Article Text

Abstract
Objectives: Anti-citrullinated peptide antibodies (ACPAs) are established as useful predictors of radiographic progression in rheumatoid arthritis (RA). The main objective of this study was to test the prognostic capacity of the recently developed test for anti-mutated citrullinated vimentin (anti-MCV).
Methods: A cohort of 238 patients with RA was followed longitudinally for 10 years; 125 patients with complete x ray sets were included in the main analyses. Radiographs were scored according to the van der Heijde modified Sharp score (SHS). Patients were analysed for anti-MCV and anti-cyclic citrullinated peptide (CCP), and were genotyped for human leukocyte antigen (HLA)-DRB1 “shared epitope” (SE) and protein tyrosine phosphatase, non-receptor type 22 (PTPN22) 1858T.
Results: Anti-MCV and anti-CCP were strongly associated with regard to status and level. Both antibodies were associated with SE, but only anti-MCV was significantly associated with PTPN22 1858T. A positive anti-MCV test increased the odds of radiographic progression by 7.3 (95% confidence interval (CI) 3.2 to 16.5) compared to 5.7 (95% CI 2.6 to 12.5) for a positive anti-CCP. Presence of MCV antibodies gave an average increase in the total SHS of 30 U compared to an average increase of 25 U for the presence of CCP antibodies. Anti-MCVs were more strongly associated to progression in erosions than joint space narrowing. Associations remained after adjustment for other predictors of radiographic progression. The odds of progression increased with increasing anti-MCV level.
Conclusions: Presence of anti-MCV predicted joint damage, and the strength of this prediction was at least as strong as for anti-CCP. Antibody status showed a stronger association to bone than to cartilage destruction. This study also indicates that higher anti-MCV levels add prognostic information compared to their mere presence or absence.
Statistics from Altmetric.com
Rheumatoid arthritis (RA) is a systemic disease characterised by chronic inflammation of the synovium and subsequent cartilage and bone destruction. Reliable prognostic markers are crucial since the progression rate varies considerably between patients and the efficacy of treatment on joint destruction is best early in the disease course.1
The disease mechanisms are considered to be of autoimmune aetiology supported by the strong association to autoantibodies and human leukocyte antigen (HLA)-DRB1 “shared epitope” (SE). The antibody system most specific for RA is directed against citrullinated peptides. Whereas citrullination is associated with inflammation in general;2 the development of anti-citrullinated peptide antibodies (ACPAs) has been shown to be relatively specific for RA.3 Further, the well known RA susceptibility gene HLA-DRB1 is a risk factor for ACPA production rather than for RA in general.4 5 Results from an experimental animal model have suggested that ACPAs may have a direct pathogenetic role in RA.6 ACPAs recognise a variety of citrullinated antigens, including fibrinogen, vimentin and enolase, but not all ACPA-positive sera will recognise all citrullinated antigens.7 8 The presence of ACPAs is established as a useful prognostic marker of joint destruction,9 10 11 12 13 14 15 but the mechanisms for the coupling of antibody status and joint destruction are not known.
ACPAs are commonly measured by anti-cyclic citrullinated peptide 2 (CCP2) assays,16 which use a synthetic mix of citrullinated peptides. The identity of the antigen that initiates RA remains to be found, but vimentin, previously known as the Sa antigen,17 has been proposed as a candidate. Studies have shown that vimentin, secreted by activated macrophages,18 is citrullinated during inflammation and presented via the shared epitope.17 19 To detect antibodies to citrullinated vimentin, an ELISA system that utilises genetically modified citrullinated vimentin (MCV) has recently been developed.20 Anti-MCV has been suggested to be a more sensitive marker of RA than anti-CCP,20 21 22 but the results are conflicting.20 21 22 23 24 25 26 27 Anti-MCV have also been suggested as prognostic marker,21 24 but a recent systematic review reported that a conclusion on the prognostic value of anti-MCV still cannot be drawn.13
The aim of this study was to test the prognostic capacity of antibodies towards MCV. Analyses with anti-CCP are presented as a background reference. We also wanted to address the role of quantitative measures of anti-MCV, and whether cartilage and bone destruction could be equally predicted. Associations between anti-CCP2 and anti-MCV levels and their relations to the key genetic markers HLA-DRB1 (SE) and protein tyrosine phosphatase, non-receptor type 22 (PTPN22) 1858T were also examined.
Methods
Study design and study population
The current analyses were performed in the Norwegian arm of the European Research on Incapacitating Disease and Social Support (EURIDISS) study, which included 238 patients at baseline. Patients and methods have previously been described in detail.15 28 29 All patients had disease of short duration at baseline (maximum 4 years, mean 2.3 years) and fulfilled the American College of Rheumatology (ACR) criteria for RA.30 Clinical, laboratory and radiographic data used in the present study were collected at baseline and at 5-year and 10-year follow-up. The patients were treated according to clinical judgment by their rheumatologist during the study. At baseline (10-year follow-up) 52% (41%) were using disease-modifying antirheumatic drugs (DMARDs), 25% (36%) used prednisolone and 52% (17%) used non-steroidal anti-inflammatory drugs (NSAIDs). In addition, none (12%) of the patients were treated with tumour necrosis factor (TNF)-blocking agents.
Radiographic evaluation
In all, 125 patients with x rays of hands available for scoring at baseline and 10-year follow-up were included in the main analyses. Analyses were also performed in the 136 patients with x rays at baseline and 5 years to prove consistency. The radiographs were scored according to the van der Heijde modified Sharp score (SHS)31 with a maximum score of 280 U (hands only).15 Radiographic progression was defined as a change in SHS of hands >10 U/10 years (hands only). The cut-off is thought to represent real radiographic progression and is used in previous papers from this cohort.15 32 33 As the cut-off is arbitrarily chosen, analyses were also performed by using the median value (>17 U/10 years) as cut-off to prove consistency.
Analyses of antibodies and genotyping
Serum was collected at baseline, 5 and 10 years and stored at −70°C. IgG antibodies to MCV were analysed by ELISA assays (Orgentec, Mainz, Germany) according to the manufacturer’s instructions. Positive cut-off was 20 U/ml. IgG antibodies to cyclic citrullinated peptide (anti-CCP2) was analysed by a second generation ELISA (Inova Diagnostics, San Diego, California, USA) and considered positive above a cut-off value of 25 U/ml. Interassay and intra-assay coefficients of variation (CVs) were <10% and <3% for the anti-CCP and anti-MCV assay, respectively. Genotyping for the PTPN22 1858C>T (rs2476601) polymorphism and HLA-DRB1 was performed by TaqMan allelic discrimination and by sequence-based typing, as previously described.33 SE positivity was defined as carriage of the DRB1 alleles: 0101, 0102, 0401, 0404, 0405, 0408, 1001 and 1402.
Statistical analyses
The analyses were performed using SPSS V. 16 statistics package (SPSS, Chicago, Illinois, USA). Data are presented by means (SD) or by medians (interquartile range (IQR)) according to the distribution of data. Comparisons between groups were performed by Mann–Whitney U test (skewed data) or Student t test (normal distribution) for continuous variables and χ2 tests for comparisons between proportions. Correlations were examined by the Spearman rank correlation test. The area under the curve value (AUC) of anti-MCV was calculated based on measures at baseline, 5 and 10 years. The possible change over time in the ACPA levels were examined by generalised mixed linear modelling. Univariate and multivariate logistic regression analyses were performed to assess predictors of radiographic progression. Associations between the antibodies and the change in SHS were also explored by linear regression. Standard diagnostic tests of model assumptions and residuals were performed. All tests were two-sided and conducted at the 0.05 significance level.
Results
Demographic, clinical and biological characteristics of the cohort
The baseline characteristics of the whole cohort (n = 238) and the 125 patients with complete x ray sets are presented in table 1. Baseline characteristics were similar between the patients with and without radiographic films available. Smoking status was not recorded at baseline, but 71% of the patients were “ever smokers” at 10-year follow-up.
Baseline characteristics of the 238 patients included in the study and the 125 patients with x rays available at baseline and 10 years
Associations of anti-MCV to anti-CCP and genetic status
The presence of anti-MCV (64.3%) was strongly associated to the presence of anti-CCP (60.5%) in the 238 sera measured at baseline (fig 1A). Percentages for the 125 patients with complete data sets were similar (fig 1B). In patients positive for both antibodies, the correlation between anti-CCP level and anti-MCV level at baseline and follow-up (5 and 10 years) was high (Rho = 0.71, 0.79 and 0.84, respectively (p<0.01)).

Association of anti-mutated citrullinated vimentin (MCV) and anti-cyclic citrullinated peptide (CCP) status in all patients at baseline (A) and in the 125 patients with complete data sets (B).
Both anti-MCV and anti-CCP were significantly associated with HLA-DRB1 (odds ratio (OR) 9.0 (95% confidence interval (CI) 4.2 to 19.0) and 8.7 (95% CI 4.1 to 18.5), respectively). Only anti-MCV was significantly associated with PTPN22 1858T (OR 2.3 (95% CI 1.2 to 4.3, p = 0.01, anti-CCP OR 1.5 (95% CI 0.8 to 2.7), p = 0.20). ACPA levels were higher in patients positive versus negative for SE and/or PTPN22 1858T, but these differences did not reach statistical significance when only patients who were ACPA positive were included in the analyses (Supplementary material).
Prediction of radiographic progression
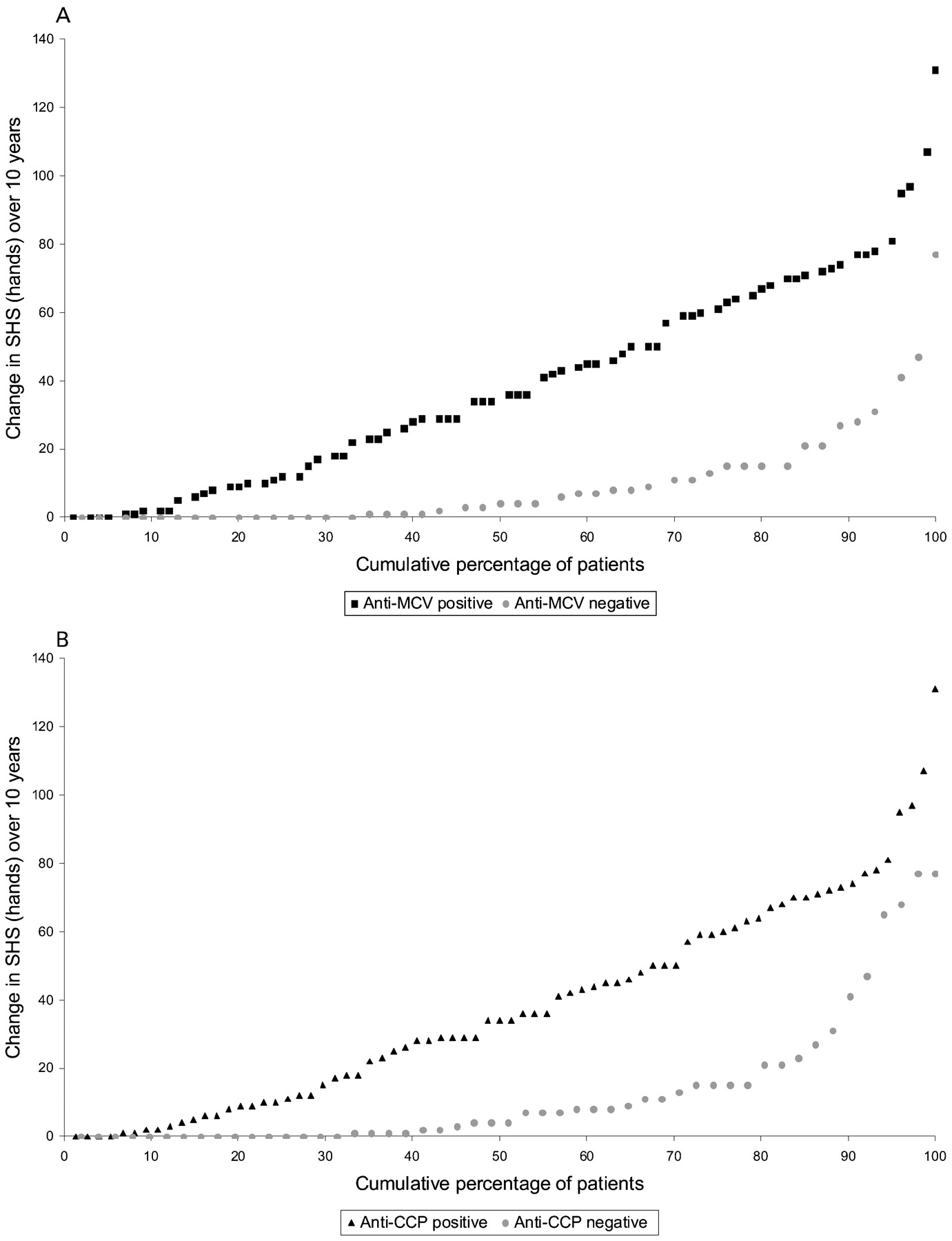
Radiographic progression occurred in 59.2% (n = 74) of the patients with 10-year radiographs available. The median change in the SHS of hands from baseline to 10-year follow-up was 17 (IQR 3 to 47), while median changes in the joint space narrowing and erosion scores were 9 (2 to 26) and 4 (1 to 18), respectively. The percentage of patients with progression was higher in the anti-MCV/anti-CCP positive versus patients who were anti-MCV/anti-CCP negative (77.3%/75.7% versus 31.9%/35.3%, p<0.01). The change in SHS over 10 years according to anti-MCV status (fig 2A) and anti-CCP status (fig 2B) is depicted in cumulative probability plots which show data from each individual patient ranked from the lowest to the highest observed change score within each subgroup.

Change in van der Heijde modified Sharp Score (SHS) of hands from baseline to 10 years according to the anti-mutated citrullinated vimentin (MCV) (A) and anti-cyclic citrullinated peptide (CCP) (B) status.
The presence of anti-MCV showed a slightly higher sensitivity (79.5 (95% CI 68.8 to 87.1) vs 75.7 (95% CI 64.8 to 84.0) of predicting radiographic progression compared to the presence of anti-CCP, with no loss in specificity (anti-MCV 65.3 (95% CI 51.3 to 77.1)/anti-CCP 64.7 (95% CI 51.0 to 76.4)) .The pretest probability of progression in this cohort was 59.2%. The post-test probability with a negative test was 31.9% and 35.3% for anti-MCV and anti-CCP, respectively, and the post-test probability with a positive test 77.3% and 75.6%, respectively.
Regression analyses
Associations between anti-MCV status and radiographic progression were further explored in logistic and linear regression analyses. A positive anti-MCV test (OR 7.3 (95% CI 3.2 to 16.5)) and a positive anti-CCP test (OR 5.7 (95% CI 2.6 to 12.5)) both predicted radiographic progression (table 2). Similar results were found when the median value was used to define radiographic progression (data not shown). In multivariate analyses adjusting for factors previously shown to predict radiographic progression in this cohort (age, gender, rheumatoid factor status, erythrocyte sedimentation rate (ESR), SE and PTPN22 1858T),15 33 the OR for anti-MCV remained significant and numerically higher than for anti-CCP (table 2). The presence of rheumatoid factor (RF), adjusted for the presence of anti-MCV, increased the odds of progression by 2.4 (95% CI 0.9 to 6.4). This indicates an additional contribution of RF to the ACPAs, but the effect was only borderline significant (p = 0.08) as shown in table 2.
The ACPA antibodies as predictors of radiographic progression, results from univariate and multivariate logistic regression analyses
Results from the linear regression analyses are presented in table 3. Presence of MCV antibodies gave an average increase in the total SHS of 30 U, whereas presence of CCP antibodies gave an increase of 25 U (table 3). Anti-MCV status also explained a higher percentage of the change in the SHS (R2 25% versus 18%) (table 3). Both antibodies, as in the logistic regression, predicted radiographic progression independent of other known predictors of radiographic progression, and the numerically stronger association for anti-MCV from the logistic regression analyses was also shown in the multivariate linear regression analyses (table 3). Linear and logistic regression analyses were also performed in the 136 patients at 5-year follow-up with similar results (data not shown). The yearly progression rate was consistent during the whole study period. Similar results were found in subanalyses of patients with disease duration >2 years and <2 years (data not shown).
Associations of the antibodies to change in SHS (total score, erosion score and joint space narrowing score) between baseline and 10-year follow-up
Longitudinal measurements of the antibodies
We did not establish a significant change either in the anti-CCP or in the anti-MCV levels (linear mixed model analyses) over the 10 years, indicating stable levels in individual patients over time (data not shown). Furthermore, the accuracy (logistic regression) or the R2 (linear regression) did not improve if area under the curve values for anti-MCV was used as an independent variable (data not shown).
Separate analyses of change in joint space narrowing (JSN) and erosion scores
The ORs were higher for prediction of progression in erosion score than for progression in JSN score for both antibodies (table 2). This may suggest that ACPAs are stronger predictors of bone than cartilage degradation. Results from the linear regression analyses with change in JSN and erosion score as separate dependent variables supported this observation (table 3). The percentage of the change in the erosion score explained by the presence of ACPAs (R2) was higher than for JSN score (anti-MCV 21% vs 9%, anti-CCP 16% vs 6%) (table 3).
Antibody level
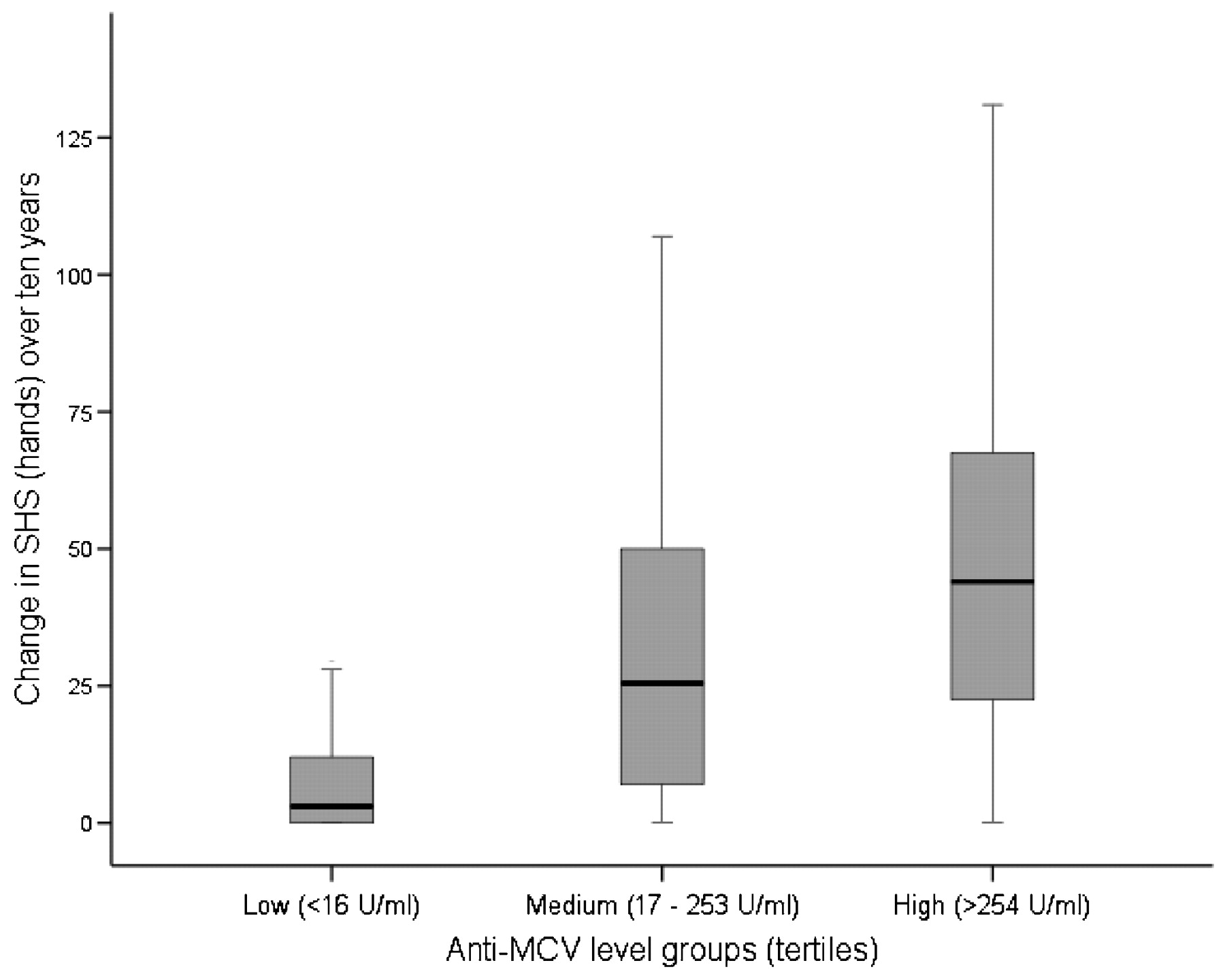
To explore the effect of antibody level, patients were divided into tertiles according to anti-MCV level (lowest tertile 0–17 U/ml, middle tertile 18–253 U/ml and highest tertile >253 U/ml). The median (IQR) changes in SHS over 10 years (3 (0 to 13), 26 (7 to 50) and 44 (22 to 68)) were significantly different (p<0.05) across the groups (fig 3). When these groups were entered as independent variables in logistic regression analyses, the odds of progression increased with increasing anti-MCV level. Patients with moderate levels had an OR of 4.6 (95% CI 1.9 to 11.5) for progression and patients with high levels an OR of 12.7 (95% CI 4.3 to 37.6) compared to patients with levels in the lowest tertile. The same trend appeared when the patients were divided into quartiles the (data not shown).

{kind=link}
{kind=link}
{kind=link}
Change in van der Heijde modified Sharp score (SHS) between baseline and 10 years according to anti-mutated citrullinated vimentin (MCV) level.
Discussion
To make individualised decisions regarding treatment is one of the most important challenges in clinical practise, and identification of sensitive and specific markers of prognosis is an important research question.34 35 36 Patients who are ACPA positive are especially prone to rapid radiographic progression,9 10 11 12 14 15 and early aggressive treatment will particularly slow progression in those patients.37 Less is known of the importance of the subtypes of ACPA related to prognosis. This study shows that the presence of antibodies towards citrullinated vimentin is a strong predictor of radiographic progression, independent of genetic background, RF status and inflammation. A positive anti-MCV test increases the odds of progression by 7 and the average change in the SHS by 30 units (hands only). Compared to the anti-CCP test, anti-MCV numerically showed a stronger prognostic capacity in the logistic and linear regression analyses. This study was, however, not powered to detect a statistically significant difference between the strength of anti-MCV and anti-CCP as prognostic markers, as this would have required 300 patients.
The sensitivity data support that anti-MCV is a valid prognostic marker of radiographic progression, but low specificity of current prognostic markers including ACPAs, is also a limitation with the anti-MCV test.
This study is in line with the reports by Innala et al and Mathsson et al that have previously examined the association between anti-MCV status and radiographic progression in two longitudinal cohorts of patients with RA followed for 2 years.21 24
In this study with a considerably longer follow-up time, radiographs were scored by the van der Heijde modified Sharp score, which enabled us to also investigate joint space narrowing and erosions as separate entities. The association between ACPA status and radiographic progression is well established,9 10 11 12 14 15 but the mechanisms behind this association are not known. It is also not known whether this association exists due to joint degradation in general or to cartilage or bone destruction in particular. This study suggests that especially anti-MCV, but also anti-CCP, was more closely related to bone than to cartilage degradation. Development of bone erosions in RA is mediated primarily by osteoclasts, which are activated by proinflammatory cytokines. A recent study has established that joint space narrowing and erosions occurs at least to some extent as separate processes,38 supporting that ACPAs could have different relationships to these two aspects of joint destruction.
Along the same lines, it is possible to speculate about the nature of the association between high antibody levels and progression. This relationship, previously demonstrated for anti-CCP,15 seems to be related to ACPAs in general and might indicate that the antibodies are directly involved in tissue destruction. ACPAs have been shown to contribute to disease progression by amplifying inflammation and damage in an animal disease model.6 Alternative explanations for a more aggressive disease course in patients with high levels are that high ACPA levels could reflect either a more evolved immunological response or as recently reported from a genome wide association study, a different genetic background.39 Whatever the nature of this association, the demonstration of the association between anti-MCV level and radiographic progression is of clinical importance, as it adds prognostic information. To look at the effect of antibody level, the assay must have an acceptable linearity and precision, which has been shown for the anti-MCV assay (Orgentec) used in the present study.25
We confirmed previous findings of a strong association between CCP and MCV antibodies, regarding status and level.21 22 The question arises whether this association is due to the same epitopes being detected in the two assays. The precise antigenic makeup of the CCP2 kit is not available, and the crossreactivity between CCP2 and MCV is therefore difficult to assess. A recent study has shown that while a high percentage of ACPA-positive sera from patients with RA recognise citrullinated vimentin, sera from ACPA-positive healthy relatives do not.8 This markedly different recognition of citrullinated antigens in health and disease suggests epitope spreading as a possible explanation. Further examination of this question should be performed in cohorts of very early arthritis.
Second generation CCP antigen used in the anti-CCP2 assay is a mixture of cyclic citrullinated synthetically formed peptides, and different from the antigen in the anti-MCV test, showing no known homology to naturally occurring tissue proteins. We found a significant relationship to SE and PTPN22 1858T for anti-MCV, whereas only to SE for anti-CCP. The fact that anti-MCV, unlike anti-CCP, shows a significant association with PTPN22 1858T in the present study could point to a more primary role of anti-MCV in the RA pathogenesis, but could also be due to a higher sensitivity of the anti-MCV rather than a true difference between the antibodies.
The present study has some limitations. Patients were treated according to clinical judgement before inclusion and during the study, but the follow-up was completed before anti-TNF drugs became widely available. However, treatment might be a confounding factor in the relationship between the antibodies and radiographic progression, and detailed data regarding, for example, type of DMARD would have been an advantage. Even though ACPA status was not known to the treating doctors, patients with active, severe disease will be treated more intensively by their doctors and the effect of baseline prognostic markers could be disguised by differences in treatment over time.
Radiographs of feet were not available at baseline and could therefore not be used in the present analyses. This may limit the comparisons of scores to other studies. Possible prognostic markers such as DAS and extra-articular manifestations were not recorded at baseline.
We cannot rule out the possibility that loss of patients can have affected the results. The retention rate among living patients was 73%.28 The patients differed according to disease duration at baseline, but subanalyses showed that the results were similar in patients with short and more established disease. The prognostic value of anti-MCV must also be tested in cohorts of even earlier RA or undifferentiated arthritis. An obvious strength of this study is the long observation period of 10 years and that the scoring method gave the opportunity to examine bone and cartilage involvement as separate dependent variables.
In conclusion, this observational study shows that anti-MCV is a predictor of joint destruction, and that the strength of this prediction is at least as strong as for anti-CCP. Antibody status showed a higher association to bone than to cartilage degradation. This study also indicates that levels and not only presence of anti-MCV should be considered.
Acknowledgments
We thank Inge C Olsen for helpful discussions regarding the statistical analyses.
REFERENCES
Supplementary materials
Web Only Data 69/2/345
Files in this Data Supplement:
Footnotes
▸ Additional data (supplementary table 1) are published online only at http://ard.bmj.com/content/vol69/issue2
Funding This study has been financed with grants from the Eastern Norway Regional Health Authority, the Norwegian Foundation for Health and Rehabilitation and the Norwegian Women Public Health Association.
Competing interests Hans Bijlsma was the Handling Editor for this article.
Ethics approval The regional ethics committee granted approval.
Provenance and Peer review Not commissioned; externally peer reviewed.