Article Text

Abstract
Objectives: To determine whether changes in levels of anti-cyclic citrullinated peptide (anti-CCP) and rheumatoid factor (RF) are associated with the spontaneous improvement of rheumatoid arthritis (RA) during pregnancy and with the subsequent flare post partum.
Methods: Disease activity scores from the Pregnancy-induced Amelioration of Rheumatoid Arthritis (PARA) study of 118 patients were available for analysis. Before conception (if applicable), at each trimester and at 6, 12 and 26 weeks post partum, levels of the autoantibodies anti-CCP, IgM-RF, IgG-RF and IgA-RF were determined. Responses in disease activity were classified according to European League Against Rheumatism (EULAR) response criteria during pregnancy and post partum, and associated with the presence or absence of autoantibodies.
Results: The median levels of anti-CCP and all subclasses of RF during pregnancy were stable, whereas post partum the levels of anti-CCP, IgM-RF and IgA-RF declined. A significantly higher percentage of women without autoantibodies (negative for anti-CCP and RF) improved compared with women positive for either or both autoantibodies (75% vs 39%, p = 0.01). The occurrence of a flare post partum was comparable between these groups.
Conclusions: Improvement of disease activity of RA during pregnancy was not associated with changes in levels of autoantibodies during pregnancy, however, improvement may occur more frequently in the absence of anti-CCP and RF.
Statistics from Altmetric.com
Pregnancy is the only natural situation where improvement of rheumatoid arthritis (RA) occurs and flares after delivery.1 Insight into this mechanism may increase our knowledge on pregnancy-induced remission and also contributes to a better understanding of pathogenic mechanisms underlying RA in general.
Evidence for B cells and autoantibodies in the pathogenesis of RA is accumulating,2 3 especially for those autoantibodies directed against cyclic citrullinated peptides (anti-cyclic citrullinated peptide (CCP)).4 Other evidence in support of B cells is derived from clinical studies demonstrating improvement of disease activity upon treatment with B cell targeted therapies.5 However, it is not known whether improvement during pregnancy and flare after delivery is associated with changes in levels of anti-CCP and rheumatoid factor (RF); nor whether the presence of these autoantibodies may predict the clinical course of RA during and after pregnancy. In this study, levels of anti-CCP and RF in pregnant patients with RA were determined, and associations between antibodies and clinical features were assessed.
Patients and methods
Patient population
The current study is embedded in the Pregnancy-induced Amelioration of Rheumatoid Arthritis (PARA) study, a prospective cohort study on pregnancy and RA.1 For the present analysis data were collected between May, 2002 and November, 2006. Only data of women available from before pregnancy or first trimester until 26 weeks post partum onwards were used. Women who had a miscarriage were not included. No woman was included twice.
Data collection
Patients were visited before conception (prepregnancy), at each trimester (8–12, 20 and 30 weeks of gestation) and three times post partum (6, 12 and 26 weeks). At each visit serum was stored for determination of autoantibodies and disease activity was measured. Presence of RF, anti-CCP and erosions were ascertained from patient medical records.
Determination of autoantibodies
In all sera, levels of antibodies were measured, anti-CCP by ImmunoCAP EliATM CCP test (Phadia AB, Uppsala, Sweden). A level above 10 U/ml was considered as positive. IgM-RF, IgG-RF and IgA-RF were measured by ELISA (HYCOR Biomedical, Garden Grove, California, USA). For each subclass of RF, the level above which only 5% of healthy controls were tested as positive, was defined as the cut-off level; IgM-RF >24 IU/ml, IgG-RF >40 IU/ml and IgA-RF >30 IU/ml. In the present study, a positive RF was defined as the presence of one or more subclasses above cut-off level.
Determination of disease activity
Disease activity was calculated using the 28-joint Disease Activity Score (DAS28) with three variables consisting of a swollen joint count, a tender joint count and a C-reactive protein (CRP) level (mg/litre) (DAS28 CRP 3).1 6 7
Data analysis
Patients were classified as positive either when the presence of an autoantibody was reported in medical records, or when the autoantibody was tested positive at first visit. All other patients were classified as negative. Levels of autoantibodies are expressed as median (interquartile range (IQR)).
To determine whether changes in autoantibody levels between first and third trimester were associated with improvement of RA during pregnancy, patients were classified for their clinical response according to the European League Against Rheumatism (EULAR) response criteria during pregnancy (see Supplementary material).6 8 Since the baseline requirement for these criteria is that patients have an initial DAS28 of at least 3.2, analyses could only be performed on a subgroup of patients.
Disease activity course post partum was defined according to the “reversed” EULAR response criteria of disease activity of RA (see Supplementary material).1 Since there was no baseline requirement, the classification could be applied to all patients.
Changes in disease course during pregnancy and post partum were determined in women who were classified according to the presence of autoantibodies: “both negative”, “either anti-CCP or RF positive” and “both positive”.
Statistical analysis
Changes in autoantibody levels within patients were compared using the Wilcoxon test, while changes between different subgroups were compared using the Mann–Whitney U test. Disease course in presence or absence of autoantibodies was compared using the χ2 test or the Fisher exact test. A two-sided p<0.05 was considered statistically significant. SPSS for Windows (Chicago, Illinois, USA) V.15.0 was used for analysis.
Results
Demography
Data of 118 pregnancies, of which 59 were collected from before pregnancy, were obtained and are shown in table 1.
Demographics and clinical parameters of 118 patients with rheumatoid arthritis (RA)
Autoantibody levels and disease course
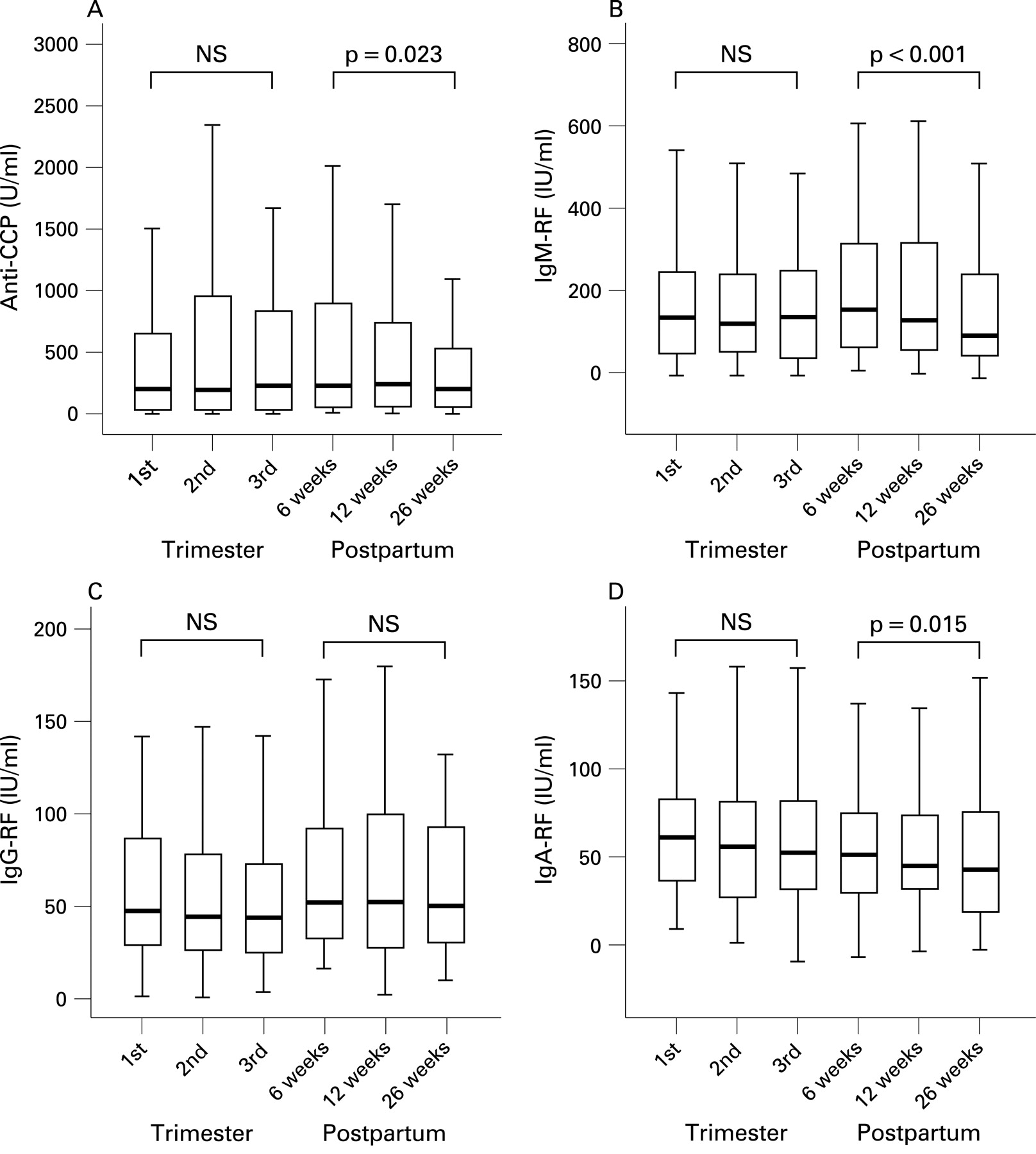
In fig 1(A–D) the courses and median levels with IQR of autoantibodies during pregnancy are shown. Only levels of patients who were positive for a certain autoantibody are shown. No statistically significant changes in median levels were present during pregnancy. Post partum, however, median levels of all autoantibodies, except IgG-RF, decreased by statistically significant amounts.
{kind=link}
Box plots of levels of autoantibodies in women with rheumatoid arthritis (RA) during pregnancy and post partum (n = 118). A. Levels of anti-cyclic citrullinated peptide (CCP) (n = 73); B. Levels of IgM-rheumatoid factor (RF) (n = 86); C. Levels of IgG-RF (n = 39); D. Levels of IgA-RF (n = 41). Each box represents the 25th to 75th centiles; lines inside the boxes represent the medians. Lines outside the boxes represent the 10th and 90th centiles. Statistical analyses were performed by Wilcoxon tests (NS, not significant).
Since autoantibody production might be influenced early in pregnancy, data of 59 women visited before pregnancy were analysed separately. No statistically significant changes were found between median autoantibody levels before pregnancy and at first trimester (see Supplementary material), or between disease activity at these time points (mean DAS28 CRP 3 of 3.8 and 3.7, respectively).
Changes in levels of anti-CCP and subclasses of RF at first and third trimester were not associated with disease course during pregnancy. The median differences in autoantibody levels during pregnancy for “responders” and “non-responders” are shown in the Supplementary material.
Post partum the largest change in anti-CCP level was measured either between 6 and 12 weeks post partum or between 6 and 26 weeks post partum. Changes in levels of anti-CCP and RF were not associated with a flare post partum. The median changes in autoantibody levels post partum for “flare” and “no flare” patients are shown in the Supplementary material.
Presence of autoantibodies and disease course
Finally, patients (n = 118) were classified as being positive or negative for a certain autoantibody. In some women anti-CCP (n = 2) or RF (n = 10) was documented as positive in medical charts, although they tested negative at first visit. Neither the presence of anti-CCP, nor of any RF was more likely to be present in responders during pregnancy or in patients with a flare post partum (all p>0.05). However, in subsequent analysis on patients classified for autoantibodies as “both negative” compared with patients classified as “either/or” or “both positive” (see table 2), the percentage of responders during pregnancy of the first group was significantly higher (75% vs 39%, p = 0.01). Comparable results were obtained when classification of the autoantibody status was made only by autoantibodies measured at first visit. Post partum, presence of autoantibodies was not associated with flares (p = 0.42).
Patients characteristics and disease activity responses classified according to presence of anti-cyclic citrullinated protein (CCP) and rheumatoid factor (RF)
Discussion
In this large prospective study of pregnant patients with RA, levels of anti-CCP were measured during pregnancy for the first time. Anti-CCP levels remained stable during pregnancy, even in women with spontaneously improved disease activity. As reported previously in smaller studies, similar results were obtained regarding RF.9 Post partum, however, when medication was resumed, levels of all autoantibodies, except IgG-RF, declined. These results are comparable with previous studies upon start of antirheumatic therapy.10 11 12 The changes in the measured autoantibody levels, however, were not associated with the disease course during and after pregnancy. But, surprisingly, women who were negative for both autoantibodies were more likely to improve during pregnancy.
The lack of association between levels of autoantibodies and disease course during pregnancy brings the study design into question, however we feel the following three points are valid:
The number of patients included seems sufficient, since a statistically significant decline in autoantibody levels (anti-CCP, IgM-RF and IgA-RF) was observed post partum.
In analogy with previous studies outside pregnancy,11 disease activity in the present cohort may be too well established to demonstrate changes in autoantibody levels. However, subgroup analysis on only patients with recent (<2 years, n = 19) RA also failed to demonstrate a decline in autoantibody levels during pregnancy.
Medication use hardly changed during pregnancy in our cohort, (reported previously),1 so this is unlikely to have biased our results.
The finding that women who were negative for both autoantibodies are more likely to improve during pregnancy, supports the hypothesis that RA is a heterogeneous disease with different pathogenic mechanisms involved.13 In analogy with systemic lupus erythematosus (SLE), where presence of autoantibodies together with increased Th2-mediated responses during pregnancy, may make that disease flare during pregnancy,14 one can speculate that similar mechanisms are responsible for the observation that disease activity is less likely to improve during pregnancy in patients with RA with autoantibodies (anti-CCP and/or RF).
Although a decline in levels of autoantibodies does not seem to be involved in the phenomenon of pregnancy-induced remission of RA, involvement of other functions of B cells and autoantibodies might still be relevant. These functions, that could be influenced by pregnancy, include the production of (inflammatory) cytokines and chemokines, antigen presentation and the formation of ectopic lymphoid tissue.2 Furthermore it has been shown that during pregnancy the pathogenicity of autoantibodies is modified by changes in glycosylation of IgG.15 This may have a role in the pregnancy-induced remission of RA, because the glycosylation of IgG determines its ability to bind to complement and to Fc receptors.
In conclusion, in the world’s largest cohort of pregnant patients with RA, no association was found between improvement of disease activity during pregnancy and changes in levels of autoantibodies. However, in the absence of anti-CCP and RF, improvement of RA during pregnancy occurred more frequently. Further investigations will be needed to discover whether improvement during pregnancy is related to other roles of B cells beyond autoantibody production.
Acknowledgments
We thank all patients and Dutch rheumatologists for their voluntary contribution to the PARA study, as well as Fleur van de Geijn and Esther Gasthuis and research assistants, for their help in data collection and all laboratory workers for their excellent technical assistance in laboratory research. Finally we thank Sten Willemsen (Erasmus MC, Department of Biostatistics) for his advice regarding the statistical analyses.
REFERENCES
Supplementary materials
Web Only Data 69/2/420
Files in this Data Supplement:
Footnotes
▸ Additional data (supplementary files 1–3) are published online only at http://ard.bmj.com/content/vol69/issue2
Funding This study was funded by the Dutch Arthritis Association (“Reumafonds”).
Competing interests None.
Ethics approval The protocol was approved by the Medical Ethics Committee of the Erasmus MC, University Medical Center Rotterdam, Rotterdam, The Netherlands. All patients gave written informed consent.
Provenance and Peer review Not commissioned; externally peer reviewed.