Article Text

Abstract
OBJECTIVE In Europe giant cell arteritis (GCA) is more common in Scandinavian countries than in southern regions. Epidemiological studies on GCA in other more distant countries have indicated a progressive increase in incidence. A regular cyclical pattern in incidence of GCA over 20 years has been reported in Olmsted County (Minnesota, USA). In contrast, no cyclical fluctuation has been recently reported in Sweden. To investigate further the epidemiology of GCA in southern Europe the trend in incidence and fluctuations of this vasculitis over 18 years in the Lugo region of northwestern Spain were examined.
METHODS A retrospective study of biopsy proven GCA diagnosed between 1 January 1981 and 31 December 1998 at a single hospital for a well defined population of almost 250 000 people. Annual incidence was calculated for the whole group of patients and for men and women separately. Monthly variations, annual peaks of incidence, and trend in the incidence of biopsy proven GCA with and without polymyalgia rheumatica (PMR) were also examined.
RESULTS One hundred and sixty one Lugo residents were diagnosed with biopsy proven GCA between 1981 and 1998. The average annual incidence for the population aged 50 and older was 10.24/100 000 (men 11.00/100 000, women 9.57/100 000). A progressive increase in the incidence in both men and women was seen. In men there was an annual increase of 8% (95% CI 4% to 13%; p<0.0001). In women the annual increase was 11% (95% CI 5% to 17%; p<0.0001). The overall annual increase for men and women was 10% (95% CI 6% to 14%; p<0.0001). No seasonal pattern or peaks in the incidence were seen. During the period 1981–94 GCA was more common in men than in women. In contrast, during the last years of study the increase in incidence was higher in women. In women the annual ratio of incidence of GCA with PMR/incidence of GCA without PMR was generally higher than 1. However, in men the annual ratio was initially 1 but decreased gradually, indicating a progressive decrease in the proportion of men with biopsy proven GCA associated with PMR.
CONCLUSION In northwestern Spain there has been a progressive increase in GCA incidence. As seen in other countries where GCA is more common, during the past few years the increase in incidence has been mainly due to a higher number of new cases in women.
- giant cell arteritis
- temporal artery biopsy
- incidence
- trend
Statistics from Altmetric.com
Giant cell (temporal) arteritis (GCA) is a vasculitis of unknown cause, usually affecting large and medium sized vessels in the elderly.1-3 It is the most common systemic vasculitis in Western countries.4 ,5 In Europe GCA is more common in Scandinavian countries2 ,6 ,7 than in southern regions.5 ,8-10 Epidemiological studies on GCA in more distant countries have indicated a progressive increase in incidence.11-13 In the north of the United States, Salvarani et al reported a regular cyclical pattern in incidence of GCA over a 20 year period.14 In contrast, no cyclical fluctuation has been recently reported in Sweden.15 To investigate further the epidemiology of GCA in southern Europe we examined the trend and fluctuations of this vasculitis over an 18 year period in the Lugo region of northwestern Spain.
Patients and methods
All patients diagnosed with biopsy proven GCA, seen in the department of medicine of the Hospital Xeral-Calde (Lugo, Spain) between January 1981 and December 1998, were included in this study. The Hospital Xeral-Calde is the only referral centre for a mixed rural (60%) and urban population of almost 250 000 people living in the Lugo region of northwestern Spain. The main characteristics of the Lugo population have been reported elsewhere.5 ,16 This population is Caucasoid of Celtic origin,17 is relatively static, and no important migration has occurred in the area during the past two decades. In 1991 the population aged 50 and older in Lugo comprised 99 800 (men 46%; women 54%). It constituted 41% of the whole population of this area. In Lugo the average age of the population is greater than in the rest of Spain.18 During the past 10 years the population fell by 7500.
Patients with suspected GCA were sent to the hospital by general practitioners or they self referred to the emergency unit. A temporal artery biopsy was performed in all patients with clinical manifestations of GCA. Segments longer than 2.5 cm were generally obtained. In patients with polymyalgia rheumatica (PMR), without any clinical manifestation of GCA, biopsies were usually considered if patients had constitutional syndrome or the erythrocyte sedimentation rate (ESR—by Westergren's method) was greater than 80 mm/1st h, or both.18 ,19 Patients were diagnosed as having biopsy proven GCA if histological examination of the temporal artery showed interruption of the internal elastic laminae with infiltration of mononuclear cells into the arterial wall with or without giant cells.5 ,16 Patients were classified as having biopsy proven GCA associated with PMR if, in addition to the pathological abnormalities in the temporal artery described above, they met the following criteria: (a) aged 50 or older at the onset of symptoms; (b) severe and bilateral pain associated with morning stiffness (lasting at least 30 minutes) in at least two out of three areas: neck, shoulder, and/or pelvic girdles; (c) ESR at the time of diagnosis of at least 40 mm/1st h; and (d) exclusion of other diseases that may present with polymyalgia manifestations or mimic PMR except GCA.13 ,16 ,18 ,20 ,21
Twenty nine biopsy negative patients fulfilled the American College of Rheumatology (ACR) classification criteria for GCA.22 In these patients headache and PMR were common presenting symptoms. In contrast, abnormal temporal artery on physical examination, jaw claudication, and ischaemic visual manifestation were less common than in patients with biopsy proven GCA.23 Temporal artery biopsy samples were taken in 89 patients with PMR without any clinical manifestation of GCA. Only 8 (9%) had positive biopsy results. The positive/negative temporal artery biopsy ratio did not change significantly during the period of study.
STATISTICAL ANALYSIS
The target population was based on the census. The population distribution was provided by the Instituto Nacional de Estadística (INE). In the Lugo region, people grouped by age and sex were estimated by exponential interpolation from census data. In Spain the censuses were taken every 10 years when the last figure of the year was zero. More recently, censuses have been carried out in years whose last figure is 1. In addition, municipalities assess the population every five years. The population between censuses is established by extrapolation using the formula provided by the INE: Pt= P0 (1 + r)t, where Pt is the population to be calculated, P0 is the reference population, t is the time lag to be extrapolated, and r is the growth rate of the population during this period. Incidence rates standardised by age were calculated by a direct method using the European population as standard; the European standard was preferred to the World standard because it better represents a developed country's population. Rates are reported as cases for 105 population aged 50 or older. They were calculated from the number of new cases observed/the estimated population aged 50 and older. The annual incidence adjusted for age was calculated as a five year moving average reflecting the slow random changes. To analyse relations between age and calendar year (as explanatory variables) and GCA incidence rate (as outcome variable) three models were developed by Poisson regression.
The first one only considers age as explanatory and it assumes that the GCA incidence = exponential (β0 + β1×age); exponential (β1) would then be interpreted as the ratio corresponding to each year of age.
The second model assumes that the GCA incidence = exponential (β0 + β1×age + β2×calendar year); then exponential (β1) would be interpreted as before, and β2 as the rate ratio related to each calendar year.
Finally, the third model is the same as that used by Petursdottiret al 15 and assumes that the GCA incidence = exponential (β0 + β1×age + β2×calendar year + β3×calendar year2).
Goodness of fit of all three models were compared by the likelihood ratio. To analyse whether any season or any month of onset of symptoms in particular was more common, a χ2 test was used. This test was used to compare the number of cases observed and expected. To investigate if there were non-random peaks in the annual incidence, the actual number of annual cases was compared with the number of cases predicted by Poisson regression. All statistical analyses were performed with the software Stata Intercooled, release 6 (Stata Corporation, College Station, Texas, USA).
Results
The overall average annual incidence for the 18 year period was 10.24/100 000 people aged 50 and older (men 11.00/100 000, women 9.57/100 000). Table 1 shows the adjusted rates for the population aged 50 and older by age and sex. In both men and women biopsy proven GCA was more common in patients older than 70.
Average annual incidence of biopsy proven giant cell arteritis in Lugo (Spain). Number of cases by age and sex and incidence per 100 000 population aged 50 and older for the period 1981–98
Based on the second model described in “Patients and methods” the risk ratio (RR) per year in men was 1.08 (95% CI 1.04 to 1.13; p<0.0001). The RR per year in women was 1.11 (95% CI 1.05 to 1.17; p<0.0001). For men there was an annual increase in incidence adjusted by age of 8% (95% CI 4% to 13%; p<0.0001). In women the annual increase was 11% (95% CI 5% to 17%; p<0.0001). As a whole the overall annual increase for men and women was 10% (95% CI 6% to 14%; p<0.0001). The highest incidence in both men and women aged 50 and older was seen in 1998 (men 17.4/100 000 population, women 21.6/100 000).
No seasonal pattern was seen (p values for men 0.20, women 0.64, and total 0.32). Also, no increase of the incidence of GCA in any month in particular (considered as the month of onset of symptoms) was seen (p values for men 0.53, women 0.64, and total 0.57).
Figure 1 shows the incidence of GCA by sex. A progressive increase in the incidence was seen in both men and women. During the period 1981–94 GCA was more common in men. In contrast, during the last few years of the study the increase in incidence was higher in women. However, no peaks in the annual incidence of GCA were found.

Incidence of biopsy proven giant cell arteritis (GCA) by sex in Lugo, Spain (1981–98). During the period 1981–94 GCA was more common in men. However, during the last years the increase of incidence was higher in women.
In Lugo isolated PMR (not associated with GCA) is known to be more common in women.18 Because of this, we analysed GCA with and without PMR separately. Figure 2 shows that biopsy proven GCA associated with PMR was more common in men until 1987. Since then, there has been a trend towards an increase in the number of women with biopsy proven GCA associated with PMR. Likewise, until 1994 GCA without PMR was more common in men. Since then GCA without PMR has also been found to be more common in women (fig 3). To further investigate possible changes in the incidence of biopsy proven GCA associated or unassociated with PMR we examined the annual incidence of GCA with PMR/annual incidence of GCA without PMR ratio. Figure 4 shows that in most years the ratio in women was higher than 1 (more cases of biopsy proven GCA associated with PMR than those without PMR). In men, however, unlike women, the ratio was initially 1 but it has tended to decrease gradually and indicates the progressive decrease in the proportion of men with PMR.

Incidence of biopsy proven giant cell arteritis (GCA) associated with polymyalgia rheumatica (PMR) in Lugo, Spain by sex (1981–98). Since 1987 there has been a trend towards an increase in the number of women with biopsy proven GCA associated with PMR.

Incidence of biopsy proven giant cell arteritis (GCA) without polymyalgia rheumatica (PMR) in Lugo, Spain by sex (1981–98). Since 1994 GCA without PMR has been seen to be more common in women than in men.

Annual incidence of biopsy proven giant cell arteritis (GCA) with polymyalgia rheumatica (PMR)/annual incidence of GCA without PMR ratio in Lugo, Spain by sex (1981–98). In men, unlike in women, the ratio was initially 1 but has tended to decrease gradually and indicates the progressive decrease in the proportion of men with PMR.
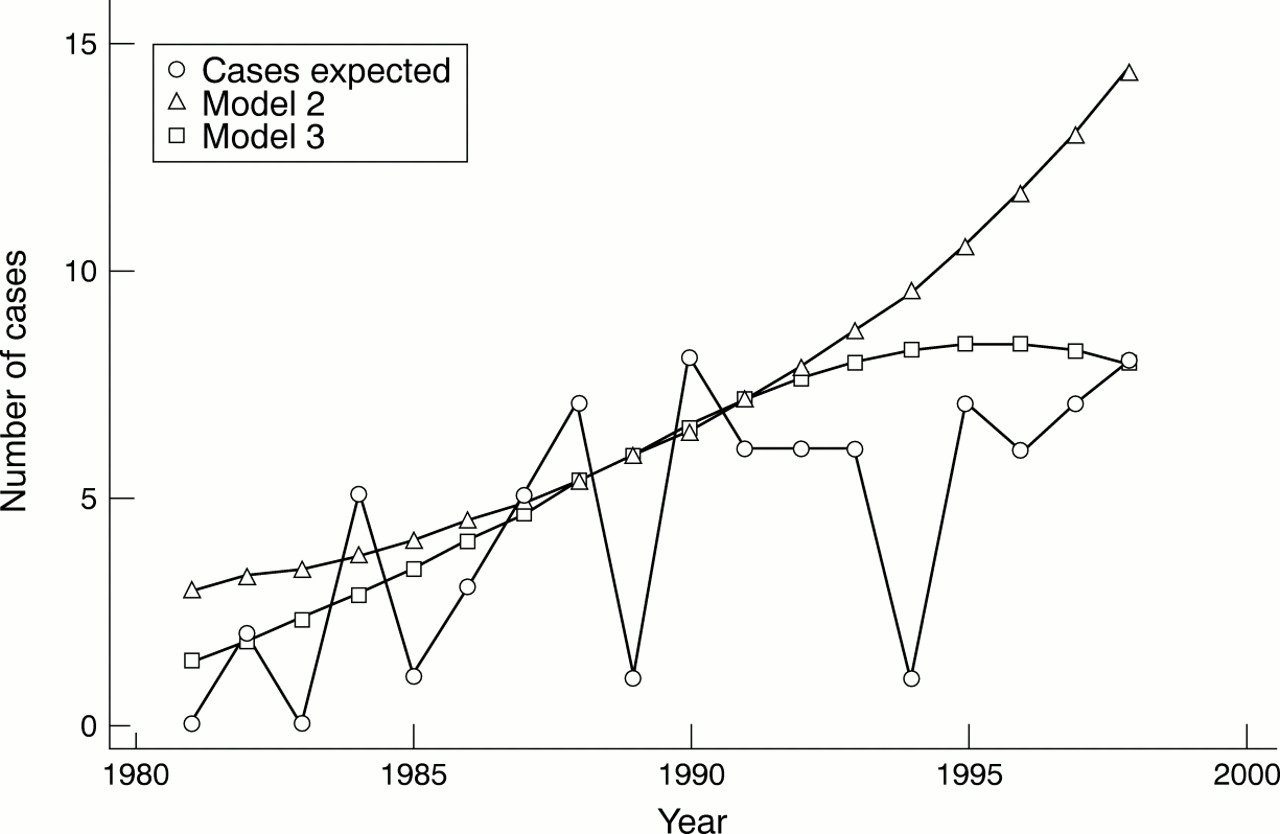
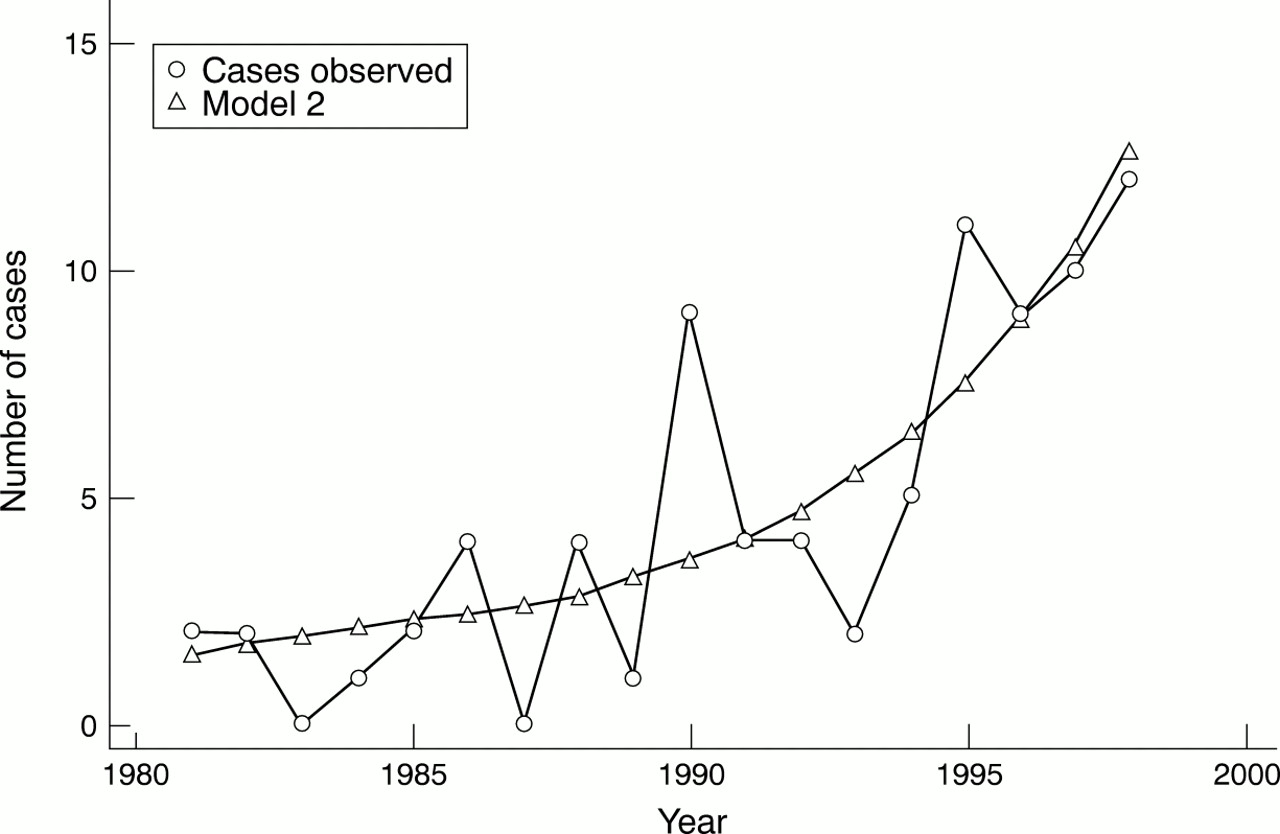
In women, the second model developed by Poisson regression that included age and calendar year as explanatory variables fits the data. Thus fig 5 suggests that new increases in GCA incidence are expected for women. Also, the addition of a third explanatory term (calendar year2) did not improve the goodness of fit. However, in men the second model did not adjust well, and it was necessary to include a calendar year2 term (third model). Figure 6 suggests that the peak of the incidence in men has been reached.

Number of biopsy proven giant cell arteritis (GCA) cases observed (circles) and those expected in women from Lugo, Spain (1981–98) by Poisson regression using as explanatory variables age and calendar year (triangles). The figure shows that new increases in GCA incidence are expected for women.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Number of biopsy proven giant cell arteritis cases (GCA) observed (circles) and those expected in men from Lugo, Spain (1981–98) by Poisson regression using as explanatory variables age and calendar year (triangles), and using age, calendar year, and calendar year2 (squares). The figure suggests that the peak of the incidence of GCA in men has been reached.
Discussion
Giant cell arteritis does not always require a positive temporal artery biopsy. As shown in patients with biopsy proven GCA, we have also seen a progressive increase in the incidence of patients with negative temporal artery biopsies who were classified as GCA according to the criteria proposed by the ACR. Moreover, as contralateral temporal artery biopsies were not considered in all cases if the first biopsy was normal, it is possible that some cases were missed because a positive temporal artery biopsy was a requirement for inclusion in this study.
The incidence of GCA is higher in Scandinavian countries and in Olmsted County, Minnesota, whose population has a Scandinavian background, than in other European countries.1 ,2 ,6 ,7 ,11 ,14 ,15 ,24 In these countries the annual incidence is generally higher than 20/100 000 people aged 50 and older. In southern Europe, in contrast, the incidence is lower than 12/100 000 people aged 50 and older.5 Within southern Europe differences in the incidence also exist. For example, in northwest Spain the incidence of GCA is almost twice as high as that seen in northern Italy.5 ,8 ,9
The incidence of GCA increases with latitude in the northern hemisphere, with at least a twofold increase in incidence in Scandinavian countries compared with Lugo. The present study, however, also supports a progressive increase in incidence in southern Europe. Such an increase has also been seen in Israel, a country traditionally considered to have a low incidence of GCA.12 As seen in other countries,11 ,15 the increase in the incidence of GCA in Lugo was associated with a constant relation between positive and negative biopsies.13 However, the rheumatologists from Lugo were puzzled by the predominance of GCA in men between 1981 and 1990.16 To our surprise, and unlike reports from other countries, the incidence of GCA in women during that decade was lower than in men. This could not be explained by sex differences in the structure of the population. However, although a progressive increase of the incidence in both sexes was found over this 18 year study, in the last few years the trend has been towards a higher increase in women. These observations have been found both in women with biopsy proven GCA associated with PMR and in those with GCA unassociated with PMR. Moreover, in the past few years the GCA associated with PMR in men has tended to decrease gradually. A declining trend in the annual incidence of GCA in men was also seen in Olmsted County and Israel.11 ,12 Variations in the annual incidence of GCA with peaks every seventh year have been reported in Olmsted County.14 However, in keeping with Petursdottiret al,15 no rhythmic pattern in the annual incidence of GCA was seen in the Lugo region. Ellinget al reported evidence of simultaneous fluctuations of the incidence of GCA and PMR in different regions of Denmark, suggesting an epidemic occurrence of a precipitating infectious agent.25 Seasonal distribution of the disease has also been reported. Based on the date of biopsy, peaks of incidence in late winter and autumn were found by Petursdottiret al.15 Also, based on the onset of symptoms, peaks of incidence were found during the summer months in Jerusalem (Israel) and England.12 ,26 In Scotland other peaks in January and May were seen by Jonassonet al.27 However, in this study we found no seasonal pattern for GCA distribution in Lugo.
Despite discrepancies in the presence of peaks of incidence and seasonal patterns among different studies, most investigations show a progressive increase in the incidence of the disease. A greater awareness of GCA may account for an increase in the diagnosis of cases in earlier stages of its natural history. Also, unknown environmental factors may play an important part in affecting the incidence of GCA as they may modulate the occurrence of the disease in a genetically predisposed population.
In conclusion, this study confirms a progressive increase in the incidence of GCA and a trend towards a greater increase of this vasculitis among women in southern Europe over an 18 year period.