Article Text

Abstract
Aim: To study the relationship between disease activity, radiographic damage and physical function in patients with ankylosing spondylitis (AS)
Patients and methods: Baseline and 2-year data of the Outcome in Ankylosing Spondylitis International Study (OASIS)(217 patients) were used. Physical function was expressed by the Bath Ankylosing Spondylitis Functional Index (BASFI) and the Dougados Functional Index (DFI); disease activity by the Bath Ankylosing Spondylitis Disease Activity Index (BASDAI) and by erythrocyte sedimentation rate and C-reactive protein; and structural damage by the modified Stoke Ankylosing Spondylitis Spine Score (mSASSS). Syndesmophyte- and non-syndesmophyte sum cores, and numbers of affected (bridged) vertebral units were derived from the mSASSS. Univariate correlations were calculated on baseline values using the Spearman rank correlation. Multivariate associations were investigated by generalised estimating equations (GEE) on baseline and 2-year data.
Results: mSASSS correlated moderately well with BASFI (Spearman’s r = 0.45) and DFI (r = 0.38). BASDAI correlated well with BASFI (r = 0.66) and DFI (r = 0.59). Correlation coefficients for mSASSS versus BASFI and DFI decreased by increasing levels of BASDAI, being zero at the highest quintile of BASDAI. GEE showed that both BASDAI and mSASSS independently and significantly helped to explain either BASFI or DFI. Results were similar for syndesmophyte sum score, non-syndesmophyte sum score, number of affected VUs or number of VUs with bridging. The lumbar part of the mSASSS contributed similarly to the cervical part in explaining BASFI/DFI.
Conclusion: Physical function impairment in AS is independently caused by patient-reported disease activity and the level of structural damage of the lumbar and cervical spine. Syndesmophytes and other radiographic abnormalities contribute to physical function impairment.
Statistics from Altmetric.com
One of the major outcomes in chronic rheumatological diseases is physical functioning. One of the major goals of treatment is to improve physical function and to maintain an acceptable state. Instruments to measure physical function have been developed for most chronic inflammatory diseases. Well-known examples of such instruments are the Health Assessment Questionnaire (HAQ) for rheumatoid arthritis (RA) and the Bath Ankylosing Spondylitis Functional Index (BASFI) for ankylosing spondylitis (AS). In the absence of true “gold standards”, these instruments are patient reported, implying that they are sensitive to subjective interpretation. Although the validity of these patient-reported instruments measuring true physical function is not beyond argumentation, they are used world wide, are accepted by regulatory authorities for drug registration and serve with some authority as outcome measures in cost-effectiveness analysis.
Physical function impairment can theoretically be subdivided into a reversible and an irreversible component.1 In this concept is the reversible component due to signs and symptoms that are experienced by the patient and prevent him from optimal daily functioning. Examples are pain and stiffness due to inflammation (disease activity). Expectedly, reversible function loss is sensitive to intentional (eg, by treatment) or unintentional fluctuations in disease activity. The irreversible component of physical function impairment is due to fundamental changes in the structure of the organism (or structural damage) that have occurred as a consequence of the disease, such as joint erosions and tendon rupture in RA and syndesmophytes and vertebral bridging in AS. These changes are permanent and not subject to fluctuations in disease activity.
The relationship between physical function, disease activity and structural damage in RA has been thoroughly investigated, and there is broad consensus that physical function, as assessed by the patient using the HAQ, is determined both by disease activity and structural damage.2–4 Importantly, disease activity itself is the major driver of structural damage, since inflammation causes joint destruction.5 The relationship between physical function, disease activity and structural damage in AS is much more complicated, primarily because there is accumulating evidence from clinical trials that—unlike the situation in RA—disease activity is not an important driver of syndesmophyte formation or other abnormalities.6 7
Theoretically, extensive structural damage in AS (bamboo spine) should interfere with physical functioning, because structural damage impairs spinal mobility,8 but it is known that patients with AS can cope very well with limitations,9 10 and moderately severe damage of the spine may not necessarily translate into measurable functional impairment.
In this study we have investigated the relationship between disease activity, structural damage and physical functioning in detail, testing the hypothesis that the level of structural damage independently contributes to physical function impairment. This relationship is relevant in view of the recent observations in clinical trials with tumour necrosis factor (TNF)-blocking drugs, which have produced excellent improvement of signs and symptoms of AS, as well as of physical function, but no effect at all on progression of structural damage.6 7 If structural damage co-determines long-term outcome in AS, specific treatments should be found to modify this outcome.
PATIENTS AND METHODS
For this analysis use was made of the Outcome in Ankylosing Spondylitis International Study (OASIS), an international initiative that started in 1996 and has included 217 consecutive patients with AS, without further eligibility criteria, who were followed up for several years.11 Patients were regularly attending the outpatient clinics of the departments of rheumatology of the hospitals in Maastricht (university hospital) and Sittard (general hospital), the Netherlands; Gent, Belgium (university hospital) and Paris, France (university hospital). Importantly, patients were treated according to standard care in 1996, implying that they used non-steroidal anti-inflammatory drugs if considered necessary (either on demand or continuously), analgesics if necessary, disease modifying antirheumatic drugs according to preference of the treating doctor and physiotherapy. None of the patients in OASIS had used TNF-blocking drugs during the period analysed in this study.
Patients were assessed regularly by questionnaires, clinimetry, laboratory assessments and radiography of pelvis and cervical and lumbar spine. For this analysis use was made of the baseline and the 2-year assessment. One-year radiographic data were omitted because of the very low level of variation in 1-year radiographic progression. Variables that were used included the BASFI12 and the Dougados Functional Index (DFI)13 for assessing physical function. Both indices are questionnaires that are completed by the patient and include 10 (BASFI) or 20 (DFI) questions about relevant components of physical function in daily life. BASFI is completed on a visual analogue scale, ranging from 0 (best) to 10 (worst). The BASFI score is the unweighted mean of the 10 questions. The DFI is completed on a five-point Likert scale with steps of 0.5 ranging from 0 (best) to 2 (worst). The DFI is the sum of all questions (range 0–40). Patients completed the validated versions for their own language. The Bath Anklyosing Spondylitis Disease Activity Index (BASDAI)14 was used to measure patient-reported disease activity. The BASDAI includes six questions related to particular signs of their disease (back pain, fatigue, pain in joints and entheses, stiffness severity and duration) and is completed by the patient on a 10 cm visual analogue scale. As additional measures of disease activity, erythrocyte sedimentation rate (ESR) and C-reactive protein were used since it is known that the association between acute phase response and the BASDAI is poor, thus providing information on other aspects of disease activity in addition to the patient-reported level of disease activity.
To measure AS-related structural damage, the modified Stoke Ankylosing Spondylitis Spine Score (mSASSS) was used.15 16 The mSASSS was recently chosen by the Assessment in AS international Society (ASAS) and the international Outcome Measurement in Rheumatoid Arthritis Clinical Trials (OMERACT) as the preferred measure for measuring structural damage and progression in AS.17 The mSASSS assesses anterior changes of the vertebrae of the cervical and lumbar spine on a scale ranging from 0 to 3 at 24 levels. The mSASSS ranges from 0 (completely normal) to 72 (complete bridging). It includes squaring, erosions, sclerosis (all score 1), syndesmophyte formation (score 2) and bridging (score 3). To investigate the relative importance of syndesmophytes, four additional scores were derived from the mSASSS, three focusing on syndesmophytes and one focusing on erosions, sclerosis and/or squaring:
a syndesmophyte sum score, which is the sum of scores ⩾2;
the number of vertebral units (VUs) (maximum 12) affected by syndesmophytes. A VU is defined as a unit delineated by the lower half of the upper vertebra, the upper half of the adjacent lower vertebra, and the intervertebral disc. Thus, 12 VUs contribute to mSASSS;
the number of VUs with complete bridging by syndesmophytes;
a non-syndesmophyte sum score, which is the sum of scores = 1.
All derived scores were determined for the lumbar, cervical and lumbar plus cervical spine separately.
For analysis and visualisation we divided the patients into groups: all patients without damage, and the remaining patients with damage in tertiles, resulting in the following categories based on mSASSS: 0, 1–6, 7–36 and 37–72.
Statistical analysis
Simple univariate correlation coefficients (Spearman rank correlation) were calculated using baseline data only. Independent associations between the variables of interest were investigated by generalised estimating equations (GEE). GEE is a regression technique that allows the investigation of longitudinal data while adjusting for within-patient correlation. GEE requires a predefined working correlation structure for the dependent variable (BASFI or DFI) and based on the baseline and 2-year data, an exchangeable correlation structure was chosen here. GEE is relatively robust against violation of multivariate normality, so that variables were not transformed before entry. The main explanatory variables BASDAI and mSASSS or subscores were used as continuous variables or as categorical variables upon categorisation. Since patient-reported outcomes are age and sex dependent, interactions of age and sex with BASDAI or with mSASSS with respect to explaining BASFI (DFI) were investigated first. Other covariates in the analysis were disease duration, defined as the onset of complaints, HLA-B27 status and hip involvement. Results were expressed as regression coefficients and estimated marginal means (an estimated marginal mean is the model estimator of the mean value of the dependent variable after adjustment for the covariates).
Subsequently, the importance of syndesmophytes as well as of sclerosis, squaring and erosions in explaining variation in BASFI and DFI by splitting mSASSS into a syndesmophyte sum score and a non-syndesmophyte sum score (the latter including scores for sclerosis, squaring and erosions) was examined. Separately, sum scores for the number of VUs with syndesmophytes, and for the number of VUs with bridging were developed. These sum scores were compared by goodness-of-fit statistics (Quasi Likelihood under Independence Model Criterion (QIC), which is an extension of Akaike’s Information Criterion). Goodness-of-fit statistics give an impression of the way in which the model fits the data (R2 in simple regression analysis). The lower the QIC, the better the model fits the data.
RESULTS
Table 1 presents the key baseline characteristics of the OASIS cohort.
It is obvious that the dataset includes the entire range of possible values that a variable can take. Expectedly, BASFI and DFI correlated well (Spearman correlation coefficient 0.88). The correlation coefficients were 0.45 for mSASSS and BASFI, and 0.38 for mSASSS and DFI, suggesting moderate correlation. The correlation coefficient was 0.66 for the relation between BASDAI and BASFI, and 0.59 for the relation between BASDAI and DFI, suggesting a moderate to good association.
Interestingly, the correlation between mSASSS and BASFI or DFI was modified by the level of BASDAI (table 2).
Using baseline data only, the correlation between mSASSS and both measures of function was highest in the lowest stratum of BASDAI and decreased for each increasing stratum of BASDAI, being completely absent at the highest stratum of BASDAI. This phenomenon strongly suggests a ceiling effect of BASFI and DFI: because of the high level of correlation between BASDAI and BASFI/DFI, a correlation between mSASSS and BASFI/DFI can no longer be demonstrated at high levels of BASDAI.
To further investigate the relationship between mSASSS and BASFI/DFI while adjusting for BASDAI and other potential confounders, multivariate analysis was performed using GEE with BASFI or DFI as dependent variables and mSASSS and BASDAI as covariates, while adjusting for age, sex, disease duration, HLA-B27 status and hip involvement. This analysis was performed on a limited dataset including only cases with a BASDAI ⩽6 (188 patients with one or two time points, resulting in 303 cases), in order to overcome spurious results caused by a ceiling effect, but with data obtained at baseline and 2 years while adjusting for within-patient correlation. Table 3 shows the results of this analysis.
Both BASDAI and mSASSS independently contributed to explaining BASFI or DFI with highly significant parameter estimates. The regression coefficients describe the independent relationship between the explanatory variable (eg, mSASSS) and the dependent variable (eg, BASFI): on average, as compared with a patient with a mSASSS of 40 units, a patient with a mSASSS of 50 units has a BASFI that is 0.57 (10 times 0.057) higher, independent of the BASDAI. ESR was weakly contributory, though the correlation between BASDAI and ESR was weak (0.21). Interactions between BASDAI and sex, and between BASDAI and mSASSS were tested and excluded. Figure 1 shows the relationship between mSASSS and BASFI/DFI after adjustment for the “confounding effects” of BASDAI in a visual manner. The level of mSASSS is positively associated with the BASFI and the DFI. Especially if the mSASSS is in the highest category (upper 50% of the scale range) the effect is important. Note that even a slight involvement of the spine (mSASSS category 2: 1–6) has a measurable and statistically significant effect on BASFI as well as DFI after adjustment for differences in BASDAI.

Relationship between spinal damage (mSASSS) and physical function (BASFI or DFI) after adjustment for the independent effects of a constant level of disease activity (BASDAI). The categories of mSASSS are chosen in such a way that they can be interpreted as number of vertebral units (two adjacent vertebrae and one intervertebral disc) that are completely fused (bridging). Error bars are 95% confidence intervals around the estimated marginal mean. BASDAI, Bath Ankylosing Spondylitis Disease Activity Index; BASFI, Bath Ankylosing Spondylitis Functional Index; DFI, Dougados Functional Index; mSASSS, modified Stoke Ankylosing Spondylitis Spine Score.
We subsequently investigated the importance of syndesmophytes in explaining variation in BASFI and DFI by replacing mSASSS by the syndesmophyte sum score, the number of affected VUs and the number of VUs with bridges, making use of goodness-of-fit statistics. The lower the QIC, the better the model fits the data.
Expectedly, all subscores of mSASSS were independently contributory to explaining the variation in BASFI (p<0.001 for all three subscores). As compared with the model with mSASSS (QIC = 566), which performed best, the models with the syndesmophyte sum score (QIC = 590), the number of affected VUs (QIC = 622) and the number of VUs with bridges (QIC = 595), but also the model with non-syndesmophyte sum score (QIC = 623), show that syndesmophytes are mainly but not solely responsible for explaining variation in BASFI. A model with syndesmophyte sum score (p<0.001) and non-syndesmophyte sum score (p = 0.002) simultaneously tested (QIC = 568) showed that both components significantly contributed to explaining variation in BASFI. Results with DFI as dependent variable were similar.
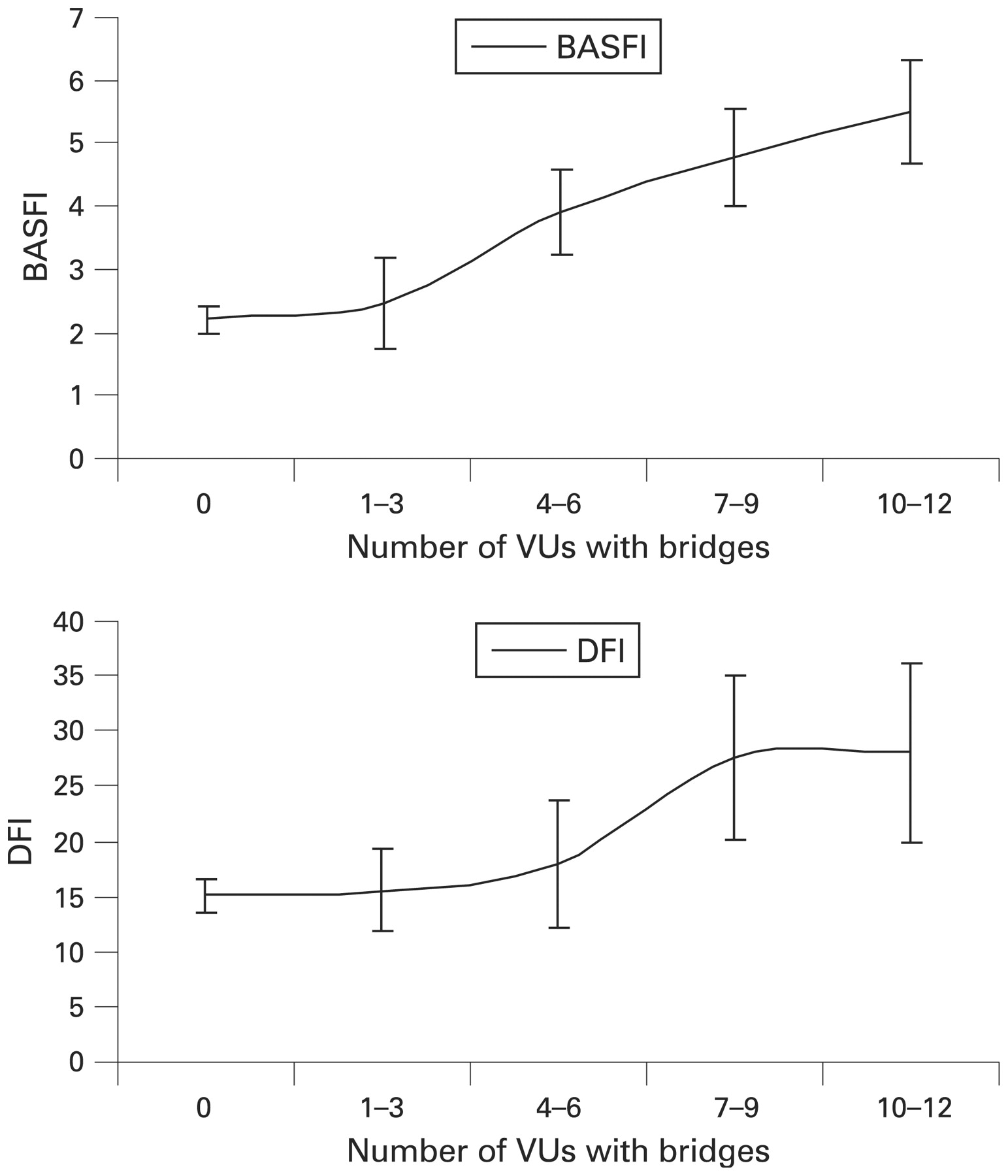
Since the concept of “VUs with bridges” reflects the characteristic picture of AS best (“bamboo spine”), we visualised the independent effect of an increasing number of VUs with bridges on BASFI in fig 2: the more bridges there are, the worse is the BASFI or DFI.

{kind=link}
{kind=link}
Relationship between the number of vertebral units (VUs) with bridging (maximum 12) and physical function (BASFI or DFI) after adjustment for the independent effects of a constant level of disease activity (BASDAI). Error bars are 95% confidence intervals around the estimated marginal mean. BASDAI, Bath Ankylosing Spondylitis Disease Activity Index’ BASFI, Bath Ankylosing Spondylitis Functional Index; DFI, Dougados Functional Index.
Finally, we investigated the relative contribution of the lumbar and the cervical spine to explaining variation in BASFI and DFI. Using either mSASSS, or syndesmophyte sub score, or number of affected VUs or number of VUs with bridges, it was shown that lumbar and cervical involvement of the spine contributed independently, and almost similarly, to explaining variation in BASFI and DFI (data not shown).
DISCUSSION
This analysis proves that physical function, measured by two different patient-reported questionnaires (BASFI and DFI), is determined by the level of patient-reported disease activity (BASDAI) and independently of that by the level of structural damage (mSASSS). This conclusion closely resembles the situation in RA where physical function is partly determined by reversible components such as disease activity and partly by irreversible components (radiographic damage). BASDAI reflects patient-reported outcomes such as pain in the back and joints, fatigue and stiffness, and has been shown to be reversible upon treatment with non-steroidal anti-inflammatory drugs18 and especially TNF-blocking drugs.19 mSASSS primarily reflects syndesmophyte formation and bridging, which is structural and irreversible. This study clearly shows that if BASDAI is at a low level (patients report no complaints), structural damage may cause important impairments in physical functioning, which is a strong justification for the assessment of structural damage by regular x-ray examinations of the spine and the development of treatment that may interfere with the formation of syndesmophytes. Even if drugs can bring a patient into complete symptomatic remission, physical function will remain impaired owing to the structural damage in the spine. Interestingly, TNF-blocking drugs are extremely effective in reducing pain, fatigue and stiffness, and accordingly improve physical function as measured by the BASFI and DFI. However, two different TNF-blocking drugs have been shown not to be effective in inhibiting the formation and growth of syndesmophytes over a 2-year period.6 7 If true, TNF-blocking drugs will not be able to prevent the development of some irreversible function loss in patients with AS, which may raise the hypothesis that syndesmophyte formation and growth occur through TNF-independent mechanisms.20 21
It was shown too that lumbar and cervical involvement contributed similarly and independently to functional impairment of patients with AS. The interpretation of this finding is that impairment of physical function in patients without radiographic lumbar involvement but with cervical involvement may be affected as much as in patients with the opposite involvement.
An interesting finding of this study is that syndesmophytes as well as abnormalities not due to syndesmophytes, such as erosions, sclerosis and squaring, both contribute to functional impairment. It was clear that the models including both aspects of mSASSS performed better than the models including only one part. Although the mSASSS is dominated by syndesmophytes, this study indicates that the other abnormalities that are scored according to mSASSS also affect physical function, though the effect of syndesmophytes is stronger. This could not be an assessment artefact (the phenomenon that a score of 1 (erosion, sclerosis, squaring) is more easily given if scores of 2 and/or 3 (syndesmophytes) are present), since the contribution of the non-syndesmophyte score is not over-ruled by the syndesmophyte score in the model, and remains independently present. Thus, these data underline the validity of the mSASSS as it is, and form a strong argument against a simplification of the mSASSS into a syndesmophyte score. In this study, the data indicate that any radiographic abnormality that is attributable to AS may independently contribute to impaired physical function.
One matter for consideration is that mSASSS measures only part of the spine. Important anatomical structures, such as the thoracic spine and the facet joints, or the posterior ligaments of the vertebrae are not assessed at all. It is likely, however, that abnormalities in these structures go along with abnormalities at sites measured by the mSASSS. As an example, the subtle relationship between low-grade mSASSS abnormalities and physical function could be explained by unmeasured but present abnormalities in the facet joints. Similarly, the association between the rather subtle abnormalities assessed in the non-syndesmophyte sum score and physical function may actually be due to concomitant but unmeasured abnormalities in facet joints or other anatomical structures.
An important limitation of this study is that it does not—and cannot—take into consideration that patients with AS can often cope very well with their limitations. The consequence of coping might be that functional impairment is underestimated by patient-reported functional assessments. If so, however, the association between mSASSS (which is an objective measure of damage) and BASFI/DFI is underestimated rather than overestimated, and the true relationship might be even stronger. Another limitation is that BASFI and DFI scales are anchored at 0 and 10 (BASFI) or 0 and 40 (DFI), which makes them vulnerable to ceiling effects, as shown in this study. This ceiling effect may importantly hinder the demonstration of multivariate associations: If, as is shown here, there is a high level of collinearity (eg, between BASDAI and BASFI), BASDAI at high levels entirely “fills up” the potential of BASFI to express a further contribution of the mSASSS. It is important to recognise that the lack of correlation between mSASSS and BASFI/DFI in the highest quintile(s) of BASDAI does not imply that in such circumstance mSASSS is not contributory any more. The lack of correlation is simply a limitation of metric properties of the instruments measuring physical function. Similar arguments apply for mSASSS, which has a maximum score of 72, which is not necessarily similar to complete ankylosis, since mSASSS does not include the thoracic spine that may contribute to significant additional loss of physical function.
In summary, this analysis clearly proves that patient-reported physical function is dependent not only on patient-reported signs and symptoms (disease activity) but also on the level of structural damage. Optimal treatment of AS should not only include strategies aiming at relieving pain, stiffness and fatigue, but also treatments specifically targeting syndesmophyte formation and growth.
REFERENCES
Footnotes
Competing interests: None declared.
Ethics approval: Ethics committee approval obtained.