Article Text

Abstract
Background: It is known that onset of rheumatoid arthritis (RA) is increased post partum.
Objective: To compare incidence rates between RA and other chronic arthritides (OCA) 0–24 months after delivery, and to compare the incidence rates within each group 0–24 versus 25–48 months post partum.
Methods: Premenopausal women from a Norwegian patient register were linked with the Medical Birth Registry of Norway to study the interval between delivery and time of diagnosis. Cox regression analysis with adjustments for age at delivery and birth order was applied to compare proportions of incident cases of RA and OCA with onset 0–24 months post partum. Poisson regression analysis with adjustment for the population at risk was applied to estimate the incidence rate ratio (IRR) 0–24 versus 25–48 months post partum.
Results: Of 183 RA and 110 patients with OCA diagnosed after delivery, 69 (37.7%) had RA and 31 (28.2%) OCA during the first 24 months post partum (p = 0.09). The IRR (95% CI) for diagnosis during 0–24 months versus 25–48 months was 1.73 (1.11 to 2.70) (p = 0.01) for RA, 1.05 (0.59 to 1.84) (p = 0.86) for OCA. The IRR was 2.23 (1.06 to 4.70) and 1.87 (0.67 to 5.21), respectively, when only considering diagnoses after the first pregnancy. Clinical characteristics were similar within each diagnostic group.
Conclusion: The proportions of incident cases with onset 0–24 months after delivery were not different between RA and OCA. A peak in incidence during 0–24 months was seen in the RA group, both when considering all pregnancies and only the first pregnancy.
Statistics from Altmetric.com
Onset of rheumatoid arthritis (RA) is in several studies found to be rare during pregnancy and more common post partum.1 2 3 However, whether this pattern occurs also in other types of chronic arthritides, including psoriatic arthritis (PsA), ankylosing spondylitis (AS) and unspecified arthritis (UA), has not been extensively studied.
RA is more common in women. In a Norwegian patient register, the female/male ratio under 50 years of age was >4.4 In PsA the female gender ratio is increased in polyarticular disease while oligoarticular and spinal disease is more prevalent in men.5 6 7 PsA may start at all ages,8 9 but in a Finnish study the median age at diagnosis was 46.8 years.10 AS usually starts before 40 years of age with a predominance of male patients,11 12 and the disease onset in women usually occurs during childbearing age.
The increased risk of RA in women during their reproductive years4 13 may partly be explained by hormonal factors. It has been known for a long time that amelioration of RA is often seen during pregnancy,14 15 16 possibly because of increased immune tolerance and shift from Th1 towards Th2 differentiations of T cells, driven by high concentrations of circulating hormones, such as cortisol, oestrogen and progesterone as well as endogenous corticosteroids.16 17 In contrast, there is often a flare in the disease during the postpartum period, which is associated with a sudden fall in hormones after delivery, and a high concentration of prolactin during breastfeeding.18
The hypothesis of this study was that not only RA but also other chronic inflammatory arthritides (OCA) start more frequently after delivery. We could examine this by comparing the proportions of all premenopausal incident RA and OCA cases with diagnosis 0–24 months after delivery, and by comparing the incidence rates 0–24 versus 25–48 months post partum in both RA and OCA.
Patients, materials and methods
Setting
Patients with inflammatory arthropathies have been enrolled into the Norwegian Disease-Modifying Antirheumatic Drug (NOR-DMARD) register since 2001. The patients are included when they start treatment with DMARDs and/or biological treatment, but many of the patients have been diagnosed several years before the inclusion. The NOR-DMARD register has previously been described in detail.19 Medical data on all births in Norway since 1967 have been recorded in the Medical Birth Registry of Norway (MBRN).20 21 Patient data from the NOR-DMARD register in the period 2001–6 were linked with MBRN. Data of female patients aged 18–45 years at the time of inclusion in the NOR-DMARD register and with the diagnosis RA, PsA, AS, UA and juvenile idiopathic arthritis were included in the linkage.
All patients had signed a written informed consent form before enrolment in the NOR-DMARD register. In addition, the eligible women received written information about the planned linkage of NOR-DMARD data with MBRN, and they were given the opportunity to withdraw from the study. Fourteen women withdrew, and data of 632 women from the NOR-DMARD register were linked with the MBRN. The study was approved by the Norwegian Data Inspectorate, the Regional Ethic Committee of Central Norway and the Norwegian Directorate of Health.
Patients
The study population included women with RA, PsA, AS and UA diagnosed after delivery and before 45 years of age. The group with UA comprised patients who started treatment with DMARDs and/or biological treatment without fulfilment of criteria for any specified arthritis. Patients with juvenile idiopathic arthritis were not included in the analyses since they were diagnosed before 16 years of age. All patients were diagnosed by a rheumatologist before or during enrolment in the NOR-DMARD register, and the time of diagnosis was recorded during enrolment.
Assessments
The time interval between the last child delivery before diagnosis and time of diagnosis of RA and OCA (PsA, AS and UA) was identified for each individual patient (data on child delivery from MBRN, time for diagnosis from NOR-DMARD). Since we had registered the time of diagnosis, we chose to examine an interval of 24 months post partum for incident cases since a delay between onset of symptoms and diagnosis is common. Data on birth order and age at delivery were also retrieved from the MBRN register. Birth order was defined as the number of pregnancies including the actual pregnancy. From the NOR-DMARD register we also had data on demographic variables, presence of rheumatoid factor and erosive disease and baseline core measures of disease activity. Disease activity was assessed by swollen joint count and the Disease Activity Score (DAS28) based on 28 tender and swollen joint counts, patient’s global assessment on 100 mm visual analogue scale and the erythrocyte sedimentation rate. Information about erosive disease was based on a routine evaluation of x rays of hands and feet by a radiologist, and erosions were registered as present or absent.
Analyses
Group comparisons were performed with Mann–Whitney U test for continuous variables and χ2 tests for categorical variables. The proportions of incident RA cases and OCA cases with diagnosis 0–24 months after delivery were estimated by Cox multiple regression analyses with adjustments for potential confounding variables as age at delivery and birth order. Kaplan–Meier plots were used to visualise the proportion of patients without disease during the first 5 years after delivery. The curves start at the time of delivery, and time to event is time to diagnosis in years. Poisson regression analysis with adjustments for population at risk was applied to estimate the incidence rate ratio (IRR) of disease 0–24 versus 24–48 months post partum. Data were analysed using the Statistical Package of Social Sciences, version 15.0 (SPSS, Chicago, Illinois, USA) and Statistics/Data Analysis (STATA), version 10.1 (StataCorp, Lakeway Drive College Station, Texas, USA).
Results
Patients
The linkage between NOR-DMARD and MBRN showed that 393 women were parous. Of these, 93 had received a diagnosis of inflammatory arthritides before their first pregnancy, and three patients were diagnosed during pregnancy both in the RA and the OCA group. One patient had missing data for the time of diagnosis. Characteristics of the remaining 293 women (the study population) with disease occurrence after delivery are shown in table 1 (n = 183 women with RA) and table 2 (n = 110 women with OCA). The OCA group consisted of patients with PsA (n = 51), AS (n = 14) and UA (n = 45). The patients with RA had as expected a significantly higher number of swollen joints than for the other diagnosis separately and overall (p<0.001), higher DAS28 score (p = 0.001), were more frequently rheumatoid factor positive (p<0.001) and had more erosive disease (p<0.001). Mean age at diagnosis, mean age at delivery and mean birth order were similar in the patients with RA and those with OCA (tables 1 and 2). Clinical characteristics were similar within each diagnostic group between incident cases after first versus second and additional pregnancies and between incident cases during the first 24 months or subsequent two years after delivery (tables 1 and 2).
Age at diagnosis and at delivery with clinical characteristics of patients who developed RA 0–24 months or 25–48 months after delivery
Age at diagnosis and at delivery with clinical characteristics of patients who developed OCA 0–24 months or 25–48 months after delivery
Occurrence of arthritis post partum
In all, 69 (37.7%) of 183 patients with RA (table 1) and 31 (28.2%) of 110 patients with OCA (table 2) developed arthritis within 2 years post partum versus 27 (14.8%) and 20 (18.2%), respectively, during the next 2 years (tables 1 and 2). Table 3 shows the unadjusted and adjusted relative risks (RR) (95% CI) for being diagnosed during the first 24 months post partum after any pregnancy and after the first and the second and additional pregnancies in RA versus OCA. The relative risks exceeded one, but the risks in RA were not significantly higher than in OCA (table 3).
Relative risk of incident RA versus OCA diagnosed 0–24 months post partum (Cox regression analyses)
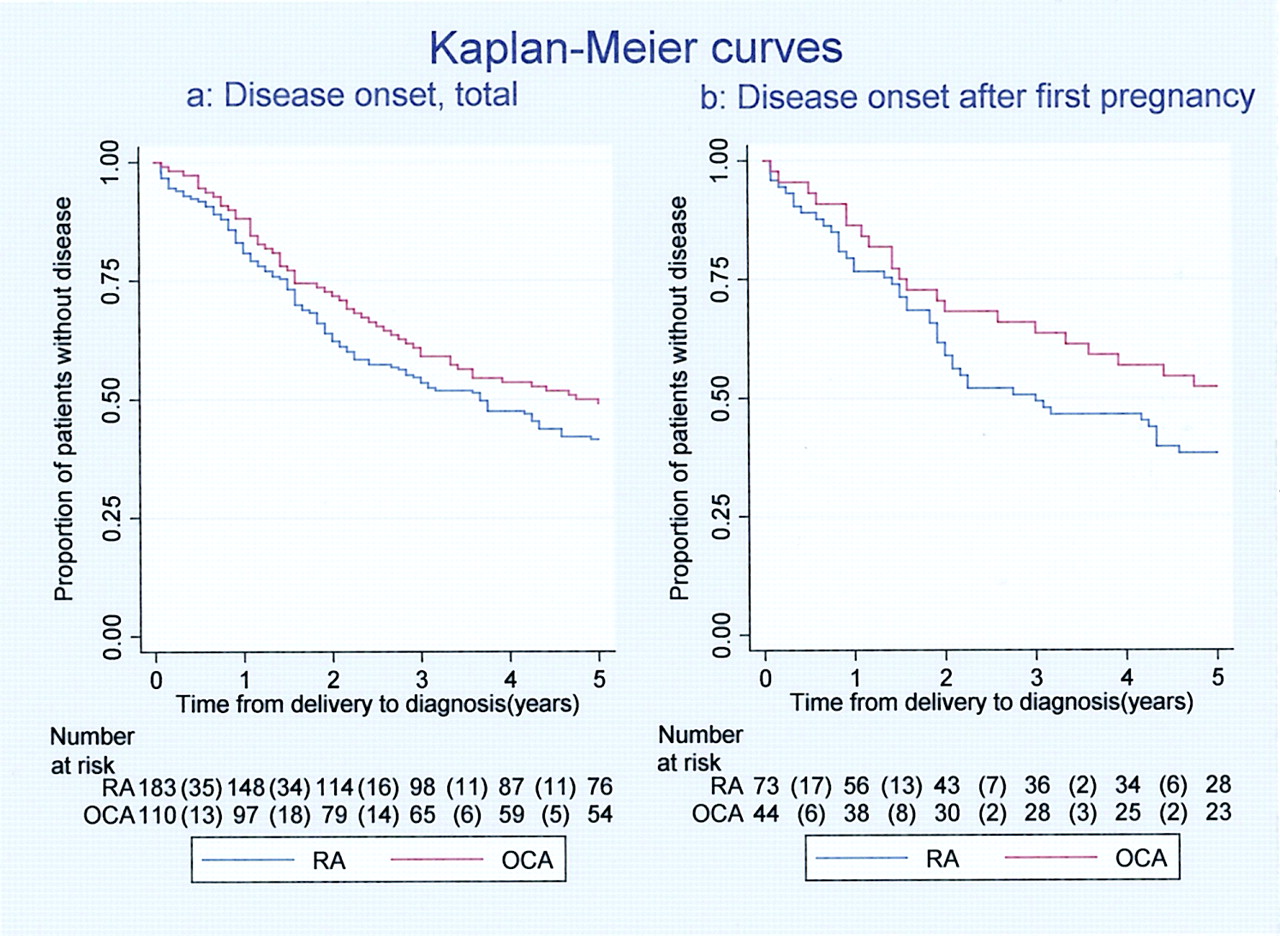
The proportion of patients without disease 0–5 years after delivery is illustrated by Kaplan–Meier curves in fig 1a (total number of disease onset) and fig 1b (disease onset after the first pregnancy). The number of patients at risk each year is also shown in figs 1a and b. Both in the patient group overall (RA + OCA) and in the RA group more incident cases were identified during 0–24 months versus 25–48 months post partum, both after any pregnancy and after the first pregnancy, estimated by a significantly elevated IRR (table 4). In the OCA group IRR was numerically increased for incident cases after the first pregnancy, but the elevation was not statistically significant (table 4).
{kind=link}
Kaplan–Meier curves for patients (RA and OCA) in the NOR-DMARD register without diagnosis 0–5 years post partum; (a) total number of incident cases; (b) incident cases after the first pregnancy. The curves start at the time of delivery, and time to event is time to diagnosis in years. OCA, other chronic arthritides; RA, rheumatoid arthritis.
Relative incidence rate 0–24 months versus 25–48 months post partum by type of arthritis and birth order
Discussion
This study is the first to compare the postpartum onset of RA and OCA. In this registry based case–case study, we found that both RA and OCA were frequently diagnosed during the first 2 years after delivery, and the disease risk was not significantly different between the groups (table 3). We found a higher incidence at 0–24 months versus 25–48 months post partum in the RA group, both for the total number of pregnancies and for diagnosis after the first pregnancy (table 4). The elevation of IRR in the OCA group was not statistically significant, but the group might have been too small with rather wide confidence intervals around the IRR estimate (table 4).
Some previous studies have shown that onset of RA tends to have a peak incidence during the first 12 months post partum,1 2 3 but onset of other arthritides in relation to deliveries has only been examined by a few studies, which have indicated increased onset of PsA22 and AS23 post partum. It is difficult to predict incidence rates of arthritides after delivery, but a prospective Japanese study found that the incidence of RA was 0.08% during the first year after delivery.24 In 1950, a British report concluded that RA occurred less than 1 year after pregnancy in 19%, and in 29% during the first 2 years among all patients with RA under the age of 45.25 Oka found that 12.6% of patients with RA had disease onset within 1 year after delivery.2
Most other studies on incidence of rheumatic diseases after delivery have been analysed according to the time of disease onset (first symptom) rather than time of diagnosis. In these studies, peak onset has been reported within 1 year after delivery. Time of diagnosis will in most patients be later than the time of the first symptom, which may explain why we found an excess of incident cases also in the second year after delivery. If we had included diagnoses only in the first year after delivery, several patients with postpartum onset of disease would have been lost because of the common delay from symptom onset to diagnosis. The diagnoses were always made by a rheumatologist in a clinical setting, which probably reduced the risk of misclassification of patients in our study. However, the patients in the UA group did not fulfil the criteria of any specified arthritis. Some of these patients with UA might later be classified in another group. In the study examining onset of PsA after pregnancy, the patients had polyarthritis, which was partly used as an explanation for why these patients had the same high risk of onset after pregnancy as reported in RA.22 In AS, peripheral arthritis occur in 23–87% of the women.5 In our study, the OCA group most commonly had oligoarthritis, indicating that different types of arthritides may have increased risk of onset after pregnancy.
The current setting represented a unique opportunity to study onset of disease in relation to delivery in both RA and OCA. However, all patients had developed a level of disease which required treatment with DMARDs and/or biological agents, and a potential study limitation is that we were unable to include patients with milder disease who did not require such medication. This possible bias may have contributed to fewer incident cases, especially in the OCA group, since DMARDs usually are more widely used in patients with RA.
We found a higher onset of disease during 0–24 months versus 25–48 months post partum after the first pregnancy, both overall (RA+OCA) and in the RA group (table 4). This indicates a higher risk of developing arthritis after the first pregnancy. A similar trend has been reported in two other studies.3 26 The point estimates of IRR were also numerically higher after the first pregnancy than after the second and additional pregnancies, both for RA and OCA (table 4). However, robust statistical analyses could not be performed owing to insufficient number of patients.
Hazes et al found a lower risk of RA in women who had been pregnant than among women who had never been pregnant.26 Also, the earlier the first pregnancy occurred, the lower the risk of developing RA.26 In the current study, adjustments for birth order and age at delivery in the Cox regression analyses did not significantly influence the relative risks for developing disease 0–24 months post partum (table 3).
A strength of this study was access to clinical data when patients were included in the NOR-DMARD registry. However, we did not observe any associations between disease characteristics and pregnancy order or the time interval from delivery to diagnosis.
It is assumed that hormonal changes due to lactation may influence the timing of RA onset.27 A study limitation was the lack of information about breastfeeding, however, Norwegian women have among the highest rates of breastfeeding in the world up to 1 year post partum.28 29 Further, we had no information about the use of oral contraceptives before pregnancy. Some studies have reported that oral contraceptive use may protect against the development of RA,30 31 but other studies have been unable to confirm this effect.32 33
The tendency for postpartum onset of not only RA but also other types of chronic inflammatory arthritides may be open to various interpretations. First, pregnancy-related hormonal and immunological changes may be shared pathogenic factors influencing the onset of any type of arthritis. Second, adjustment of the immune response to a non-pregnant state after delivery may be a trigger for different autoimmune diseases in susceptible people. Third, the apparently increased onset of RA and OCA post partum may not be a true increased incidence, but a consequence of postponed onset due to the immunosuppressive properties of pregnancy. More research is needed to study these issues in arthritic and other autoimmune diseases.
In summary, the proportion of incident cases with onset 0–24 months after delivery, were not different for RA and OCA. A peak in onset of disease 0–24 months versus 25–48 months post partum was seen overall and in the RA group, both for the total number of pregnancies and for diagnosis after the first pregnancy.
REFERENCES
Footnotes
Funding Research grants for the NOR-DMARD register have been received from Abbott, Amgen, Aventis, BMS, MSD, Roche, Schering-Plough/Centocor, Wyeth and the Norwegian Directorate for Health and Social Affairs. This actual work was supported by the liaison committee between the Central Norway Regional Health Authority (RHA) and the Norwegian University of Science and Technology (NTNU).
Competing interests Hans Bijlsma was the Handling Editor for this article.
Ethics approval Approval from the regional ethic committee of Central Norway.
Provenance and Peer review Not commissioned; externally peer reviewed.