Article Text

Abstract
Background: Rheumatoid arthritis (RA), psoriatic arthritis (PsA) and other spondylarthritides impose a great impact on the individual in addition to the costs on society, which may be reduced by effective pharmacological treatment. Industry-independent health economic studies should complement studies sponsored by industry.
Objective: To study secular trends in baseline health utilities in patients commencing tumour necrosis factor (TNF) blockade for arthritis in clinical practice over 7 years; to address utility changes during treatment; to investigate the influence of previous treatment courses; to study the feasibility of health utility measures and to compare them across diagnostic entities.
Methods: EuroQoL 5 dimensions (EQ-5D) utility data were collected from a structured clinical follow-up programme of anti-TNF-treated patients with RA (N = 2554), PsA (N = 574) or spondylarthritides (N = 586). Time trends were calculated. Completer analysis was used.
Results: There were weak or non-significant secular trends for increasing baseline utilities over time for RA, PsA and spondylarthritides. The maximum gain in utilities had already occurred after 2 weeks for all diagnoses and remained stable for patients remaining on therapy. The first and second anti-TNF courses performed similarly.
Conclusions: Utilities at inclusion remained largely unchanged for RA, PsA and spondylarthritides over 7 years. Improvement occurred early during treatment and not beyond 6 weeks at the group level. Improvement during the first course was not consistently greater than the second. There were no major differences between RA, PsA and spondylarthritides. EQ-5D proved feasible and applicable across these diagnoses. These “real world” data may be useful for health economic modelling.
Statistics from Altmetric.com
Societal costs of rheumatoid arthritis (RA), psoriatic arthritis (PsA) and other spondylarthritides are substantial1 and indirect costs predominate. Effective treatment for these diseases, preventing disability, should therefore be beneficial for society. On the other hand, the new effective biological therapies (blockers of tumour necrosis factor (TNF), IL-1, T-cell costimulation and B-cell depletors) are costly. Therefore, the cost effectiveness of these drugs has been subject to health economic studies.2 3 However, many studies on cost effectiveness rely upon clinical trial data4 5 6 with their limited generalisability, and not on observational data from daily clinical practice.7 8 Furthermore, several diagnoses from the same setting are rarely reported, and health utilities are derived from measures such as the health assessment questionnaire (HAQ)9 10 in RA.11 12
Changes in the indications for treatment with biological agents can be anticipated when used in clinical practice, as physicians become more familiar with them. This could result in secular changes in baseline utilities as well as a change in their improvement during treatment. Indeed, we and others have reported changes in baseline characteristics towards lower disease activity and disability at the start of first treatment during the first 3 years after introducing anti-TNF therapy.13 14
We have reported the costs and health economic benefits associated with early anti-TNF therapy for RA in clinical practice.7 However, we had to use sensitivity analyses for cost-effectiveness estimations, because we did not have multiple measurements during the first treatment year and we also lacked utility values beyond this time. Another aspect not scrutinised in the study was that patients switched between different expensive biological drugs (up to 35% in our setting).14
We undertook the present study on patients with RA, PsA and other spondylarthritides treated in clinical practice in southern Sweden, with four specific goals: (1) To determine if health utilities at the initiation of anti-TNF treatment changed over the 7-year period between May 2002 and December 2008; (2) To address changes in this measure during anti-TNF treatment both in the short and long perspective, including reasons for drug withdrawal; (3) To study if previous biological therapy influenced this measure; (4) To study the feasibility of the preference-based health utility instrument EuroQoL-5 dimensions (EQ-5D) and apply it across different diagnostic entities.
Materials and methods
Anti-TNF treatment courses for patients with RA, PsA and spondylarthritides according to the treating physician were retrieved from the South Swedish Arthritis Treatment Group (SSATG) registry.15 16 17 In 2002, collecting health utility data was introduced in routine clinical follow-up. Data were collected using the five descriptive questions of the EQ-5D.18 The visual analogue scale (VAS) of the EQ-5D was not used. From this generic preference-based instrument, utility values can be derived with a range from death (0) to full health (1), with values below 0 (−0.56) being possible.19 20 The dimensions covered by the EQ-5D include mobility, self-care, usual activities, pain/discomfort and anxiety/depression.
Patients eligible for this study had a diagnosis of RA, PsA or spondylarthritides according to the opinion of the treating physician. Patients with PsA and spondylarthritides were further classified as having peripheral joint disease (arthritis distal of shoulder and hips ever) and/or clinical signs of spondylitis by the treating physician.21 The different diagnoses and classifications have been validated in large groups of patients and found to be accurate in between 90–98%16 21 according to established criteria.22 23 24 The patients were identified in the SSATG registry during the period May 2002 to December 2008 as starting a treatment course of infliximab, etanercept or adalimumab. Treatment courses were classified as either first, second, or third or more anti-TNF. All EQ-5D utility values at treatment follow-up time points 0, 0.5, 1.5, 3, 6, 12, 24, 30, 36, 48 and 60 months were retrieved from the database. Treatment courses lacking baseline EQ-5D were excluded. Anti-TNF treatments were grouped according to the year of initiation for analyses of time trends at treatment onset. The reason for drug withdrawal was documented in the SSATG protocol as failure, adverse event or other, but only one stop reason could be given. Distinction between primary failure (never having a response) and secondary failure (having an initial response, with deterioration later), was not always possible, and they were therefore grouped together. Other stop reasons include among others pregnancy, switching for convenience or remission. Missing follow-up data were requested from treating physicians one to two times per year, including the possible withdrawal reason.
To assess the feasibility of EQ-5D in the current observational setting, the number of follow-up visits with full EQ-5D information was compared with those with data on HAQ.
Statistics
Values are given with mean and 95% CI. Follow-up times are given with median (range) and mean (SD) values. Generally, only observations with at least 20 valid N are presented. Patients remaining on therapy at given follow-up time points were estimated from Kaplan–Meier plots. Patients with full datasets at time 0, 3, 6, 12 and 24 months were compared with all patients to see if there were relevant differences between those with complete and incomplete data.
Results
Baseline patient characteristics according to anti-TNF treatment and diagnosis are shown in table 1. Most patients receiving their second, third or more course of TNF-blocker were included in the first course group, thus making direct statistical comparisons of the patient groups hazardous. There were several differences between the diagnostic groups. RA patients were older, had tried more disease-modifying antirheumatic drugs (DMARD), were more often treated with concomitant DMARD and were more often women. Overall, patients subject to more than one anti-TNF drug tended to be older, have longer disease duration and they were less often treated with concomitant methotrexate. As expected, clinical signs of spondylitis were more prevalent in the spondylarthritides group (77%); many patients belonged to the undifferentiated spondylarthritides entity. Clinical spondylitis was also present in almost 30% of PsA patients.
Baseline characteristics in the different diagnostic and treatment groups
The secular trends for baseline EQ-5D utility values at first anti-TNF treatment and the different diagnoses are illustrated in fig 1. There were weak, non-significant trends for increasing baseline utility values for RA patients (Spearman’s ρ = 0.03, p = 0.23), PsA (ρ = 0.04, p = 0.37) and spondylarthritides (ρ = 0.05, p = 0.29) over time.

EuroQoL-5 dimensions (EQ-5D) at first treatment initiation 2002–8 for rheumatoid arthritis (RA), psoriatic arthritis and spondylarthritides patients.
The development of EQ-5D utilities at first, second and third or more anti-TNF treatment courses for RA, PsA and spondylarthritides patients is illustrated in fig 2. For RA patients, utility improvement during the first and second anti-TNF treatments perform in a similar way. The third or more anti-TNF treatments start from a lower utility level and groups are smaller with wider confidence intervals, but nevertheless they perform with approximately the same numerical improvement as for first and second anti-TNF treatments.

(A) EuroQoL-5 dimensions (EQ-5D) during follow-up for rheumatoid arthritis patients, starting anti-tumour necrosis factor (TNF) treatment 2002–8 and with baseline EQ-5D values. (B) EQ-5D during follow-up for psoriatic arthritis patients, starting anti-TNF treatment 2002–8 and with baseline EQ-5D values. (C) EQ-5D during follow-up for spondylarthritides patients, starting anti-TNF treatment 2002–8 and with baseline EQ-5D values.
Most gain in EQ-5D utilities was already achieved after 2 weeks for both first and second anti-TNF treatments for RA and PsA at the group level, whereas the spondylarthritides patients had a somewhat slower initial improvement.
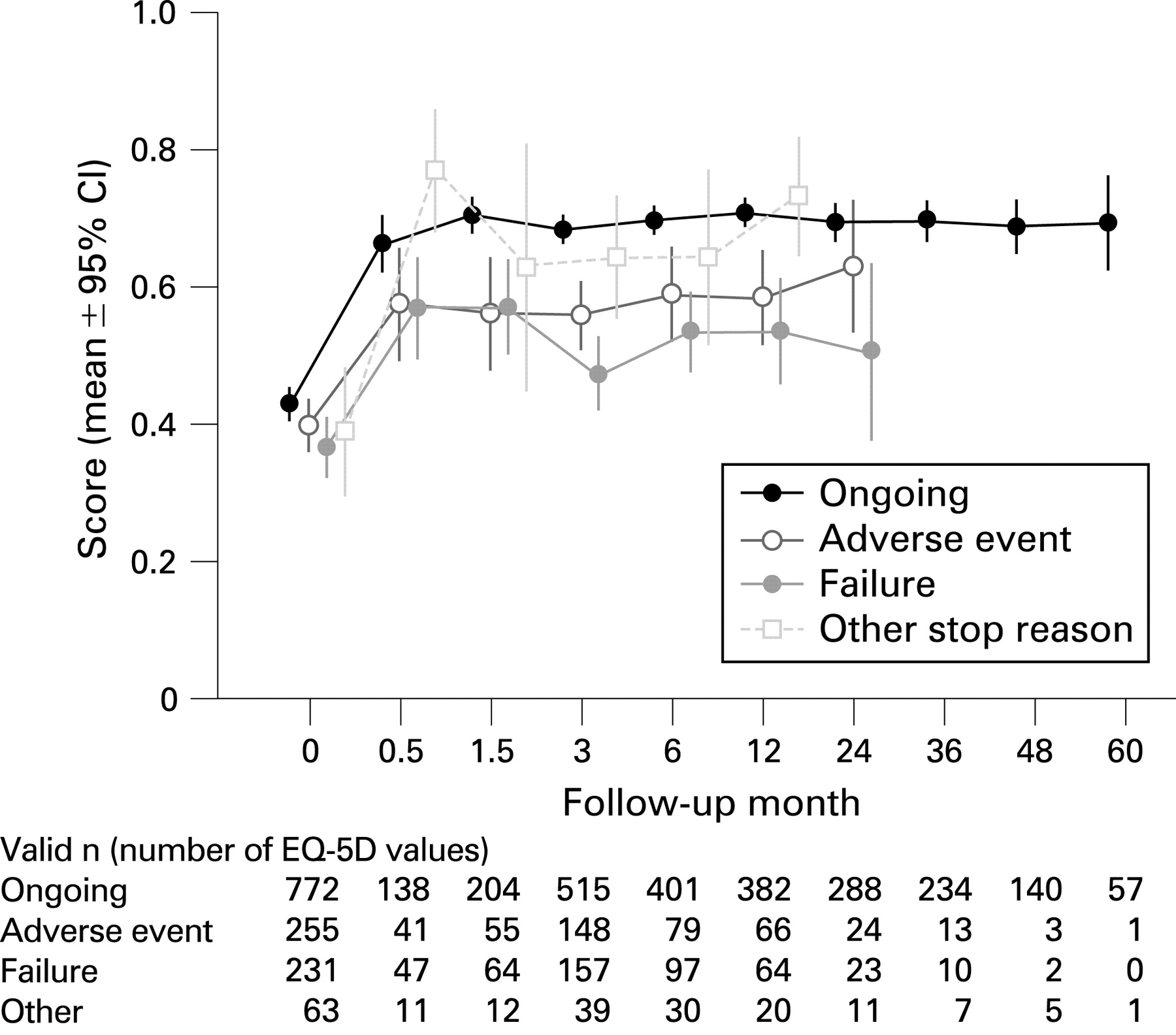
RA patients stopping therapy demonstrated a lower utility gain regardless of the reason for withdrawing treatment (fig 3). Utility improvement in cases with stop reasons other than adverse event or failure seems to perform like those remaining on treatment, but numbers are limited.

EuroQoL-5 dimensions (EQ-5D) during follow-up—stop reason. Rheumatoid arthritis patients starting first anti-tumour necrosis factor treatment 2002–8 and with baseline EQ-5D values.
To assess the feasibility of EQ-5D in clinical practice, we compared the frequency of complete EQ-5D and HAQ questionnaires. The total number of follow-up visits was 12 585, 2553 and 2630 with the presence of HAQ values in 98%, 97%, 97% and the presence of EQ-5D values in 93%, 94% and 94% for RA, PsA and spondylarthritides, respectively.
To investigate the possibility of bias in patients with missing values, we compared the total amount of information for RA patients at time points 0, 3, 6, 12 and 24 months with RA patients with complete datasets at all these time points, grouped according to treatment order (fig 4). The pattern of improvement is similar regardless of dataset completeness, but the magnitude of improvement is somewhat higher at some time points in first anti-TNF courses with complete datasets.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
EuroQoL-5 dimensions during follow-up for rheumatoid arthritis patients. All patients and patients with complete data. TNF, tumour necrosis factor.
To facilitate health economic modelling, we calculated the median/mean follow-up time and life-table estimates of drug survival, in relation to diagnoses, anti-TNF treatment sequences and stop reasons (see supplemental table 1 available online only and fig 2A–C). As expected, patients with ongoing treatment had longer follow-up, whereas those stopping because of adverse events had the shortest. Treatment courses terminated as a result of low response and failure had follow-up times close to those caused by adverse events. Other stop reasons were less common but resulted in longer follow-up times. The overall follow-up time decreased with increasing anti-TNF numbers, and follow-up times were skewed towards early withdrawal as indicated by lower median compared with mean values.
Discussion
A major finding in this study was the rapid improvement in health utilities after only 2 weeks in RA, PsA and spondylarthritides patients treated with their first anti-TNF drug. The improvement was maintained for at least 5 years for patients remaining on therapy. Baseline utilities remained relatively stable during the period 2002–8 for the first anti-TNF drug. This was somewhat unexpected, given our previously reported steady improvement of both disability (HAQ) and disease activity (DAS28; disease activity score in 28 joints) levels during 1999–2006.14 Interestingly, there were no major differences between different chronic arthritis diagnoses, whereas there was a trend towards lower baseline utilities with an increasing number of anti-TNF drugs. However, a limited number of third course anti-TNF in PsA and spondylarthritides patients precludes firm conclusions at present.
EQ-5D was chosen because of its simplicity, patient acceptability and well-established utilities. It is well suited for measuring diseases mainly involving locomotor organs, including dimensions such as pain, mobility, self-care and usual activities, all of which are important in inflammatory joint diseases. We have found the VAS of the EQ-5D less suitable, with low patient acceptability in clinical practice, and the core set already included two VAS scales, one of pain and one of global disease activity. Our findings of only 6–7% missing health utilities compared with 2–3% for HAQ scores confirms the feasibility of the EQ-5D instrument in our observational setting.
EQ-5D is a generic measure thus intended for comparing various diseases. Our findings support this. This type of comparison had not been possible using disease-specific measures such as the HAQ, RA QoL and PsA QoL.9 25 26 Although VAS scales have been used as surrogates in health economic models,27 it should be better to use instruments with established health utilities. However, EQ-5D entails several subjective judgements made by the patients, and therefore it has to be complemented with more objective measures before making decisions regarding the start or change of biological treatment.
Observational data like ours are more generally applicable as a reference for health economic modelling than randomised controlled trial (RCT) data, which are derived from highly selected patients.5 28 29 Furthermore, in Sweden there are no formal requirements for inclusion or response, few economic restrictions, and drug costs are almost entirely funded by society. This may result in more missing data, but data may be less biased towards worse utility and disease activity.
The major strengths of the present study are that the variables have been prospectively collected and the setting can be regarded as truly population based.17 It is also, to our knowledge, the first report giving comprehensive data on the development of EQ-5D utility over 7 years for patients with RA, PsA and spondylarthritides in a clinical setting. Our findings are in line with utility gain in RCT of TNF blockers in RA30 31 and ankylosing spondylitis32 and an observational study of PsA.33
Our investigation also has limitations. First, it is difficult to obtain complete sets of data in the observational setting. Using all available data increases generalisability. This, however, will yield lower improvement estimates compared with including only subjects with complete follow-up information from all visits (fig 4). There may thus be a possible bias if complete datasets are required. Incompleteness could be due to either withdrawal from therapy or missing reports for other reasons. Withdrawal may be the main reason why the gain in health utility is less when using all available data compared with only subjects with complete follow-up information. Those stopping therapy, irrespective of cause (lack of effect or adverse event), had less improvement in health utility before the stop (fig 3). More emphasis should be put on the overall withdrawal rate than on the stop reason, because insufficient effect may lower the threshold for stopping treatment due to a mild adverse event.21 34 Second, regular follow-up is a prerequisite for good data provision. This can be a problem in a voluntary multicentre observational setting such as ours, where health care is provided in organisations changing over time for economic, political or other reasons. Even so, the professional SSATG network has remained stable over the past 10 years, and we have not been able to identify any major bias in the missing follow-up data that would seriously impair our conclusions.
Previously, when we only had baseline and one-year measures, we had to make sensitivity analyses as to when the actual improvement occurred.7 This can now be simplified. In the present dataset, the gain can be regarded as almost instantaneous and steady over the years after anti-TNF institution (fig 2), thereby facilitating the calculation of gain in quality-adjusted life-years. However, it must be kept in mind that these calculations are derived from patients remaining on therapy and therefore selected as good responders. Drug continuation can vary substantially between different treatment remedies in our setting,35 and this must be accounted for in health economic modelling. We consider the data in fig 2 and supplemental table 1 (available online only) fairly robust due to the active and regular search for the treatment withdrawal reason when follow-up data are missing.16 35
Our data illustrate that, irrespective of guidelines, there are trends regarding the baseline characteristics of patients who are started on biological drugs.14 These trends seem less obvious for health utility measures, but long-term follow-up, as in the present study, is needed in addition to analyses of RCT and shorter observational studies to establish the true utility gain in the clinical setting.
In conclusion, this study demonstrates a rapid gain in EQ-5D utility after the initiation of anti-TNF-treatment in chronic arthritis, irrespective of diagnosis, and that this changes little in the subsequent 5 years for patients remaining on therapy. The EQ-5D utility used to describe improvement is feasible in this observational population, and the similar results obtained for various diagnoses support its generic character.
Acknowledgments
The authors are indebted to all colleagues and staff in the South Swedish Arthritis Treatment Group for cooperation and data supply and to Jan-Åke Nilsson for help with statistical calculations.
REFERENCES
Supplementary materials
Web Only Data 69/2/352
Files in this Data Supplement:
Footnotes
▸ Additional supplemental table 1 is published online only at http://ard.bmj.com/content/vol69/issue2
Funding This study was supported by grants from Österlund and Kock Foundations, King Gustav V 80 year fund, Lund University Hospital, Region Skåne, Faculty of Medicine, Lund University and Reumatikerförbundet.
Competing interests None.
Provenance and Peer review Not commissioned; externally peer reviewed.