Article Text

Abstract
Objective To investigate how antibodies against anti-tumour necrosis factor (anti-TNF) agents influence response after switching from infliximab to adalimumab in rheumatoid arthritis (RA).
Methods This cohort study consisted of 235 patients with RA, all treated with adalimumab. At baseline 52 patients (22%) had been previously treated with infliximab (‘switchers’), and 183 (78%) were anti-TNF naive. Disease activity (using the 28-joint count Disease Activity Score (DAS28)) and presence of antibodies against infliximab and adalimumab were assessed. Clinical response to adalimumab was compared between switchers and anti-TNF naive patients and their anti-infliximab and anti-adalimumab antibody status.
Results After 28 weeks of adalimumab treatment the decrease in DAS28 (ΔDAS28) for the 235 patients was 1.6±1.5 (mean±SD). Anti-adalimumab antibodies were detected in 46 patients (20%). ΔDAS28 was 1.8±1.4 in patients without anti-adalimumab and 0.6±1.3 in patients with anti-adalimumab (p<0.0001). Thirty-three of the 52 switchers (63%) had anti-infliximab antibodies. Patients with anti-infliximab more often developed anti-adalimumab than anti-TNF naive patients (11 (33%) vs 32 (18%); p=0.039). ΔDAS28 was greater for anti-TNF naive patients (1.7±1.5) than for switchers without anti-infliximab antibodies (ΔDAS28=0.9±1.4) (p=0.009). ΔDAS28 for switchers with anti-infliximab was 1.2±1.3 and did not differ significantly from anti-TNF naive patients (p=0.262).
Conclusion Switchers with anti-infliximab antibodies more often develop antibodies against adalimumab than anti-TNF naive patients. Response to adalimumab was limited in switchers without anti-infliximab antibodies, which raises the question whether a second anti-TNF treatment should be offered to patients with RA for whom an initial treatment with an anti-TNF blocker fails, in the absence of anti-biological antibodies.
Statistics from Altmetric.com
Introduction
Biological agents directed against tumour necrosis factor (TNF) have greatly improved the treatment of chronic inflammatory diseases, such as rheumatoid arthritis (RA), ankylosing spondylitis, Crohn's disease and psoriasis. However, in RA, the proportion of patients who do not respond to anti-TNF treatment is substantial and varies between 30% and 40%.1,–,3 The lack of response can partly be explained by an immunogenic antibody response against these drugs, but there are also non-responding patients in whom an immunogenic reaction cannot be demonstrated.4 5 Lack of response to TNF blockade in these patients might to a certain extent be related to mechanisms that are not primarily driven by TNF.6 7 Hence, there seem to be different types of non-responders with different underlying pathogenic mechanisms causing non-response. Currently, these mechanisms and their consequences are not completely understood and it is unclear whether patients for whom one TNF blocker fails should switch to another TNF antagonist or to a drug with a different mechanism of action.
At present three TNF antagonists are available for the treatment of RA: infliximab, adalimumab and etanercept; their mechanisms of action have recently been reviewed in great detail.8 Personalised treatment regimens in the field of TNF blocking treatment are still far from optimal and most importantly, the factors influencing treatment outcomes in individual patients are unclear.6 9 In RA it is common to try another TNF blocker after treatment with the first has failed. Previous studies on switching from one TNF blocker to another after non-response have focused on whether switching was useful or not.10,–,13 These studies have also shown that there is considerable variation in response after switching; however, the contributing factors influencing this response have not been investigated.
To achieve a better understanding of factors determining response after switching from one TNF blocker to another, we prospectively studied a cohort of consecutive patients with RA receiving adalimumab treatment, for some of whom prior treatment with infliximab had failed. We compared clinical response as well as anti-antibody formation for infliximab–adalimumab switchers and TNF blockade naive patients. The ultimate goal is to understand the variation in clinical response after switching in different patient groups and to identify these different types of (non-) responders.
Patients and methods
Patients
Between February 2004 and February 2006, 255 consecutive patients with RA were included in a prospective observational cohort at the outpatient clinics of the departments of rheumatology of the Jan van Breemen Institute and the Academic Medical Centre in Amsterdam. All patients fulfilled the American College of Rheumatology 1987 revised criteria for RA,14 and had active disease, indicated by a disease activity score in 28 joints (DAS28) of ≥3.2 despite earlier treatment with two disease-modifying antirheumatic drugs (DMARDs), including methotrexate (MTX), at a dosage of 25 mg weekly or at the maximal tolerable dosage, according to the Dutch consensus statement on the initiation and continuation of TNF blocking treatment in RA.15 Patients were treated with either adalimumab and concomitant DMARD treatment or adalimumab monotherapy. All patients used adalimumab 40 mg subcutaneously every other week. In patients with an inadequate response as judged by the treating rheumatologist, the dosing frequency of adalimumab could be increased to 40 mg/week.
Eligible patients for this study were all patients who had previously been treated with infliximab and anti-TNF naive patients. A total of 235 patients fulfilled these criteria; 52 of these patients had previously been treated with infliximab, and are referred to as ‘switchers’, and 183 were anti-TNF naive patients. The study was approved by the medical ethics committee of the Slotervaart Hospital, BovenIJ Hospital, the Jan van Breemen Institute and the Academic Medical Centre/University of Amsterdam. All patients gave written informed consent.
Clinical response to adalimumab
Disease activity was assessed at baseline and after 4, 16 and 28 weeks of treatment using the DAS28 score. Clinical response was assessed by the decrease in DAS28 score (ΔDAS28) and the European League Against Rheumatism (EULAR) response criteria.16 The 52 patients who had previously been treated with infliximab and for whom infliximab was stopped were qualified as non-responders to infliximab.
Measurement of antibodies against infliximab and adalimumab
Serum samples were collected at baseline and just before an injection with adalimumab after 4, 16 and 28 weeks. The presence of anti-infliximab antibodies was determined at baseline before the start of adalimumab. The presence of anti-adalimumab antibodies was determined at all time points between baseline and 28 weeks. Anti-infliximab and anti-adalimumab antibodies were detected by radioimmunoassay as more extensively described previously.4 5 17 The assays measure specific high avid IgG antibodies against adalimumab and infliximab by an antigen binding test. Serum (1 µl/test) was preincubated with Sepharose-immobilised protein A (1 mg/test; Pharmacia, Uppsala, Sweden) in Freeze buffer (Sanquin, Amsterdam, The Netherlands). Non-bound serum components were removed by washing before 50 µl of 125I-labelled F(ab)′2 fragment of adalimumab/infliximab was added. 125I F(ab)′2 fragment of adalimumab/infliximab was added as two separate incubations. After overnight incubation, non-bound radiolabel was washed away and Sepharose-bound radioactivity was measured. Test results were converted into arbitrary units per millilitre (AU/ml) by comparison with dilutions of a reference serum. The mean cut-off value was set at 12 AU/ml, which was derived from 100 healthy donors. Assay specificity was demonstrated by the absence of anti-adalimumab in 25 serum samples containing high-titre anti-infliximab antibodies. In the assays we did not find cross reactivity. Recently, patient serum samples were tested in a bioassay, which confirmed the specificity and validity of the radioimmunoassay.17
Statistical analysis
For statistical analysis SPSS version 16.0 was used. For differences between groups we used the independent samples t test, Mann–Whitney test or χ2, as appropriate. To investigate the influence of confounders on ΔDAS28 a multiple regression analysis was used. The threshold for significance was set at p<0.05.
To analyse clinical response in patients with and without antibodies after 28 weeks of treatment we used last observation carried forward for patients who stopped treatment owing to non-response or adverse events, and for patients who had received increased dosing frequency.
Variables considered potential confounders were chosen from all available baseline variables and were determined for every analysis specifically, based on differences between groups included in the analysis (table 1). Variables were included in the regression model as confounders if the β changed 10% or more after inclusion of the variable. Additionally, adjustments for possible intermediates were made.
Demographic and clinical characteristics at baseline
Results
Patient characteristics
Patient characteristics are shown in table 1. Of the 235 patients, 52 patients had received infliximab treatment before the start of adalimumab. The median period between the last infliximab administration and the first adalimumab injection was 47 weeks, interquartile range (IQR 11–102). Of the 235 patients enrolled in the study, 230 (98%) completed 16 weeks of adalimumab treatment, and 217 (92%) were still receiving adalimumab treatment at week 28. Before 28 weeks, eight patients (3%) stopped owing to treatment failure, nine (4%) because of adverse events and one was lost to follow-up. Twelve patients (6%) had an increased dosing frequency before 28 weeks to 40 mg adalimumab a week; in these patients the last DAS28 before dose increase was carried forward to 28 weeks.
Clinical response
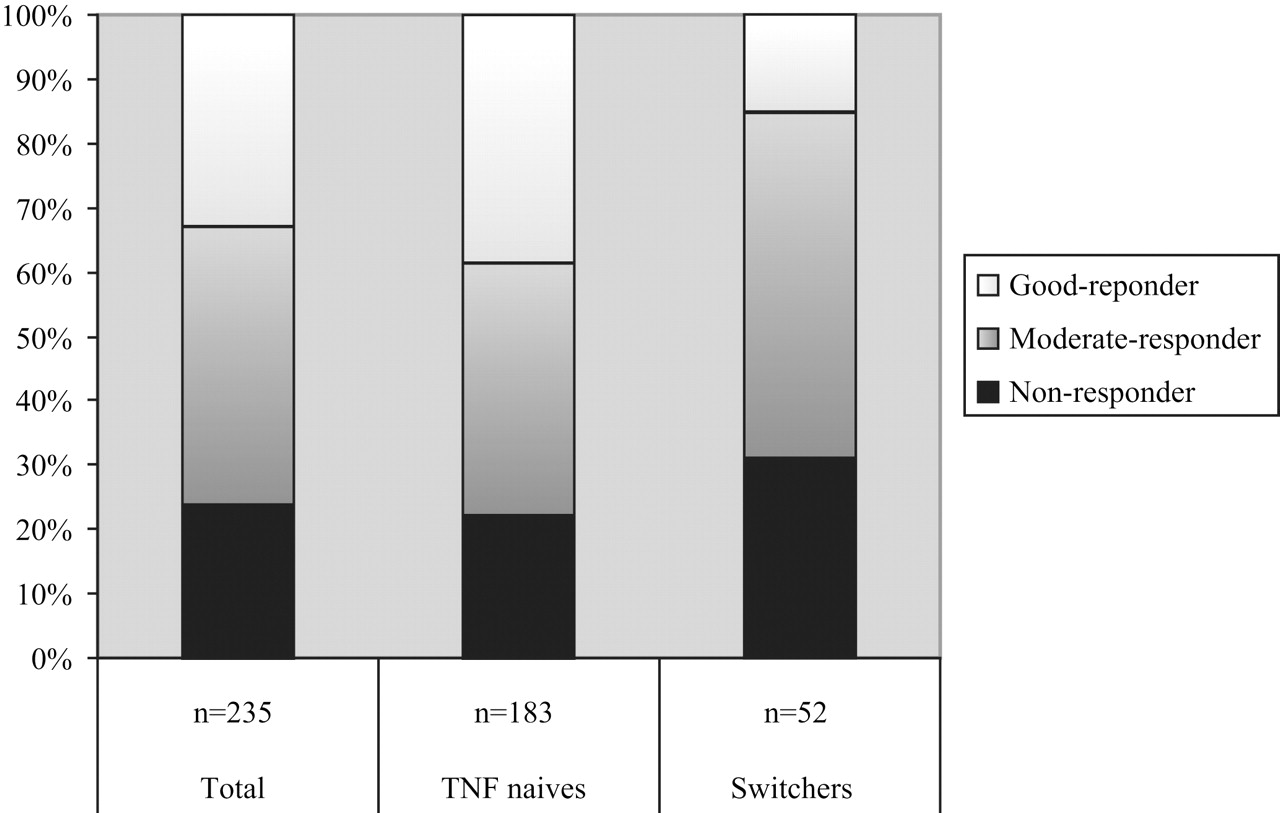
The mean decrease in DAS28 after 16 weeks of adalimumab treatment for the whole patient population was 1.7±1.4. There were 55 (23%) non-responders, 95 (40%) moderate responders and 85 (36%) good responders according to the EULAR response criteria. After 28 weeks of adalimumab treatment the mean decrease in DAS28 was 1.6±1.5. There were 57 (24%) non-responders, 100 (43%) moderate responders and 78 (33%) good responders at that time point (figure 1).

{kind=link}
The EULAR response in anti-tumour necrosis factor (anti-TNF) naive patients and switchers. Of the 235 patients, 57 (24%) were non-responders, 100 were moderate responders (43%) and 78 were good responders (33%). Of the 183 anti-TNF naive patients, 41 (22%) were non-responders, 72 were moderate responders (39%) and 70 were good responders (38%). Of the 52 switchers, 16 patients were non-responder (31%), 28 were moderate responders (54%) and 8 were good responders (15%).
There was a difference in response between anti-TNF naive patients and patients who were treated with infliximab before adalimumab treatment. The improvement in DAS28 was larger for anti-TNF naive patients than for infliximab switchers (ΔDAS28 1.7±1.5 vs 1.1±1.4; p=0.007) in a univariate analysis, and after adjustment for confounding variable DAS28 at baseline in multivariate regression analysis (95% CI −1.166 to −0.351; p<0.0001).
Among the anti-TNF naive patients 38% were good responders, 39% were moderate responders and 22% were non-responders.In the infliximab-switchers group 15% of the patients were good responders, 54% were moderate responders and 31% were non-responders (p=0.008; figure 1).
Post hoc analysis showed that only the percentage of good responders was significantly different between anti-TNF naive patients and infliximab switchers (p=0.002).
Immunogenicity
Anti-adalimumab antibodies were determined in 233 patients; for two patients appropriate serum samples were not available. During 28 weeks' follow-up, anti-adalimumab antibodies were detected in 46 patients (20%). Mean ΔDAS28 was 1.8±1.4 in patients without anti-adalimumab antibodies and 0.6±1.3 in patients with anti-adalimumab antibodies (p<0.0001) (table 2). After adjustment for the confounding variable erythrocyte sedimentation rate (ESR), the difference remained significant (95% CI −1.797 to −0.908; p<0.0001).
Frequency of anti-ADA antibodies and clinical response (ΔDAS28) after 28 weeks of adalimumab treatment
Thirty-three of the 52 patients in the infliximab switcher group tested positive (63%) for anti-infliximab antibodies at baseline. Patients with anti-infliximab antibodies significantly more often formed anti-adalimumab antibodies (n=11, 33%) than anti-TNF naive patients (n=32, 18%; p=0.039). Nineteen infliximab switchers did not have anti-infliximab antibodies, three of these 19 (16%) formed antibodies against adalimumab. Switchers with anti-infliximab antibodies more often formed anti-adalimumab antibodies than switchers without anti-infliximab antibodies, but this difference did not reach statistical significance (p=0.170) (table 2).
Of all patients without anti-adalimumab antibodies 89% used concomitant MTX treatment compared with 54% of the patients with anti-adalimumab antibodies (p<0.0001).
Immunogenicity and clinical response
Improvement in DAS28 was significantly greater for anti-TNF naive patients than for switchers without anti-infliximab antibodies (p=0.016) and greater than for switchers with anti-infliximab antibodies; however, this difference did not reach statistical significance (p=0.079; table 2). After adjusting for confounding variables prednisone dose and DAS28 at baseline, the difference in ΔDAS28 for anti-TNF naive patients compared with switchers without anti-infliximab antibodies remained (95% CI −0.934 to −0.096; p=0.017), but the trend towards significance disappeared for the difference in ΔDAS28 when anti-TNF naive patients were compared with switchers with anti-infliximab antibodies (95% CI −1.410 to 0.316; p=0.210). Since the presence of antibodies against infliximab was associated with a higher frequency of anti-adalimumab antibody formation we performed an additional adjustment for the possible intermediate anti-adalimumab; the difference in ΔDAS28 for anti-TNF naive patients compared with switchers without anti-infliximab antibodies remained (95% CI −0.881 to −0.136; p=0.008) and the p value for the difference in ΔDAS28 for anti-TNF naive patients compared with switchers with anti-infliximab antibodies remained similar (95% CI −1.155 to 0.374; p=0.311).
Clinical response to adalimumab did not differ significantly between prior infliximab-treated patients with and without anti-infliximab antibodies (p=0.356). Adjustment for prednisone dose, DAS28 at baseline and number of prior DMARDs (95% CI −1.861 to 2.032; p=0.928) and additional adjustment for anti-adalimumab status ((95% CI −1.972 to 1.900; p=0.969) did not influence this.
Examination of the EULAR response to subsequent adalimumab treatment for switchers without anti-infliximab antibodies showed that there were no good responders and 42% of the patients were non-responders.
Discussion
The results from this study show that formation of antibodies against adalimumab is associated with a diminished treatment response in patients with active RA. Second, our data indicate that switchers with anti-infliximab antibodies more often form antibodies against adalimumab than anti-TNF naive patients. Finally, there are different types of non-responders, which may be relevant in the context of individualised medicine.
These data underscore initial data that immunogenicity against monoclonal antibodies is associated with a diminished response.5 Several studies have shown a relationship between the development of antibodies against infliximab and a diminished response to treatment in Crohn's disease, ankylosing spondylitis and RA.4 18,–,20
Data on the immunogenicity of humanised and ‘fully human’ monoclonal antibodies are still limited. However, it is becoming more and more clear that these antibodies can also cause a clinically relevant immune response. Three studies have shown an association between anti-adalimumab antibodies and a diminished clinical response in RA.5 20 21 Approximately 6% of the patients receiving natalizumab, a humanised monoclonal antibody against cellular adhesion molecule α4-integrin approved for the treatment of multiple sclerosis and Crohn's disease, developed persistent antibodies to the drug with subsequent loss of efficacy.22 Our data contribute to the evidence that all biologically active molecules, even being ‘fully human’ or humanised, injected into humans can incite immune reactions, leading to antidrug antibody formation. This antidrug immune response leads to immune complex formation (therapeutic drug antibody bound to antidrug antibody) which may promote the rapid clearance of the drug resulting in low trough levels.23
An important question is why an immunogenic response is triggered in some patients but not in others. Concomitant immunosuppressive treatment is an important factor in reducing immunogenicity.4 5 18 Current data confirm that concomitant MTX reduces the risk of forming anti-adalimumab antibodies. This might be of significance for the treatment of diseases where it is not common to give concomitant MTX—for example, in the treatment of psoriasis and ankylosing spondylitis. An important new finding from this study is that patients who previously formed antibodies against infliximab are more likely to develop antibodies against adalimumab. There are three possible explanations why people develop antibodies against both drugs. Cross reactivity between the assays seems a logical explanation, but this could not be demonstrated. It is more likely that some patients are more prone to develop an immune response, possibly related to the genetic background. Another option is that too low dosing could lead to immunogenicity, and high dosing to the induction of immunotolerance. Initially, every patient receives the same dosage of infliximab or adalimumab, but in some patients with high levels of biologically active TNF the standard dose may be too low. For example, for infliximab there was more anti-infliximab antibody formation in the patient group receiving 1 mg/kg compared with the 10 mg/kg group.24 High levels of biologically active TNF could lead to patients with a high disease activity at baseline having a greater risk of developing antidrug antibodies, however, the baseline characteristics of our patient groups do not support this hypothesis.
The data show that anti-TNF naive patients had a better response to adalimumab treatment than prior infliximab non-responders. Prior infliximab non-responders without anti-infliximab antibodies had the least improvement with subsequent adalimumab treatment. Previous studies on switching biological agents also identified different patient groups based on their response after switching; patients in whom there was primary failure of previous infliximab treatment (that is, no response/intolerance, unlike secondary failure—that is, loss of response) had a poor response to subsequent adalimumab treatment.10,–,12 It was suggested by some that there may be a subpopulation of patients with RA that does not respond to anti-TNF treatment.11 13 Further evidence for the latter is given by a study that showed that high levels of circulating TNFα bioactivity was associated with a good clinical response to infliximab.7 A possible explanation is that TNF may not be the crucial cytokine instigating RA in primary non-responders to anti-TNF treatment. Another study showed that responders to infliximab had a significantly higher synovial TNF expression and significantly more infiltration by TNF-producing inflammatory cells than non-responders.6
Results from our study show that in clinical practice adalimumab is effective in the majority of patients with RA who have previously been treated with infliximab. However, effectiveness differs for different types of patient groups. From our results a first step can be made in defining these patient groups based on their immunogenic reaction towards anti-TNF treatment. The clinical response to subsequent adalimumab for patients with anti-infliximab antibodies (who probably had low serum infliximab levels during infliximab treatment) did not differ significantly from that of TNF naive patients. Prior infliximab non-responders without anti-infliximab antibodies (who did not respond to infliximab despite presumably adequate infliximab levels) had a significantly worse response to subsequent adalimumab than anti-TNF naive responders. We could not demonstrate a difference in response between switchers with and without anti-infliximab in a direct analysis, but this is probably owing to a type II error. Most switchers without anti-infliximab antibodies did not respond to subsequent adalimumab despite not having anti-adalimumab antibodies. Since immunogenicity did not cause non-response in these patients, it is possible that these patients are refractory to anti-TNF treatment. Therefore, our study suggests that non-responders to TNF blockers should be treated differently according to their anti-drug antibody status. Antibody-positive patients probably benefit most from switching to a less immunogenic drug acting on the same principle, or from optimising concomitant DMARD (MTX) treatment. Furthermore, it is likely that in non-responders without anti-TNF blocker antibodies it is more useful and cost-effective to start treatment based on a mechanism of action other than TNF blockade.
This study is limited by the number of patients and the consequences of the observational cohort study design. The patient population had severe RA: long disease duration and many prior DMARDs; therefore, possibly, treatment effects are more difficult to detect. Patients with persistent joint damage may experience less benefit from treatment than patients with early RA. Owing to the interval between the last infliximab administration and the first adalimumab injection it might be that the frequency of anti-infliximab antibodies is higher than the level we measured. However, we did not find an association between the length of the interval and the presence of anti-infliximab antibodies (data not shown). In addition to these limitations, our study provides unique insight into the role of immunogenicity in treatment with biological agents. In daily practice in RA switching to another biological agent after non-response is often a random decision rather than an evidence-based decision. To our knowledge, this is the first study providing more information on the underlying mechanisms contributing to the possible success of switching. Further studies are necessary to provide more conclusive data on this subject. However, we show that determining the immunogenic status of a non-responding patient may be important for further decision-making and might assist in developing an optimised treatment for the individual patient.
Acknowledgments
We thank Els de Groot for preparation of the rabbit anti-idiotype and Henk de Vrieze and Kim van Houten for performing the assays. We acknowledge the research nurses Marga Kammeijer-Rippen and Margot P Colombijn for performing clinical assessments. In addition, this investigation was also facilitated by the Clinical Research Bureau of the Jan van Breemen Institute. Finally, the authors would like to thank Marieke J H J Dekker for critically reading the manuscript.
References
Footnotes
GMB and CAW contributed equally.
-
Funding The clinical part of this study was partially financed by Abbott and Wyeth. CAW was supported by grant number 945-02-029 from the Netherlands Organisation for Health Research and Development (ZonMw) to PPT. The study sponsors had no involvement in the study design; in the collection, analysis, and interpretation of data; in the writing of the report; and in the decision to submit the paper for publication.
-
Competing interests BACD, PPT and WFL are members of the advisory board of Abbott and BACD and PPT have received honoraria for lectures. PPT has served as a consultant to Abbott, Amgen, Centocor, Schering-Plough, UCB and Wyeth.
-
Ethics approval The study was approved by the medical ethics committee of the Slotervaart Hospital, BovenIJ Hospital, the Jan van Breemen Institute and the Academic Medical Centre/University of Amsterdam.
-
Provenance and peer review Not commissioned; externally peer reviewed.