Article Text

Abstract
OBJECTIVES To evaluate the effect of anti-TNFα on the Th1 and Th2 cytokines in patients with spondyloarthropathy (SpA).
METHODS Peripheral blood mononuclear cells (PBMC) were obtained from 20 patients with active SpA treated with infliximab (5 mg/kg). For comparison, PBMC were also obtained from 15 healthy controls and 19 patients with active rheumatoid arthritis (RA). After stimulation with PMA/ionomycin, the intracellular cytokines interleukin (IL)2, IL4, IL10, and interferon (IFN)γ were determined in CD3+ T cells and in CD3+/CD56+ natural killer (NK) T cells by flow cytometry.
RESULTS At baseline the percentage of T cells positive for IFNγ (p=0.020) and IL2 (p=0.046) was decreased in patients with SpA compared with healthy controls, while IL10 (p=0.001) was increased. This cytokine profile, confirmed by the mean fluorescence intensities (MFI), was more pronounced in CD3+/CD8– cells and contrasted with higher IL2 production in RA. NK T cells, characterised by high IL4 and IL10 numbers, were also increased in patients with SpA (p=0.017). Treatment with infliximab induced a significant and persistent increase in IFNγ and IL2 in patients with SpA. Moreover, there was a transient decrease in IL10 and NK T cells in patients with high baseline values, resulting in values comparable with those of healthy controls. This switch in cytokine profile was seen in both the CD3+/CD8– and CD3+/CD8+ subsets.
CONCLUSIONS Before treatment patients with SpA had an impaired Th1 cytokine profile compared with healthy controls and patients with RA. TNFα blockade induced restoration of the Th1 cytokines, resulting in a normal cytokine balance. These data confirm the effect of anti-TNFα on the immune changes in SpA, and provide insights into the mechanisms involved in TNFα blockade.
- spondyloarthropathy
- T lymphocyte
- cytokine
- anti-TNFα
Statistics from Altmetric.com
Analogous with the findings in mice, human CD4+ T cells are classically divided into two subsets with regard to their cytokine secretion: Th1 cells which mainly secrete IFNγ and IL2, and Th2 cells which are characterised by the production of IL4, IL5, and IL10.1 With regard to the distinct functional properties of Th1 and Th2 cells,2 Th1 polarisation has been implicated in the pathogenesis of autoimmune disorders including different forms of experimental and human arthritis, particularly rheumatoid arthritis (RA).3 ,4 However, Th1 polarisation has not been confirmed in spondyloarthropathy (SpA), a group of related chronic autoimmune diseases of the joint with common clinical, radiological, and genetic characteristics, and there is increasing evidence that SpA is functionally characterised by a Th2 cytokine profile.5-11
A recent open label pilot study evaluating the effect of anti-TNFα in SpA indicated a dramatic clinical improvement in both axial and peripheral joint inflammation.12 Since TNFα blockade influences T cell cytokines both in vitro13 and in vivo,14-16 the effect of TNFα blockade in SpA could partially be mediated by alterations in Th1 and Th2 cytokine production. The aim of the present study was therefore to investigate the effect of anti-TNFα on Th1 and Th2 cytokine production in patients with SpA, to confirm the impact on immune changes in SpA, and to provide insights into the mechanisms that could be involved in TNFα blockade in SpA. In addition to the cytokines IFNγ, IL2, IL4, and IL10, the study pays special attention to natural killer (NK) T cells. This T cell subset, which shares characteristics of both T cells and NK cells, is a potent cytokine producing cell population with an important regulatory function on Th1/Th2 immune responses.17 ,18
Subjects and methods
PATIENTS
Twenty one patients (17 men, four women) of median age 49 years (range 26–73) with SpA diagnosed according to ESSG criteria19 were treated in an open label pilot study with anti-TNFα antibodies. All patients had active disease defined by the presence of at least one swollen joint, one region of active tendinitis or dactylitis, or inflammatory spinal pain (typical “night pain”). Treatment with disease modifying antirheumatic drugs (DMARDs) was stopped at least 4 weeks before the start of the study; steroids and non-steroidal anti-inflammatory drugs (NSAIDs) remained at a stable dose throughout the study. All patients were treated with infliximab 5 mg/kg intravenously at baseline, week 2, and week 6. Detailed information about inclusion and exclusion criteria, treatment protocol, and clinical evaluations have been reported previously.12The demographic and clinical characteristics of the patients are summarised in table 1. Heparinised blood was obtained at baseline and on days 3, 7, 14 (before the second infusion), 28, 42 (before the third infusion), 56, 70, and 84. Since in one patient no blood sample could be obtained at baseline, the final analysis reported here includes only 20 of the 21 patients.
Demographic and clinical features of patients with spondyloarthropathy
Control blood samples were obtained from 19 patients with RA (five men, 14 women) of median age 48 years (range 35–75) who fulfilled the American College of Rheumatology criteria.20All patients had active disease defined by six or more swollen joints, 10 or more tender joints, and one of the following: morning stiffness for more than 45 minutes, C reactive protein (CRP) concentration of more than 20 mg/l, erythrocyte sedimentation rate (ESR) of more than 28 mm/1st h. Finally, blood samples were also obtained from 15 healthy controls (six men, nine women) of median age 43 years (range 21–58) in order to provide normal reference values. The study protocol was approved by the local ethical committee and all patients gave their informed consent.
LABELLING OF INTRACELLULAR CYTOKINES
Peripheral blood mononuclear cells (PBMC) were isolated from 10 ml heparinised blood by Ficoll-Paque 1077 gradient (Pharmacia, Uppsala, Sweden) centrifugation (30 minutes, 1800 rpm). The cells were washed in phosphate buffered saline (PBS; Gibco BRL, Grand Island, USA), resuspended in RPMI 1640 culture medium (Gibco), and stimulated with a combination of 25 ng/ml phorbol 12-myristate-13-acetate (PMA; Sigma, St Louis, MO, USA) and 1 μg/ml calcium ionophore ionomycin (Sigma) for 5 hours at 37°C. After 1 hour, 10 μg/ml brefeldin A (Sigma) was added to enhance flow cytometric analysis of intracellular cytokine staining by interfering with the function of the Golgi apparatus and thus inhibiting protein secretion. After stimulation the cells were washed and incubated for 30 minutes with 10 μl peridium chlorophyll protein (PerCP) or allophycocyanin (APC) conjugated monoclonal antibodies (mAbs) against the following phenotypic surface markers: anti-CD3 (Leu4, Becton Dickinson, San Diego, USA), anti-CD8 (Leu-2a, Becton Dickinson), and anti-CD56 (B159, Pharmingen, San Diego, USA). Isotype matched control mAbs labelled with PerCP and APC were used as controls. Subsequently, 2 ml lysing buffer (Becton Dickinson) was added for 10 minutes, the cells were centrifuged, and 500 μl of permeabilisation buffer (Becton Dickinson) was added for another 10 minutes. After washing with PBS (Gibco), the cells were incubated with fluorescein isothiocyanate (FITC) and phycoerythrin (PE) labelled mAbs against intracellular cytokines: anti-Hu IFNγ (25723.11, Becton Dickinson), anti-Hu IL2 (5344.11, Becton Dickinson), anti-Hu IL4 (3010.211, Becton Dickinson), and anti-Hu IL10 (JES3-9D7, Biosource Europe, Nivelles, Belgium) for 30 minutes. Again, isotype matched control mAbs were used to assess non-specific binding. Following a final washing step, the cells were resuspended in 300 μl CELLfix (Becton Dickinson) and kept at 4°C until analysis. All incubations were performed at room temperature and in the dark.
FLOW CYTOMETRY
The labelled cells were analysed by four colour flow cytometry (FACSort, Becton Dickinson) using Cellquest software (Becton Dickinson). T cells were selected using a forward and side scatter gate for lymphocytes in combination with a gate on CD3+ cells. Non-specific staining and autofluorescence were determined by the isotype matched controls. Since CD4 is downregulated by PMA/ionomycin stimulation, the CD3+ T cell subsets were determined by their expression of CD8: CD3+/CD8+ T cells and CD3+/CD8– T cells. The percentage and cytokine profile of NK T cells, identified as CD3+/CD56+ cells, were analysed separately.
STATISTICAL ANALYSIS
Values are expressed as median (range). The Kruskal-Wallis test was used to compare the cytokine profiles at baseline in the three groups (SpA, RA, and healthy controls). Where there were significant differences the exact p values were calculated using the Mann-Whitney U test and corrected for the number of comparisons. The paired Wilcoxon signed ranks test was used to compare the values after treatment with the values at baseline in the SpA group. Spearman'sr s test was used to calculate correlations. A p value of <0.05 was considered to be statistically significant.
Results
BASELINE CYTOKINE PROFILE OF PATIENTS WITH SpA VERSUS HEALTHY CONTROLS
The cytokine profile of CD3+ peripheral blood T cells in healthy controls (n=15) and SpA patients at baseline (n=20) is summarised in table 2. Both the percentage of positive cells and the mean fluorescence intensities (MFI) of IFNγ (p=0.020 and p=0.039, respectively) and IL2 (p=0.046 and p=0.020, respectively) were decreased in patients with SpA compared with healthy controls. In contrast, the number of IL10 positive T cells was clearly increased (p=0.001), paralleled by a slight but non-significant increase in MFI. There were no differences for IL4. The percentage of IL10 positive cells in SpA was inversely correlated with the percentage of IFNγ positive cells (r=–0.51, p=0.022) and the percentage of IL2 positive cells (r=–0.54, p=0.015). When the T cell subsets were analysed, the differences for IFNγ, IL2, and IL10 were even more pronounced in the CD3+/CD8– subset, while only IL10 was significantly different in the CD3+/CD8+ subset (data not shown).
Cytokine profile of CD3+ peripheral blood T lymphocytes in healthy controls (HC), patients with spondyloarthropathy (SpA) at baseline, and patients with rheumatoid arthritis (RA)
BASELINE CYTOKINE PROFILE OF SpA PATIENTS VERSUS RA PATIENTS
The cytokine profile of CD3+ T cells in patients with RA before treatment (n=19) is summarised in table 2. Although RA showed some similarities with SpA, including a decrease in IFNγ positive T cells (p=0.046) and an increase in IL10 positive T cells (p=0.000) compared with healthy controls, there were some important differences. Firstly, the percentage of T cells positive for IL4 was decreased in patients with RA compared with those with SpA (p=0.044) and healthy controls (p=0.008), with a similar trend for the MFI. Secondly, both the percentage of positive T cells and the MFI of IL2 in patients with RA were significantly increased compared with patients with SpA (p=0.006 and p=0.000, respectively). Thirdly, despite a similar percentage of positive cells, the MFI for IFNγ was increased in patients with RA compared with those with SpA (p=0.004). As in SpA, the observed differences were more pronounced in the CD3+/CD8– subset while in the CD3+/CD8+ subset the differences were only significant for IL10 (data not shown).
CONTRIBUTION OF NK-T CELLS TO HIGH IL10 IN SpA
A separate analysis of CD3+/CD56+ NK T cells was performed to assess the role of these cells in the Th1/Th2 cytokine balance in patients with SpA and RA. In healthy controls the CD3+/CD56+ subset had a manifest Th2 profile compared with the global CD3+ population: the percentage of cells positive for IFNγ (p=0.019) and IL2 (p=0.049) was decreased whereas cells positive for IL4 (p=0.000) and IL10 (p=0.000) were increased (table 3). Although only 1.6% (range 0.4–7.0%) of the T lymphocytes were CD3+/CD56+, this small subset constituted 16.4% (range 5.3–28.4%) and 18.3% (range 2.8–69.6%), respectively, of the T cells positive for IL4 and IL10. Accordingly, there was a significant correlation between the percentage of NK T cells and the percentage of IL10 positive cells in the global T cell population (r=0.59, p=0.028). Thus, NK T cells are a minor subset of peripheral blood T cells in healthy controls but contribute significantly to the Th1/Th2 balance by their strong Th2 profile. Analysis of the NK T cell subset in patients with SpA and RA at baseline resulted in two important observations. Firstly, the percentage of CD3+/CD56+ cells in the global T cell population was increased in SpA (4.6% (range 0.8–50.2%); p=0.017) and RA (4.7% (range 0.9–31.3%); p=0.018) compared with healthy controls (1.6% (range 0.4–7.0)), thereby parallelling the increase in IL10 in these two populations. Secondly, the cytokine profile of these NK T cells was also shifted towards Th2 in patients with SpA and RA (table 3). However, the percentage of NK T cells positive for IL4 was lower in patients with RA (3.0%, (range 0.2–14.4%)) than in healthy controls (13.2% (range 1.3–35.8%); p=0.001) and patients with SpA (11.1% (range 0.2–68.0%); p=0.036), which is of interest with regard to the global reduction of IL4 in RA.
Cytokine profile of peripheral blood CD3+ T cells and CD3+/CD56+ NK T cells in healthy controls (HC), patients with spondyloarthropathy (SpA) at baseline, and patients with rheumatoid arthritis (RA)
CORRELATIONS BETWEEN T CELL CYTOKINES AND CLINICAL ASSESSMENTS IN SpA
In order to explore the clinical relevance of the impaired Th1 profile in SpA, possible correlations were studied between T cell cytokines and a number of clinical features: CRP concentration, ESR, swollen joint count, tender joint count, physicians' global assessment of disease activity, patients' global assessment of disease activity, and patients' pain assessment. The number of IFNγ positive cells correlated inversely with CRP levels (r=–0.56, p=0.010), swollen joint count (r=–0.54, p=0.025), tender joint count (r=–0.53, p=0.027), and patients' global assessment of disease activity scored on a 100 mm visual analogue scale (r=–0.59, p=0.006; fig 1). Neither the T cell expression of other cytokines (IL2, IL4, and IL10) nor the number of NK T cells correlated significantly with any of these clinical parameters.

Relation between the percentage of IFNγ positive peripheral blood T cells analysed by flow cytometry and the patients' global assessment (100 mm visual analogue scale) in 20 patients with spondyloarthropathy. A significant inverse correlation was found (r=–0.59, p=0.006).
EFFECT OF ANTI-TNFα ON CYTOKINE PROFILE IN SpA
As indicated in table 4, TNFα blockade in SpA (infliximab 5 mg/kg intravenously given on days 0, 14, and 42) induced an increase in both the percentage of positive T cells and the MFI of the Th1 cytokines IFNγ and IL2. This increase was already apparent at day 3, became significant from day 7, and was maintained throughout the study. At day 84 the percentage of IFNγ and IL2 positive T cells (p=0.002 and p=0.001, respectively), as well as the MFI of both cytokines (p=0.004 and p=0.002, respectively), were strongly increased compared with baseline values. Moreover, there was no significant difference at day 84 of anti-TNFα treatment between the patients with SpA and healthy controls in percentage positive T cells (32.7%v 33.0%, p=0.79) and MFI (146.5v 153.0, p=0.74) of IFNγ. For IL2 there was even a slight increase in the treated patients compared with the healthy controls in both the percentage of positive cells (32.6%v 25.7%, p=0.033) and the MFI (125.9v 104.6, p=0.089). When the T cell subsets were analysed the increase in Th1 cytokines was observed in both the CD3+/CD8– and CD3+/CD8+ subsets (data not shown).
Cytokine profile of peripheral blood CD3+ T cells in patients with spondyloarthropathy at baseline (day 0) and during treatment with anti-TNF-α (infliximab 5 mg/kg intravenously on days 0, 14, and 42)
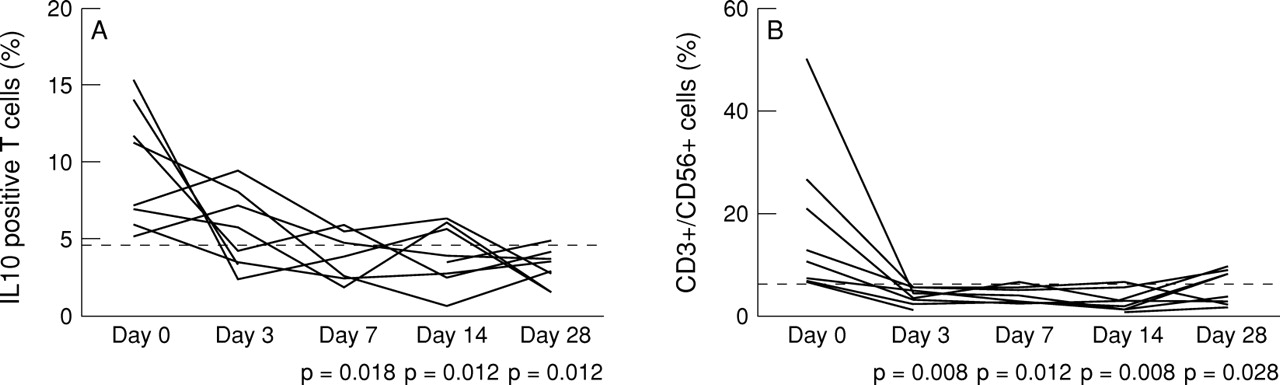
When the total group of patients with SpA was analysed, no significant changes were found in the Th2 cytokines IL4 and IL10 (table 4) nor in the number of CD3+/CD56+ NK T cells (data not shown). However, in the eight patients with raised baseline values of IL10 (9.28% (range 5.22–15.44%); mean + 2 SD of healthy controls considered upper limit of normal), there was a significant decrease in the percentage of IL10 positive cells at days 7, 14, and 28 of treatment with anti-TNFα (3.27% at day 28; fig 2A). The remaining 12 patients who had normal values at baseline (2.73% (range 0.87–4.65%)) maintained values within the normal range after treatment (2.85% at day 28). A similar phenomenon was observed for NK T cells; in the nine patients with high baseline values (10.19% (range 6.34–50.16%), again defined as more than mean + 2 SD of healthy controls) there was a significant reduction in the number of CD3+/CD56+ cells at days 3, 7, 14, and 28 compared with baseline values (4.23% at day 28; fig 2B), while the remaining 11 patients maintained normal values (data not shown). There were no significant differences in clinical characteristics between patients with high and low baseline values of IL10 and NK T cells. The changes in IL10 and NK T cells induced by anti-TNFα were transient as they lasted only until day 28.

{kind=link}
{kind=link}
Peripheral blood T cells of patients with spondyloarthropathy with high baseline values for IL10 and NK T cells were analysed by flow cytometry at baseline and at days 3, 7, 14, and 28 of treatment with anti-TNFα (infliximab 5 mg/kg on days 0, 14, and 42). The upper limit of normal values, defined as more than the mean + 2 SD of the healthy control group, is indicated by the dotted line. (A) Decrease in the percentage of IL10 positive cells in the CD3+ population in patients with high baseline values (n=8). (B) Decrease in the percentage of CD3+/CD56+ cells in the CD3+ population in patients with high baseline values (n=9).
Discussion
Challenging the classical concept that autoimmunity is associated with a Th1 cytokine profile, the present study indicates that peripheral blood T cells of patients with active SpA are characterised by low IFNγ and IL2 compared with healthy controls. Previous reports of low IFNγ and/or IL2 in peripheral blood7 ,8 as well as in the synovium9 ,10 and gut mucosa7 of patients with SpA confirm the relevance of this finding and refute the hypothesis that this cytokine profile in blood is secondary to a Th1 profile at the site of inflammation. In order to allow a direct comparison of the cytokine profile in SpA with that of another inflammatory joint disease, a group of patients with active RA was included in the study. In accordance with previous reports,10 ,21 ,22 these patients were characterised by higher IL2 production. In contrast, IFNγ production in RA was quite similar to that in SpA and was clearly less than in healthy controls, indicating that the differences in T cell cytokine profiles in SpA and RA are more complex than a classical Th1/Th2 polarisation.
With regard to the Th2 cytokines, patients with SpA had normal IL4 production whereas IL10 production was increased in both SpA and RA patients compared with healthy controls. Increased IL10 production in SpA is in line with reports which indicate a high expression of IL10 in psoriatic synovium23 and synovial fluid mononuclear cells in patients with reactive arthritis,6 as well as a correlation between disease activity and IL10 plasma levels in patients with SpA.5 Increased production of IL10 by T cells24 and non-T cells25 has also been reported previously in patients with RA. The high levels of IL10 were paralleled by an increase in the percentage of NK T cells, a T cell subset which has been implicated in the regulation of the Th1/Th2 balance17 ,18 and which plays a role in numerous autoimmune disorders.26-30 Indeed, this minor T cell subset appears to contribute significantly to the cytokine balance, with increased production of IL10 and IL4 in patients with SpA and increased IL10 production in patients with RA. The high numbers of IL10 producing T and non-T cells in different inflammatory conditions and the lack of correlation with IL4 question the classification of IL10 as a Th2 cytokine in humans. Instead, the findings support a role for IL10 as an anti-inflammatory cytokine implicated in an autoregulatory feedback loop aimed at counteracting the chronic inflammation by suppression of proinflammatory cytokine secretion and antigen presentation.31 ,32
The impaired Th1 cytokine production found in SpA is highly compatible with a prominent role of TNFα in the pathogenesis of the disease, as has recently been postulated based on the dramatic clinical improvement after TNFα blockade.12 Chronic exposure to high concentrations of TNFα is known to deactivate T cells directly and to reduce their cytokine production,13 and thus could account for the downregulation of T cell derived IFNγ and IL2. It is therefore of interest to study the effect of anti-TNFα on Th1/Th2 cytokine production in patients with SpA. Moreover, this cohort of patients appears to be a unique study model since there was no concomitant use of methotrexate or other DMARDs which might have influenced the cytokine balance.33 ,34 Treatment with three infusions of infliximab resulted in a rapid and sustained increase in the Th1 cytokines IFNγ and IL2, reaching levels comparable with those in healthy controls. In addition, there was a rapid reduction in IL10 and NK T cells in patients with high baseline values. However, this decrease was only seen in the first 4 weeks; the median IL10 value even tended to increase at week 12, while no effect was seen on IL4. This supports the view that TNFα blockade essentially reverses the state of “anergy” of Th1 cells while having no effect on Th2 cells in patients with SpA.
With regard to both the pathophysiological relevance of the impaired baseline Th1 cytokine production in SpA and the therapeutic relevance of its restoration by TNFα blockade, it seems important that low IFNγ correlates with higher disease activity—as evaluated by inflammatory parameters, joint swelling, and patients' global assessment of disease activity—and that the restoration of a normal Th1 response paralleled the clinical effect of anti-TNFα in all SpA patients.12 Furthermore, it has to be mentioned that different forms of SpA have been linked to bacterial infection. Since Th1 cytokines are known to play a crucial role in the immune response against intracellular bacteria,35 ,36 it has been postulated that a shift towards a Th2 cytokine profile contributes to the defective clearance of SpA associated bacteria.37 ,38The subsequent persistence of bacterial antigens39-41 is thought to lead to inflammation and/or autoimmunity,42possibly by triggering continuous TNFα production. In this perspective, restoration of normal Th1 cytokine production not only reflects the impact of TNFα blockade on the immune alterations in SpA, but could actively contribute to the therapeutic effect of TNFα blockade in patients with this condition.
Acknowledgments
The authors wish to thank Jenny Vermeersch and Annemie Herssens for their excellent technical contribution to the study.
References
Footnotes
Dominique Baeten and Nancy Van Damme contributed equally. Dominique Baeten is a FWO-Vlaanderen research assistant. The study was supported by a concerted action grant GOA96001 of the University of Ghent, Belgium.