Article Text

Abstract
Objectives: Wegener’s granulomatosis (WG) is a systemic vasculitis characterised by relapsing and remitting disease activity. Immunosuppressive drugs are used to control disease, but increase susceptibility to infection. Therefore, influenza vaccination should be considered in WG patients. This study was performed to assess the immunogenicity of influenza vaccination in WG patients.
Methods: A randomised, controlled trial was performed in WG patients with quiescent disease, defined as a Birmingham vasculitis activity score (BVAS) less than 2. Patients were randomly assigned to receive influenza vaccination (n = 49) or to participate as controls (n = 23). In addition, healthy controls (n = 49) were vaccinated. At entry and at 1 and 3–4 months after entry, antibody responses to vaccination were determined. Furthermore, disease activity was measured (BVAS), adverse effects were recorded and antineutrophil cytoplasmic autoantibody (ANCA) titres were determined.
Results: WG patients achieved high seroprotection rates to all three influenza strains, comparable with healthy controls. Only the A/H1N1 strain patients had a lower seroconversion rate (p = 0.002) and geometric mean titre (p = 0.037) than controls. After 1 month, one control and one vaccinated WG patient had developed active disease. At 3–4 months, two additional control patients had developed active disease compared with none of the vaccinated patients (p = 0.099). Vaccination did not influence ANCA titres. Adverse effects did not differ between patients and healthy controls.
Conclusions: Influenza vaccination in WG patients with quiescent disease induced a sufficient antibody response.
Trial registration number: NTR1130.
Statistics from Altmetric.com
Wegener’s granulomatosis (WG) is a systemic vasculitis characterised by relapsing and remitting disease activity. WG patients are at risk of infections,1 2 partly related to the use of immunosuppressive drugs. Furthermore, the median age of WG patients is relatively high, which increases morbidity and mortality following infection.1
Influenza has a very high yearly incidence and shows considerable morbidity and mortality. Vaccination is the cornerstone for the prevention of influenza. Yearly vaccination reduces the severity of influenza and related complications and is recommended in immunocompromised patients.3 Therefore, influenza vaccination appears to be indicated in WG patients. It is clinically relevant whether WG patients mount protective immune responses. However, there are no studies on the immunogenicity of influenza vaccination, nor any other vaccination, in WG. Both the disease itself and immunosuppressive drugs might hamper the response to vaccination in WG. In systemic lupus erythematosus (SLE), another systemic autoimmune disease, it has been found that the disease itself diminishes the antibody response to influenza vaccination and that azathioprine may further decrease this response.4 5 In solid organ transplant recipients, immunosuppressive drugs also decrease responses to vaccinations.6
In addition, concerns regarding the vaccination-induced activation of established autoimmune diseases have to be taken into account. For SLE, prospective studies did not show an increase in disease activity following influenza vaccination.7 For WG, prospective data are lacking. A retrospective cohort study suggested that influenza vaccination does not lead to an increase in disease activity in WG,8 although there is a case report of a relapse of vasculitis following influenza vaccination.9
Therefore, we performed a prospective, randomised, controlled study to evaluate the immunogenicity of influenza vaccination in WG patients with quiescent disease and to assess a possible influence of influenza vaccination on the risk of relapse.
METHODS
Patients and controls
Patients eligible for the study fulfilled the criteria for WG10 and had quiescent disease, defined as a Birmingham vasculitis activity score (BVAS) of less than 2. Exclusion criteria were a BVAS of 2 or greater, indication for yearly influenza vaccination due to concomitant disease (based on international guidelines),3 the use of prednisone at a dose of more than 30 mg/day and/or cyclophosphamide at more than 100 mg/day, and pregnancy. Patients with active disease were excluded for two reasons; first, the uncertainty regarding vaccination-induced disease activation and, second, expected changes in immunosuppressive medication that might influence the interpretation of the effect of influenza vaccination on disease activity and the analysis of the antibody response to vaccination. Similarly, patients using prednisone at a dose of more than 30 mg/day and/or cyclophosphamide at more than 100 mg/day were considered to have unstable disease and therefore were considered ineligible. Patients were randomly assigned to receive an influenza vaccination or to serve as a patient control, in a ratio of 2 : 1. Randomisation was stratified for influenza vaccination in the previous year and block randomisation with a block length of three consecutive patients was used. A control group of healthy individuals was included; for this purpose, healthcare workers participating in the yearly influenza vaccination campaign were asked to participate. Exclusion criteria for participation as healthy controls were the use of immunosuppressive drugs, malignancy or pregnancy.
Study design
We conducted a prospective, randomised, open, controlled study. WG patients and controls were included from October to December 2005. At entry (visit 1), patients randomly assigned for vaccination and all healthy controls were vaccinated. Patients and controls were seen again after 1 month (visit 2) and 3–4 months (visit 3). During all visits 10 ml blood was drawn, and serum was stored at −20°C until use. At each visit BVAS was recorded for assessing disease activity and antineutrophil cytoplasmic autoantibody (ANCA) titres were measured as described previously.11 A negative titre was recorded as 0. Also, patients were asked to fill in a visual analogue score (VAS) on a scale of 0 to 10 (patient VAS, disease activity as experienced by the patient), 0 indicating no activity and 10 indicating the highest activity. From all participants information on influenza vaccination in the previous year was obtained. Adverse effects to vaccination were recorded using a standardised questionnaire, which included: itching, pain, erythema, induration at the site of vaccination, shivers, myalgia, fever, headache, nausea, arthralgia, diarrhoea and the use of an analgesic/antiphlogistic drug. The study was approved by the institutional medical ethics committee, and informed consent was obtained from all participants.
A single dose of a trivalent subunit influenza vaccine (Influvac, 2005–6, Solvay Pharmaceuticals, Weesp, The Netherlands), containing A/New Caledonia/20/99 (H1N1), A/NewYork/55/2004 (H3N2) and B/Hong Kong/330/2001, was administered intramuscularly.
Antibody response to influenza
For quantitative detection of influenza antibodies the haemagglutination inhibition test was used. Haemagglutination inhibition tests were performed with guinea pig erythrocytes following standard procedures12 with slight modifications as described elsewhere.13 Sera were tested for antibodies to all three vaccine strains. The antibody response was evaluated by serological parameters and criteria as defined by the European Agency for the Evaluation of Medicinal Products (EMEA).14 Serological parameters were seroprotection rates, seroconversion rates and mean geometric increases.
The seroprotection rate is the percentage of vaccinees with titres of 40 or greater, a titre that can be considered protective in healthy adults.15 Seroconversion corresponds to a negative prevaccination titre (<10) converting to a titre of 40 or greater 1 month postvaccination (original definition of seroconversion) or a significant increase in antibody titre, ie, at least a fourfold increase in titre. Mean geometric increases correspond to the fold increase in geometric mean titres (GMT) within a study population 1 month after vaccination. Titres less than 10 (below the detection level) are assigned a value of 5 for calculation purposes.14
Statistical analysis
Data were analysed using SPSS 14. Titres were log-transformed before testing of geometric mean titres. For testing differences in age between groups Student’s t-test was used. For prednisone use, azathioprine use and geometric mean titres the Mann–Whitney U-test was used. For all other variables the χ2 test or Fisher’s exact test were used, depending on the size of the expected counts. A p value less than 0.05 was considered statistically significant. Power analysis was based on differences in antibody response. We hypothesised that the seroprotection rate in healthy controls would be 80% per strain.14 A 20% lower seroprotection rate in WG patients was considered clinically relevant. To give the study a power of 80% at an alpha of 5% to demonstrate such a difference if it should exist (one-sided testing), 54 WG patients and 54 healthy controls had to be vaccinated.
RESULTS
Patient characteristics
Seventy-three WG patients gave informed consent to participate. One patient initially randomly assigned to the control group developed active disease before the start of the study and was excluded. Seventy-two patients started and completed the study. Thirty-seven were men (51%), the mean age was 59 years (SD 14). Forty-nine patients were vaccinated, 23 served as patient controls (table 1). Patient groups did not differ in sex and age. All patients who started the study had a BVAS of 0 at entry, except for one patient in the patient control group with a BVAS of 1 (arthralgia).
Antibody responses
Sixty-five per cent of vaccinated WG patients had received an influenza vaccination in the previous year, compared with 8% of healthy controls (p = 0.000). Accordingly, WG patients had higher prevaccination GMT, although these were far below the protective level of 40 (table 2). Vaccination resulted in similar seroprotection rates in patients and healthy controls for all vaccine strains, 1 and 3–4 months after vaccination (fig 1A). Seroconversion rates for strains A/H3N2 and B were similar in patients and healthy controls. For strain A/H1N1, however, the seroconversion rate was lower in patients (fig 1B). Also, WG patients had similar postvaccination GMT to strains A/H3N2 and B as healthy controls but a lower postvaccination GMT to strain A/H1N1 (table 2).
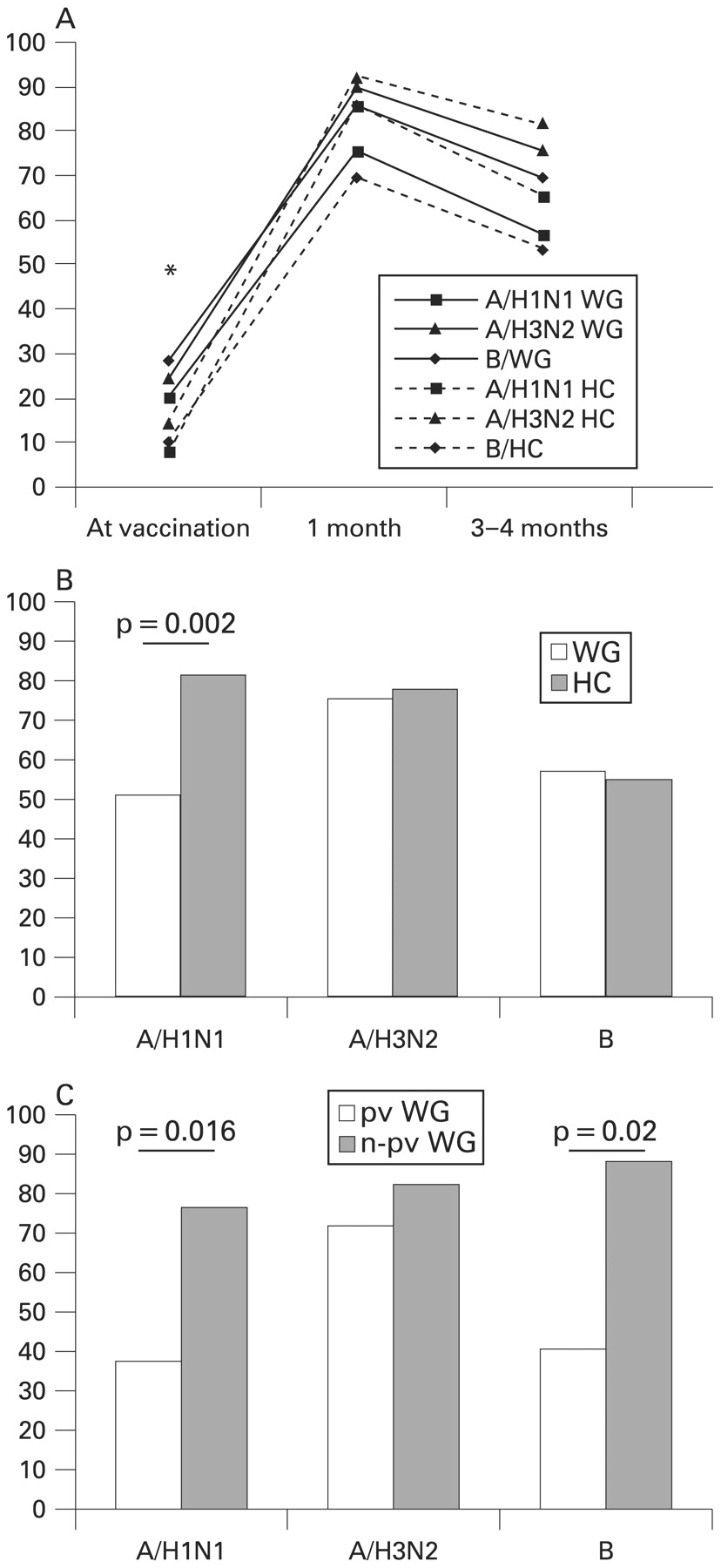
Antibody responses. Seroprotection (A) and seroconversion (B) rates to the vaccine strains in patients with Wegener’s granulomatosis (WG) and healthy controls (HC). In (C) seroconversion rates in WG patients who received influenza vaccination in the previous year (previously vaccinated; pv WG) are compared with WG patients who did not receive an influenza vaccination in the previous year (not previously vaccinated; n-pv WG). The seroprotection rate is the percentage of vaccinees with titres of 40 or greater. The seroconversion rate is the percentage of vaccinees with seroconversions. Seroconversion corresponds to a negative (<10) prevaccination titre converting to 40 or more 1 month postvaccination or a significant increase in the antibody titre, ie, at least a fourfold increase in titre. *p = 0.039 for the B strain; before vaccination the seroprotection rate to the B strain was higher in WG patients compared with healthy controls.
Patients vaccinated in the previous year were older than patients not vaccinated in the previous year (mean 60 years vs 52 years, p = 0.033), but did not differ in the use of immunosuppressives (table 2). Prevaccination GMT were higher in previously vaccinated patients; however, postvaccination GMT were lower in previously vaccinated patients (table 2); for A/H1N1 this difference was significant. Seroconversion rates were lower in previously vaccinated patients for strains A/H1N1 and B (fig 1C). No differences were observed in the seroprotection rates achieved (data not shown).
The possible effects of immunosuppressive drugs on the antibody response to vaccination were evaluated. Vaccinated WG patients using immunosuppressive drugs (n = 25) were compared with WG patients not using immunosuppressives (n = 24). Groups were comparable with respect to sex (p = 0.156), age (p = 0.787) and vaccinations in the previous year (p = 0.538). No differences were found in seroprotection rates, seroconversion rates (fig 2) and GMT (data not shown). The use of prednisone or azathioprine, studied separately, was of no influence on the antibody response (data not shown).

{kind=link}
{kind=link}
Influence of the use of immunosuppressive drugs (IS) on seroprotection and seroconversion rates in Wegener’s granulomatosis (WG) patients. Seroprotection (A) and seroconversion (B) rates to the vaccine strains in patients with WG who used immunosuppressive drugs versus patients who did not. The seroprotection rate is the percentage of vaccinees with titres of 40 or greater. The seroconversion rate is the percentage of vaccinees with seroconversions. Seroconversion corresponds to a negative (<10) prevaccination titre converting to 40 or greater 1 month postvaccination or a significant increase in antibody titre, ie, at least a fourfold increase in titre.
Two possibly confounding factors were differences in age and previous influenza vaccinations. Multivariate analysis of these factors could not be performed, due to the low number of healthy controls who received an influenza vaccination in the previous year (n = 4) and the absence of healthy controls older than 63 years. Therefore, subanalyses were performed to assess the influence of these factors. First, participants were matched for age. In this subanalysis 37 WG patients and 37 healthy controls were included. Antibody responses were similar as in the whole group analysis. Here too, a trend towards a lower response to the A/H1N1 strain was observed in WG patients, although this did not reach significance (data not shown). Next, patients (n = 17) and controls (n = 45) who were not vaccinated the previous year were compared. WG patients showed antibody responses comparable to controls, also for the A/H1N1 strain (data not shown).
Safety parameters
Adverse effects to vaccination in vaccinated WG patients and healthy controls (table 3) were comparable. Next, the effects of influenza vaccination on disease activity in WG patients were evaluated. During the first month following entry, one non-vaccinated and one vaccinated WG patient developed active disease. Both patients reached complete remission after treatment with prednisone and cyclophosphamide. Two additional non-vaccinated patients developed active disease in the period up to 4 months after entry, compared with none of the vaccinated patients (p = 0.099). At entry and during follow-up, vaccinated and non-vaccinated patients did not differ in ANCA titres, fourfold increases in the ANCA titre and patient VAS scores (table 4).
DISCUSSION
To our knowledge, this is the first controlled study to evaluate the immunogenicity of influenza vaccination in WG patients. In addition, we included a non-vaccinated patient group to get an indication of the possible effects of influenza vaccination on WG disease activity, as vaccination-induced relapses are a concern and prospective studies of vaccinations in WG are lacking. Randomisation was considered obligatory, to prevent a bias in patient groups. Because of the possible disadvantageous effects of randomisation for the non-vaccinated, patients with an indication for yearly influenza vaccination due to concomitant disease were excluded.
Antibody responses to influenza vaccination in WG patients and healthy controls were similar. First, vaccination induced high seroprotection rates in WG patients, comparable to healthy controls, which is of clinical importance. Also, seroconversion rates, which define adequate responders to vaccination, did not differ between patients and healthy controls, except for the A/H1N1 strain. Finally, results for GMT, used to compare the magnitude of the response between groups, were analogous to those for seroconversion rates. Importantly, seroprotection rates and GMT to strains A/H3N2 and B were comparable between patients and healthy controls for a period of 3–4 months. This indicates that clinical protection from influenza infection may have been achieved for at least the larger part of the influenza season. Furthermore, influenza vaccination in WG patients fulfilled EMEA serological criteria on influenza vaccine immunogenicity. In adults (18–60 years), for each strain at least one of the following criteria should be met: a seroconversion rate greater than 40%; mean geometric increase greater than 2.5; seroprotection rate greater than 70%. In individuals over 60 years, the criteria are greater than 30%, greater than 2.0 and greater than 60%, respectively.14
In transplant recipients, several immunosuppressive drugs have been shown to hamper antibody responses to vaccination.16–18 In the present study, no effects of immunosuppressive drugs on the antibody response were found. However, the number of WG patients receiving immunosuppressive drugs was low and drug use was heterogeneous. Therefore, the conclusion that in WG patients immunosuppressive drugs have no effect on the immune response to vaccination should be made with caution and is limited to the low doses of azathioprine and prednisone given in this study.
The immunogenicity of (influenza) vaccination in autoimmune diseases has been a subject of discussion, as it can be hypothesised that a dysregulated immune system is not able to mount normal responses to vaccination. In SLE, this seems to be the case,7 for WG these are the first data. As antibody responses were similar in WG patients and healthy controls, despite the use of immunosuppressives by half of the patients, WG patients appear to have a normal capacity to respond to vaccine stimuli. The difference between SLE and WG may be due to a generalised immune disturbance in SLE, compared with a restricted immune dysfunction in WG. This may be expected, as SLE is characterised by numerous autoimmune features, exemplified by the generation of a broad spectrum of autoantibodies,19 whereas dysregulation in WG appears to be more specific, involving ANCA to proteinase-3 and myeloperoxidase.20
The effect of repeated influenza vaccinations on the antibody response to vaccination was analysed in WG patients as this may be relevant in patient care. There has been considerable discussion as to whether annually repeated influenza vaccinations influence antibody responses to vaccination. Several studies reported decreased humoral responses in the case of repeated vaccinations with inactivated influenza vaccines.21–23 We also observed a trend towards lower postvaccination GMT in previously vaccinated WG patients, reaching significance for the A/H1N1 strain (same vaccine strain since 2000–1). Seroconversion rates were also lower, except for A/H3N2, which was the only new strain in the vaccine. However, others found similar24–26 or improved27 responses following repeated influenza vaccinations. Smith et al28 used mathematical modelling to explain apparently conflicting results, suggesting that vaccines that are antigenically close to a previous vaccine may be partly eliminated by pre-existent crossreactive antibodies, thus reducing the immune response. In line with this suggestion, it has been reported recently that repeated vaccinations with an identical influenza strain in consecutive years lead to lower titres compared with vaccination in a naive individual, unrelated to the prevaccination titre.29
Regarding the risk of relapse, four patients developed active disease over a period of 3.5 months, equivalent to an annual incidence of 19%, which is in accordance with the expected number of relapses.30–32 Influenza vaccination in WG patients with quiescent disease did not influence the occurrence of relapses and did not increase ANCA titres or patient VAS scores. ANCA titres reflect disease activity to some extent, although there are controversial data.33 34 However, data on the risk of relapse following vaccination need to be interpreted with caution, as the study was not designed to detect such an effect and was considerably underpowered in this respect. Furthermore, our findings are restricted to the use of a trivalent subunit vaccine for intramuscular use. Of note is the fact that the live attenuated intranasal vaccine available in some countries is contraindicated in immunosuppressed hosts.
Although our findings seem plausible, this study has some limitations. First, the study was powered to detect a clinically relevant difference in antibody response between WG patients and healthy controls. However, the number of patients and controls included was lower than required. In our opinion this will not be of major influence on the conclusions. Apart from the A/H1N1 strain, no tendency was observed towards a lower response in WG patients, making it unlikely that a significant difference with healthy controls would have been observed if five more patients and controls had been included. Second, WG patients were older and had received an influenza vaccination in the previous year more often than healthy controls. Both factors may affect immune responses. Previous vaccination status may limit seroconversion rates to a newly administered vaccine, as may have been the case for A/H1N1 in this study. To assess whether differences in age and previous vaccination status were of influence, subanalyses were performed. When WG patients and healthy controls were matched for age, no differences were found in seroprotection rates, seroconversion rates and GMT achieved, although a trend towards a decreased response to the A/H1N1 strain was observed in WG patients. Concerning previous vaccination status, WG patients and healthy controls who did not receive an influenza vaccination in the previous year showed similar antibody responses for all strains. From these subanalyses it appeared that age had a minor influence, and previous vaccination status a more profound influence, at least for the antibody response to the A/H1N1 strain. Third, BVAS and VAS may have been influenced to some extent by a lack of blinding in this study; however, BVAS criteria are fairly objective.
In conclusion, we show that in WG patients with quiescent disease, subunit influenza vaccine resulted in adequate antibody responses, despite older age and the use of immunosuppressive drugs and did not appear to increase the risk of disease relapse. WG patients constitute a population in which influenza vaccination seems to be indicated. Although questions regarding serological responses to repeated vaccinations may remain, annual vaccination can be considered clinically effective.35 36 Therefore, annual influenza vaccination may be recommended in WG patients with quiescent disease.
REFERENCES
Footnotes
Competing interests: None.
Funding: Grant support was received from the Jan Kornelis de Cock Foundation, The Netherlands and Solvay Pharmaceuticals, Weesp, The Netherlands.
Ethics approval: The study was approved by the institutional medical ethics committee.
Patient consent: Obtained.
Linked Articles
- Letter