Article Text

Abstract
OBJECTIVE To evaluate whether the Diff Quik (DQ) staining method might prove useful in identifying monosodium urate (MSU) and calcium pyrophosphate dihydrate (CPPD) crystals on permanent mounted stained slides.
METHODS 27 synovial fluid (SF) samples obtained from the knees of 21 patients with acute CPPD disease and 6 with acute gout were studied. Wet analysis for crystal detection and identification was performed within one hour of joint aspiration. In addition, 16 inflammatory synovial effusions obtained from patients with knee arthritis induced by non-crystalline inflammatory diseases were studied. For each SF, a DQ stained slide was analysed by two of the authors trained in SF analysis. The observers were blinded to the type of crystals present in the SF. Each slide was analysed by compensated polarised as well as transmitted light microscopy. An SF was considered positive if intracellular and/or extracellular crystals were clearly identified. In addition, the observer was asked to identify the type of the crystals using compensated polarised light microscopy. Sensitivity, specificity, accuracy, positive predictive value (PPV), and negative predictive value (NPV) of the DQ staining method were determined.
RESULTS 51 true positive and 28 true negative cases were correctly classified (39 CPPD samples, 12 MSU samples, 28 samples of crystal unrelated arthropathies). Overall, four false positive and three false negative cases were reported. In all the false positive cases, extracellular CPPD crystals were erroneously identified, whereas CPPD crystals present in the SF were not identified in the three false negative cases. All MSU specimens were correctly diagnosed. The overall specificity, sensitivity, and accuracy using DQ stained slides for crystal confirmation were respectively 87.5%, 94.4%, and 91.9%. The PPV was 92.7% and the NPV 90.3%. In particular, the specificity, sensitivity, and accuracy for CPPD detection were 90.9%, 92.9%, and 91.9%, with a PPV of 90.7 and an NPV of 93.0%. All the MSU specimens were correctly identified, providing 100% sensitivity, specificity, accuracy, PPV, and NPV.
CONCLUSIONS Stained preparations of SF, including DQ stained smears, could provide a useful tool for delayed SF analysis suitable for quality controls, including cytological examination and crystals detection and identification.
- synovial fluid
- Diff Quik
- monosodium urate
- calcium pyrophosphate dihydrate
Statistics from Altmetric.com
In clinical practice, detection and identification of monosodium urate (MSU) and calcium pyrophosphate dihydrate (CPPD) crystals in synovial fluid (SF) are usually performed on wet preparations with a polarising microscope fitted with a first order red compensator. By contrast, cytological examination and differential count are performed on stained preparations of both cytocentrifuge monolayers and smears of SF. However, crystal analysis and cytological examinations cannot be carried out at the same time because the staining technique commonly used for cytological studies might yield inaccurate results, owing to artefacts or solubilisation of crystals.1-4 This problem can be circumvented, as documented by Schumacher, by resorting to supravital staining using prestained slides that allow the simultaneous evaluation of pathological crystals and cytology.1
To date, crystal detection on stained preparations has received little attention.5 Recently, however, Petrocelli and coworkers6 demonstrated the usefulness of the Gram stain for MSU and CPPD crystal identification. Furthermore, this staining technique provides specimens which more than two years later still showed pathological crystals.
Our study aimed at evaluating whether smears of SF stained by Diff Quik (DQ; Dade Behring-Switzerland), an alcoholic, quick staining method for cytology, might prove useful for identifying MSU and CPPD crystals on permanent mounted slides.
Patients and methods
The study was conducted on 27 heparinised crystal induced synovial effusions collected over a six month period. All these effusions were crystal induced, as confirmed by the presence of intracellular and extracellular MSU and CPPD crystals. Twenty one SF samples were aspirated from the knee joints of 21 different patients with recurrent bouts of CPPD related arthropathy (pseudogout), and six SF samples were obtained from the knees of six patients with recurrent gouty arthritis. The patients with pseudogout had previously been diagnosed both by detecting the typical crystals in the joint effusions and by the presence of the characteristic radiological calcifications in their knees, whereas gouty arthritis had been diagnosed after identifying the birefringent negative, needle-like crystals in the SF by compensated polarised microscopy. In addition, we studied 16 inflammatory synovial effusions obtained from patients with knee arthritis due to non-crystalline inflammatory diseases. These SF samples were collected from our outpatients with a known rheumatic disorder, which had previously been diagnosed in accordance with the guidelines of the American College of Rheumatology (eight rheumatoid arthritis, one systemic lupus erythematosus, and seven seronegative spondyloarthropathy, including one ankylosing spondylitis, three psoriatic arthropathy, two inflammatory bowel disease related arthropathy, one reactive arthritis).
Wet analyses of the samples were performed within one hour of joint aspirations and the presence of crystals was assessed by our senior staff rheumatologist (RDS), who was aware of the clinical characteristics of the patients. Wet analyses were performed by analysing one slide obtained by placing a tiny drop of carefully shaken fluid onto a degreased slide and then gently coverslipped. Each slide was observed under transmitted light microscopy with the condenser diaphragm close down as narrowly as possible to enhance the refractivity of the crystals (“pseudophase” lighting), and under compensated polarised microscopy. The non-blinded observer confirmed the crystalline aetiology of the first 27 effusions, whereas no crystals were detected in the other 16 non-crystalline effusions. At least 30 adjacent microscopic fields of each slide were carefully scanned.
DQ preparations were obtained from an aliquot of the same SF. A thin smear of each SF was stained by the DQ method according to the data sheet recommendations. Briefly, the air dried smears were sequentially dipped five times in a methanol fixative solution, five more times in stain solution I (eosin G), then dipped five times in stain solution II (thiazine dye) and, finally, gently rinsed with distilled water. The overall staining process took about 15 seconds. The slides were then cleared in xylol and coverslipped with a non-aqueous mounting medium. Moreover, an aliquot of each SF was diluted with normal saline to obtain a final leucocyte concentration of 400 cells/ml. One hundred microlitres of the cell suspension were cytocentrifuged onto two degreased slides, air dried and, finally, stained by the DQ method.
A DQ stained smear of each SF specimen was blindly analysed by two of us (ES, SM) trained in SF analysis. Analysis was carried out using ×400 magnification and, if necessary, ×1000 magnification with an oil objective (Leika DMRB microscope). Each observer independently evaluated the slides of the SF and was given no more than five minutes for each slide to review the 43 DQ stained specimens. The SF samples were considered positive if intracellular or extracellular crystals, or both, were clearly identified. In addition, the observer was asked to identify the type of crystals using compensated polarised light microscopy. Sensitivity, specificity, accuracy, positive predictive value (PPV), and negative predictive value (NPV) of the DQ staining method were determined.
Results
Forty three SF samples were reviewed independently by the two observers, thus providing a total of 86 observations. Of these, 51 true positive and 28 true negative cases were correctly classified (39 CPPD, 12 MSU, 28 crystal unrelated arthropathy). In total, four false positive and three false negative cases were reported; a few extracellular CPPD crystals were erroneously identified in all the false positives, whereas in the three false negative cases intracellular CPPD crystals were not seen. The three false negative cases and one false positive case were misdiagnosed by observer 1, and the remaining three false positive cases were misdiagnosed by observer 2. The diagnoses that were false positive and false negative, respectively, were not made on the same slides by the two observers. All MSU specimens were correctly classified. The overall specificity, sensitivity, and accuracy for DQ stained slides for crystal confirmation were respectively 87.5%, 94.4%, and 91.9%. The PPV was 92.7% and the NPV 90.3%. In particular, the specificity, sensitivity, and accuracy for CPPD detection were 90.9%, 92.9%, and 91.9%, with a PPV of 90.7% and an NPV of 93.0%. All the MSU specimens were correctly identified, providing 100% sensitivity, specificity, accuracy, PPV, and NPV (table 1).
Results for monosodium urate (MSU) and calcium pyrophosphate dihydrate (CPPD) identification on Diff Quik stained smears of synovial fluid
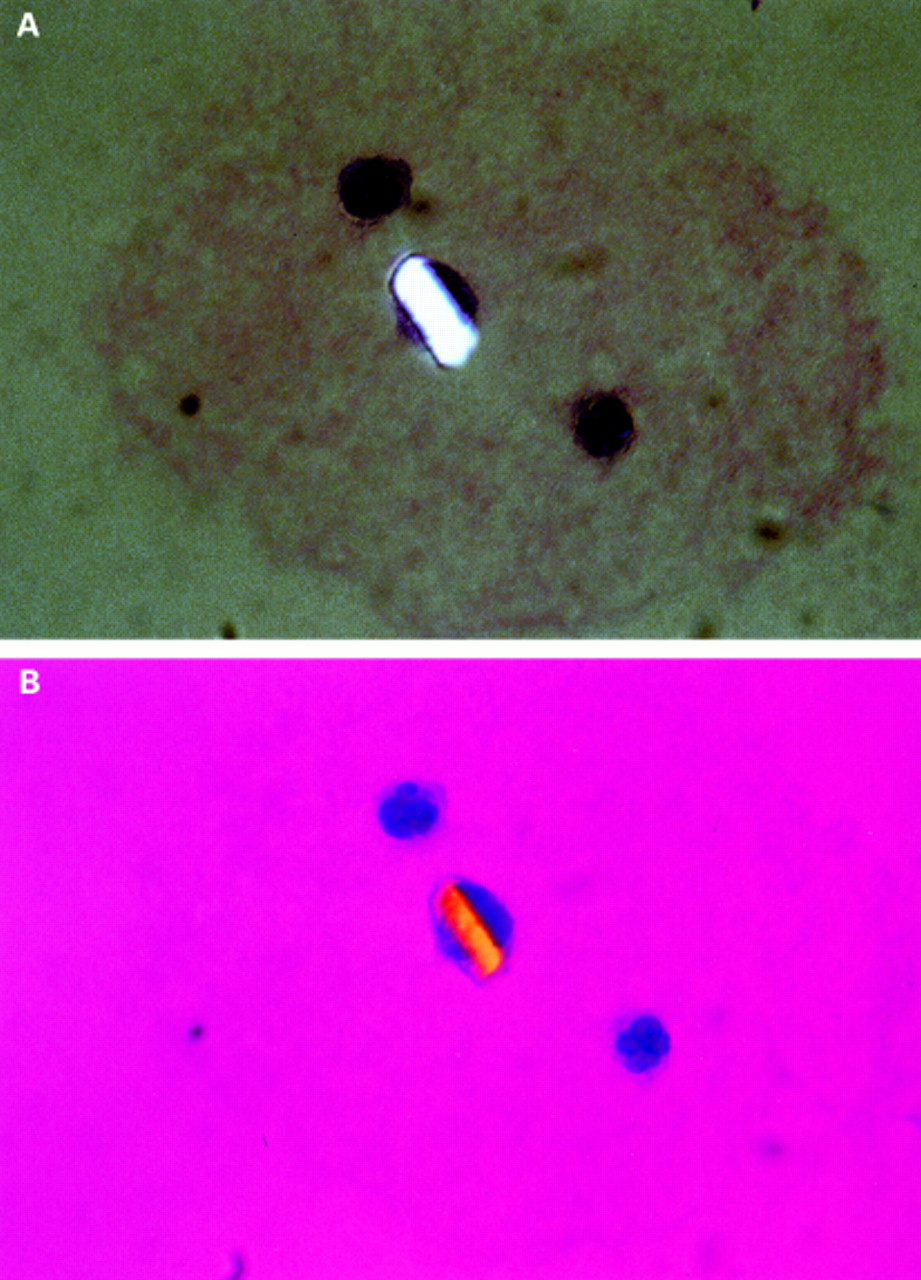
At the end of our study the reviewers, aware of the results, were asked, to re-evaluate on cytospin DQ stained preparations all the SF samples misdiagnosed in the blind study—that is, the four false positive and the three false negative cases. The detection and identification of crystals on the cytospin preparations proved extremely simple, showing several, well preserved intracellular and extracellular crystals (figs 1 and 2). The four false positive cases did not show birefringent CPPD-like particles in at least 20 adjacent microscopic fields.

Synovial effusion-cytocentrifuge monolayer preparation. An intracellular strongly birefringent monosodium urate crystal viewed in (A) polarised and (B) polarised, compensated light microscopy (Diff Quik (DQ) staining; original magnification ×100). The crystal is negatively birefringent. Neutrophils and lympho-mononuclear cells stained by DQ are easily recognisable.
{kind=link}
{kind=link}
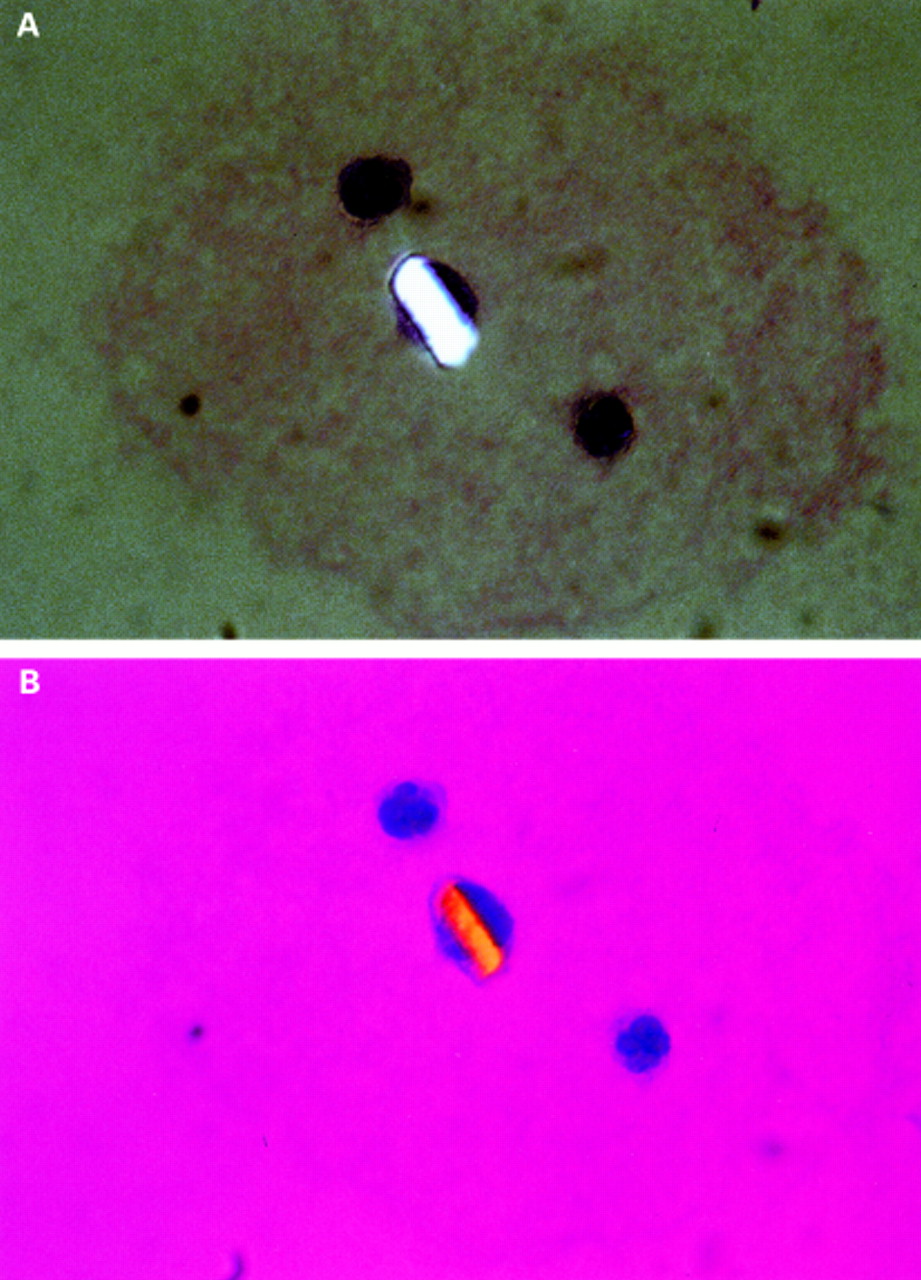
Intracellular crystal of calcium pyrophosphate dihydrate on a wet mount preparation seen by (A) polarising and (B) polarising compensated microscopy. The crystal is positively birefringent (Diff Quik staining ×100).
Conclusion
Our data showed that accurate results can be obtained from an analysis of DQ stained slides as shown by the excellent interobserver concordance in the evaluations carried out on wet slides. SF samples containing MSU crystals were easily identified, but in seven cases CPPD crystals were not correctly identified. Nevertheless, the four false positive smears of CPPD were classified as positive extracellular and none of these misdiagnosed fluids showed intracellular CPPD crystals. Therefore, it seems likely that the erroneous classifications were probably due to the presence of artefacts or dust contamination. By contrast, the SF samples misdiagnosed as false negative were characterised on wet preparations by low leucocyte counts with few, moderately birefringent intracellular and extracellular crystals. Thus the major difficulty in the blind study was to evaluate smears from fluids characterised by low cellularity and high viscosity as examined on wet preparations because cell and crystal density were further reduced on the DQ stained slides. Thus it would appear that the need to obtain thin smears suitable for the DQ stain might be responsible for such an apparent reduction. Nevertheless, our preliminary, non-blinded observations seem to indicate that cytospin DQ stained preparations may provide a further remarkable aid to detect crystals in synovial fluids with low cell count. Petrocelli et alhad the same problem in a similar study conducted using Gram stain6; sensitivity, specificity, NPV, and PPV were comparable with our results, and they concluded that stained SF smears yielded accurate results. In addition, the DQ stain also provides excellent preparations for differential counts and cytological studies of synovial effusions, thus allowing simultaneous visualisation of crystals and cellularity.
A quality control standard for SF analysis is mandatory.7-9 The gold standard for the diagnosis of MSU and CPPD crystal induced arthropathy is the identification of such crystals in synovial effusions by wet mount methodology. Wet mount preparations viewed under ordinary and compensated polarised light microscopy permit crystal detection and identification. Nevertheless, the poor reproducibility of SF analysis, particularly for crystal identification, has drawn the attention of rheumatologists to the need for quality control systems and reference laboratories.
Wet analysis is a valuable essential bedside procedure in daily clinical practice, but a correct SF analysis requires analysis by specifically trained personnel and should be conducted within a few hours from joint aspiration. By contrast, the possibility of storing stained specimens of SF for long periods, which could be also suitable for crystal analysis, might promote and enhance quality controls systems among laboratories. In our study it is noteworthy that crystals could still be easily identified on our slides 12 months after the end of our study. Thus, in conclusion, our opinion is that wet mount methodology is the gold standard for crystal detection and identification and that stained preparations of SF, including DQ stained smears, might provide a useful tool for delayed analysis suitable for cytological examination and for crystals identification.
Acknowledgments
Many thanks to Dr Nicolò Pipitone and Dr Gabriele Cevenini for helpful comments.