratory assessments were made at entry and at weeks 1, 2, 4, 6, 8, 10, 12, and 14.
Treatment
Sandostatin-LAR (Novartis, Basel, Switzerland) consists of octreotide acetate, a SOM analogue, incorporated into microspheres of a biodegradable polymer (poly-(dl-lactide-co-glycolide-glucose)), providing long term controlled release after a single intramuscular injection. Therapeutic levels of octreotide are obtained for a period of four weeks after injection.13 Sandostatin-LAR was given intramuscularly at a dose of 20 mg, once every four weeks (weeks 0, 4, 8).
Clinical assessment
A full physical examination was conducted at entry and at completion of the study. The following clinical efficacy variables were assessed: tender joint count (68 joints assessed), swollen joint count (66 joints assessed), global assessment of overall disease activity by doctor and patient, and patient evaluation of pain, using a 10 cm visual analogue scale (VAS), and physical function as assessed by the Lee questionnaire.14
The primary efficacy end point was the proportion of patients meeting the American College of Rheumatology (ACR) preliminary criteria for improvement in RA (ACR 20).15 Analgesic and non-steroidal anti-inflammatory drug use, prednisone dose, and adverse events were recorded at each visit.
Laboratory assessment
Laboratory studies included determination of ESR, C reactive protein (CRP), complete blood count, and blood chemistry at each visit.
Statistical analysis
A paired t test was used for parametric values and the Wilcoxon test for non-parametric values (SPSS, SPSS Inc software, Chicago, IL, USA). Statistical significance was accepted at p<0.05.
Results
Table 1 shows the baseline demographic and disease characteristics of the study patients. All the patients were women. Their mean age was 46.4 years (range 31–66) and the mean duration of RA was 17.7 years (range 6–30). Eight of the patients were rheumatoid factor positive. Patient 8 had a juvenile onset. The mean number of previous DMARDs was seven (range 4–10), including methotrexate in all patients, with a poor response. The median numbers of tender and swollen joints at baseline were 15.5 and 9.5 respectively. Mean (SD) ESR and CRP values at baseline were 39.10 (13.76) mm/1st h and 24.4 (16.7) mg/l, respectively.
Baseline demographic and disease characteristics of the study patients
During the study one patient required an intra-articular corticosteroid injection, one and eight weeks after entering the trial. The injected joint was counted as swollen and tender for the remainder of the study. This patient was a non-responder. Patient 9 received only two doses of the study drug because an urticarial rash appeared after the second injection. Patient 10 received only one dose owing to an unexpected trip. All the patients were included in the evaluation of safety and efficacy.
EFFICACY
Six of the 10 study patients achieved an ACR 20 response during the study period. Improvement was noted as early as two weeks after the beginning of treatment.
Two of the six responders continued to improve: patients 2 and 7 achieved an ACR 50 response at weeks 4 and 8 of the trial, respectively, while an ACR 70 response was achieved by patient 7 at week 12. Patient 10 did not achieve an ACR 20 response, though two weeks after beginning treatment the number of tender and swollen joints dropped from 33 and 15 to six and six, respectively. Marked improvement in her global assessment of pain and functional status was also noted. She withdrew from the trial after a single dose owing to an unexpected trip.
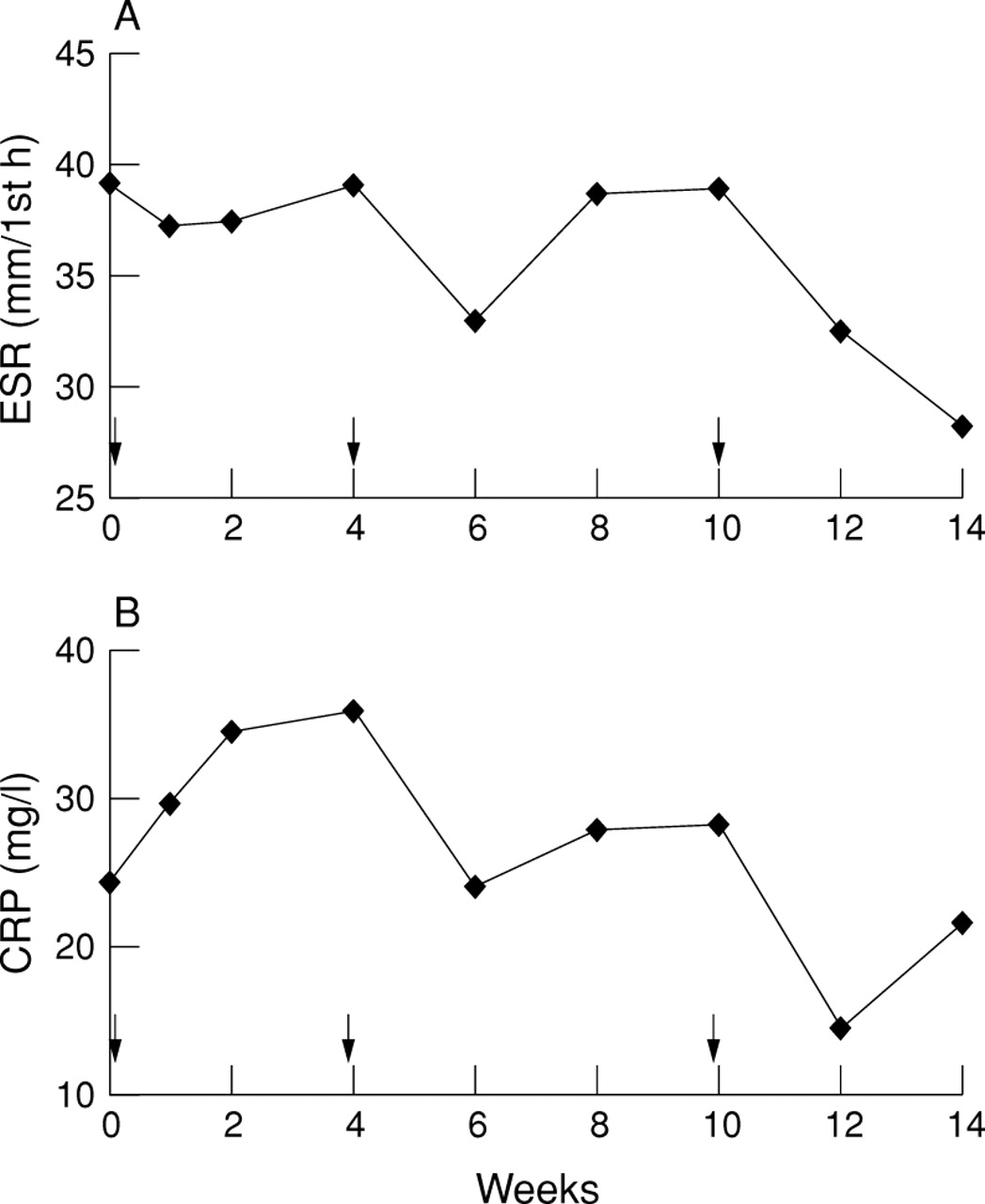
On evaluation of the 10 patients as a group, a significant improvement was noted at weeks 2, 8, and 10 of the study in the mean VAS of pain ( p<0.05), at weeks 8 and 10 in the mean doctor's global assessment of disease activity, and at weeks 6, 8, and 10 in the mean patient's global assessment of disease activity (p<0.05). Significant improvement in the mean number of swollen joints was noted at weeks 2 (p<0.01), 4, and 8 (p<0.05) (fig 1). There was a trend towards improvement in ESR and CRP values, though this did not reach statistical significance (fig 2). No statistically significant improvements in the mean number of tender joints or Lee functional index were recorded.

(A) Pain as assessed by the patients on a visual analogue scale (VAS). Statistically significant improvement was noted at weeks 2, 8, and 10 of the study. *p<0.05. (B) Global assessment of disease activity by the doctor and patients on a VAS. Statistically significant improvement was noted at weeks 8 and 10 of the study in the global disease activity as assessed by the doctor and at weeks 6, 8, and 10 as assessed by the patients. *Patient p<0.05; †doctor p<0.05. (C) Mean number of swollen joints during the study. Significant improvement was noted in the mean number of swollen joints at weeks 2, 4, and 8 of the study. *p<0.05; **p<0.01. Arrows indicate time of Sandostatin-LAR injections.

{kind=link}
{kind=link}
(A) Mean erythrocyte sedimentation rate (ESR); (B) mean C reactive protein (CRP) values for the 10 patients as a group during the 14 week study.
Patient 7 was able to reduce the dose of prednisone from 8 to 4 mg/day at week 10. This patient, who experienced marked improvement during the trial, had a flare of arthritis with fever 10 weeks after the last dose of the somatostatin analogue.
SAFETY
There were no major adverse effects. Six patients had bloating or mild diarrhoea, which subsided with continued treatment and a low fat diet. In one of these patients the diarrhoea was severe, accompanied by 3 kg weight loss, which resolved when the treatment was stopped. One patient developed an urticarial rash a week after the second injection, which resolved without treatment. One patient had a transient, mild increase of liver enzymes.
Discussion
In this pilot study the efficacy of a long acting somatostatin analogue was evaluated in 10 patients with refractory, active RA. Six patients responded, achieving an ACR 20 response. Two patients continued to improve up to an ACR response of 50 and 70, respectively. Statistically significant improvement was noted in the 10 patients, as a group, in the following parameters: mean number of swollen joints, mean VAS of pain, and global assessments of disease activity by patient and doctor. This improvement was noted for all four parameters at weeks 8 to 10 and declined by week 12. This response may be explained by the prolonged four week pharmacokinetic profile of Sandostatin-LAR.14 No statistically significant improvement was seen in the mean number of tender joints. Although there was a trend towards reduction of the mean ESR and CRP values of the 10 patients as a group, this did not reach statistical significance. This may be because of the small size of the study group and the large standard deviations, as seen in other trials evaluating treatment in RA.16 Although a decrease in ESR is expected to parallel clinical improvement, this observation is not universal. Indeed, ESR values assessed during cyclosporin treatment for RA were found to undergo little change in face of major improvements in clinical disease activity.17 Tugwellet al have assessed the relative efficiency of outcome measures to detect a treatment effect in placebo controlled trials. When comparing methotrexate or leflunomide with placebo, patient and doctor global assessments were found to be more sensitive than ESR, CRP, tender or swollen joint counts.18
Interestingly, subjective improvement, as assessed by the patients was noted earlier than that assessed by the doctor. This early sense of “wellbeing” may be attributed to the analgesic properties of SOM.8 ,11
Although this was a small pilot study, there seems to be a significant clinical effect of the treatment, more than would be expected from a placebo effect. Placebo arms of studies evaluating drug treatment in RA show a beneficial effect in 9–29% of the patients when employing ACR criteria.16 ,19 This is a much lower rate than the 60% response seen in our study. Moreover, Anderson et al have recently shown that female sex, prior DMARD use, worse functional class, and longer disease duration reduce the likelihood of patient response.19 These factors, which characterise our patients with refractory RA, should be taken into account when interpreting the results.
The results of this study, together with the immunomodulatory, antiproliferative, and anti-angiogenic effects of SOM, suggest a possible beneficial effect of somatostatin in the treatment of RA. Further large, placebo controlled studies are required to evaluate this drug as a potential DMARD for patients with RA.