Article Text

Abstract
Objective: High-density lipoprotein (HDL) antiatherogenic functions seem to be diminished during inflammatory conditions such as rheumatoid arthritis (RA). The aim of this study was to investigate the effects of tumour necrosis factor (TNF) inhibition on the antioxidative capacity of HDL in RA.
Methods: Plasma lipids and paraoxonase (PON-1) activity were investigated in 45 RA patients, before and during 6 months of anti-TNF therapy. In addition, HDL was isolated and tested for its ability to inhibit copper-induced oxidation of low-density lipoprotein in vitro.
Results: Plasma HDL concentrations did not change considerably after 6 months of therapy. However, stable increases of PON-1 activities were observed throughout the same period (p<0.03). The increases were more obvious when related to HDL or apolipoprotein AI concentrations. HDL total antioxidative capacity significantly improved 6 months after the initiation of anti-TNF therapy (p = 0.015). The initial improvement of PON-1 activity paralleled a decrease in the inflammatory status, whereas specific TNF blockade was likely to be responsible for the long-term effects.
Conclusions: Anti-TNF therapy with infliximab has beneficial effects on lipids through changes in HDL antioxidative capacity, which might be clinically relevant and contribute to the reported protective effect of anti-TNF on cardiovascular morbidity in RA. This emphasises the importance of HDL antiatherogenic capacity for cardiovascular risk in chronic inflammatory conditions.
Statistics from Altmetric.com
Cardiovascular diseases (CVD) remain the major cause of death in developed countries, despite a recent reported decrease in their incidence.1 A growing body of evidence underlines the crucial role of inflammation in the development and instability of atherosclerotic plaques. Consistent with that, patients with chronic inflammatory diseases, such as systemic lupus erythematosus and rheumatoid arthritis (RA) have increased CVD morbidity. It is believed that an adequate control of inflammation in patients with RA or systemic lupus erythematosus not only ameliorates disease-related symptoms but also reduces CVD risk. Various epidemiological studies have recently indicated that anti-tumour necrosis factor (TNF) therapy is associated with decreases in cardiovascular-related mortality in RA.2 3 It is not yet clear whether this effect is mainly due to the blockade of TNF-α itself or if it is more related to the overall suppression and control of inflammation in these patients.
An increase in high-density lipoprotein (HDL) cholesterol plasma concentrations has been constantly reported shortly after anti-TNF therapy has been initiated and this is likely to mirror an important decrease in the inflammation and acute phase reaction.4 Nevertheless, this increase in HDL was not sustained during long-term TNF-α blockade in RA patients.5 Corroborated with the epidemiological studies,2 3 this ultimately suggests that measuring HDL plasma concentrations would yield limited information concerning the CVD risk in these patients, and therefore HDL functional qualities may have a greater impact than its concentration in determining the CVD risk.
HDL antiatherogenic properties are represented by its capacity to neutralise oxidised lipids and to extract cholesterol from peripheral tissues, initiating the reverse cholesterol transport. The HDL component mainly responsible for the antioxidative effects is paraoxonase (PON-1). Compared with healthy controls, PON-1 concentrations are decreased in RA patients6–8 and this probably contributes to the recently reported lower HDL antioxidative capacity in these patients.8 In different cohorts, including that of the Framingham study, high HDL-cholesterol concentrations were not always associated with a low CVD risk,9 10 suggesting that other HDL markers, such as those responsible for its antioxidative capacity and/or cholesterol efflux from the periphery, may also be of great importance in this respect.
The aim of this study was to investigate the effects of anti-TNF therapy on the antioxidative capacity of HDL in RA. We hypothesised that TNF blockade may also modify the antioxidative capacity of HDL and this, combined with the effects on the HDL concentration, could offer a better perspective on the CVD protective value of HDL in these patients. To test the antioxidative capacity of HDL, we have investigated the paraoxonase and arylesterase activities of PON-1.
PATIENTS AND METHODS
Patients
Between January 2005 and December 2006 a group of 45 consecutive patients with RA fulfilling the 1987 American College of Rheumatology criteria were investigated in this study. All patients had active disease (disease activity score (DAS28) >3.2) at baseline and were about to start therapy with a TNF-α blocker (infliximab). Patients were attending the outpatient rheumatology clinic of the St Maartenskliniek in Nijmegen and entered the study after giving written informed consent. The Regional Medical Ethical Committee approved the study. Infliximab (3 mg/kg) was given in infusions at baseline and at 2 weeks, 6 weeks and thereafter every 8 weeks. The mean age of the RA group was 56 years (SD 11) and the disease duration was 7.9 years (SD 6.0). Of the patients, 70% were women and 60% were positive for the rheumatic factor. The group was followed for a period of 6 months. Seventeen (37%) RA patients were smokers and seven patients (17%) had ever experienced an acute cardiovascular event, as documented in the patient clinical charts. No changes in body weight were observed during this period (table 1). Besides infliximab, stable dosages of disease-modifying antirheumatic drugs were allowed during the study. Patients receiving prednisone or lipid-lowering drugs were excluded from the study. Disease activity (DAS28) and laboratory parameters were assessed regularly before each infliximab infusion.
Lipid measurements
Fasting blood was collected in vacutainer tubes (Beckton Dickinson, Rutherford, New Jersey, USA) containing K3-EDTA (1 mg/ml), and a sample was taken in a tube without anticoagulant to obtain serum. Tubes were centrifuged at 3600 rpm for 8 minutes at 4°C, supplemented with saccharose as a cryoprotectant (final concentration 6 mg/ml) and frozen at −80°C until assay. Serum levels of plasma total cholesterol, triglycerides and HDL-cholesterol were determined enzymatically on a Hitachi 747 analyser. Low-density lipoprotein (LDL) cholesterol levels were calculated according to the Friedewald formula, which provides reliable values up to a triglyceride concentration of 4.0 mmol/l. Apolipoprotein AI (ApoAI) concentrations were determined by immunonephelometry.
Analysis of PON-1 enzymatic activity
Paraoxonase and arylesterase activities were analysed spectrophotometrically in flat-bottomed UV transparent 96-well plates (Greiner Bio-One, Alphen aan den Rijn, The Netherlands). Serum paraoxonase hydrolytic activity was determined by the addition of 5 μl serum in 0.1 mol Tris/HCl, pH 8.5, 0.9 mmol calcium chloride and 30 nl diethyl p-nitrophenylphosphate (Sigma Aldrich BV, Zwijndrecht, The Netherlands) in a final volume of 200 μl. The reaction was monitored for 10 minutes at 37°C. Serum arylesterase activity was determined by the addition of 0.25 μl serum in 0.1 mol Tris, pH 8.5, 0.9 mmol calcium chloride and 34 nl phenylacetate (Sigma Aldrich) in a final volume of 200 μl. The reaction was monitored for 5 minutes at 37°C for the linear increment of absorbance at 280 nm. For paraoxonase activity the coefficients of variation (CV) were 5% for intraplate variability and 6% for interplate variability. For arylesterase activity the intraplate CV was 8% and the interplate CV was 10%. Paraoxonase and arylesterase activities are expressed as units per litre of serum, where 1 unit equals 1 μmol of substrate hydrolysed per minute.
In-vitro LDL oxidation assay
As a measure of the antioxidative capacity of HDL, we assessed the inhibitory effect of isolated HDL on in-vitro copper-induced LDL oxidation. LDL was obtained by ultracentrifugation11 from EDTA plasma frozen in the presence of saccharose (0.6% (w/v) final concentration) at −80°C. LDL oxidation (61 μg apolipoprotein/ml) was initiated by the addition of copper sulphate to a final concentration of 18 μmol12 and performed in the presence and absence of HDL (61 μg apolipoprotein/ml) at 30°C. HDL of the patients was isolated by single-spin density-gradient ultracentrifugation. Protein of LDL and HDL preparations was measured using bovine serum albumin as standard and with chloroform extraction of the colour solution to remove turbidity. The kinetics of the oxidation of LDL was determined by monitoring the change in diene absorption in a thermostatic ultraviolet spectrophotometer at 234 nm (Lambda 12; Perkin Elmer GmbH, Rodgau-Jügesheim, Germany). The oxidation characteristics of LDL were determined by the lag time (minutes), the oxidation rate (nmol dienes/mg protein per minute) and the maximal amount of dienes formed during LDL oxidation (nmol/mg LDL protein) as previously described.13 Within and between-run CV were 3.8% and 6.5% for lag time, 5.8% and 8.2% for oxidation rate and 2.2% and 5.0% for the maximal amount of dienes formed.
Statistical analysis
For non-parametric values comparisons were made using the Wilcoxon signed rank test. The differences between values of variables at baseline and after treatment were performed using the paired Student’s t-test. Correlations between inflammatory status markers and lipids were determined using the Spearman test. Significance was set at the level of 0.05. Values are expressed as mean ± SD, unless otherwise stated.
RESULTS
Anti-TNF effects on lipid concentrations and inflammatory status
At baseline all patients had active disease: erythrocyte sedimentation rate (ESR) 31 mm/h (SD 19), DAS28 5.26 (SD 1.24). Six months following infliximab therapy, ESR and the DAS28 had decreased by more than 50% and 30%, respectively, from baseline (p<0.001 compared with baseline). In addition, lipid concentrations changed during TNF blockade: total cholesterol, HDL-cholesterol and ApoAI significantly increased 2 weeks after therapy was initiated (p<0.01) (table 1). Eventually, an increase of the atherogenic index (as expressed by the total cholesterol : HDL-cholesterol ratio) was observed after 6 months of therapy, mainly due to a slight decrease in HDL-cholesterol concentrations at this time point (table 1).
Anti-TNF effects on PON-1 activities
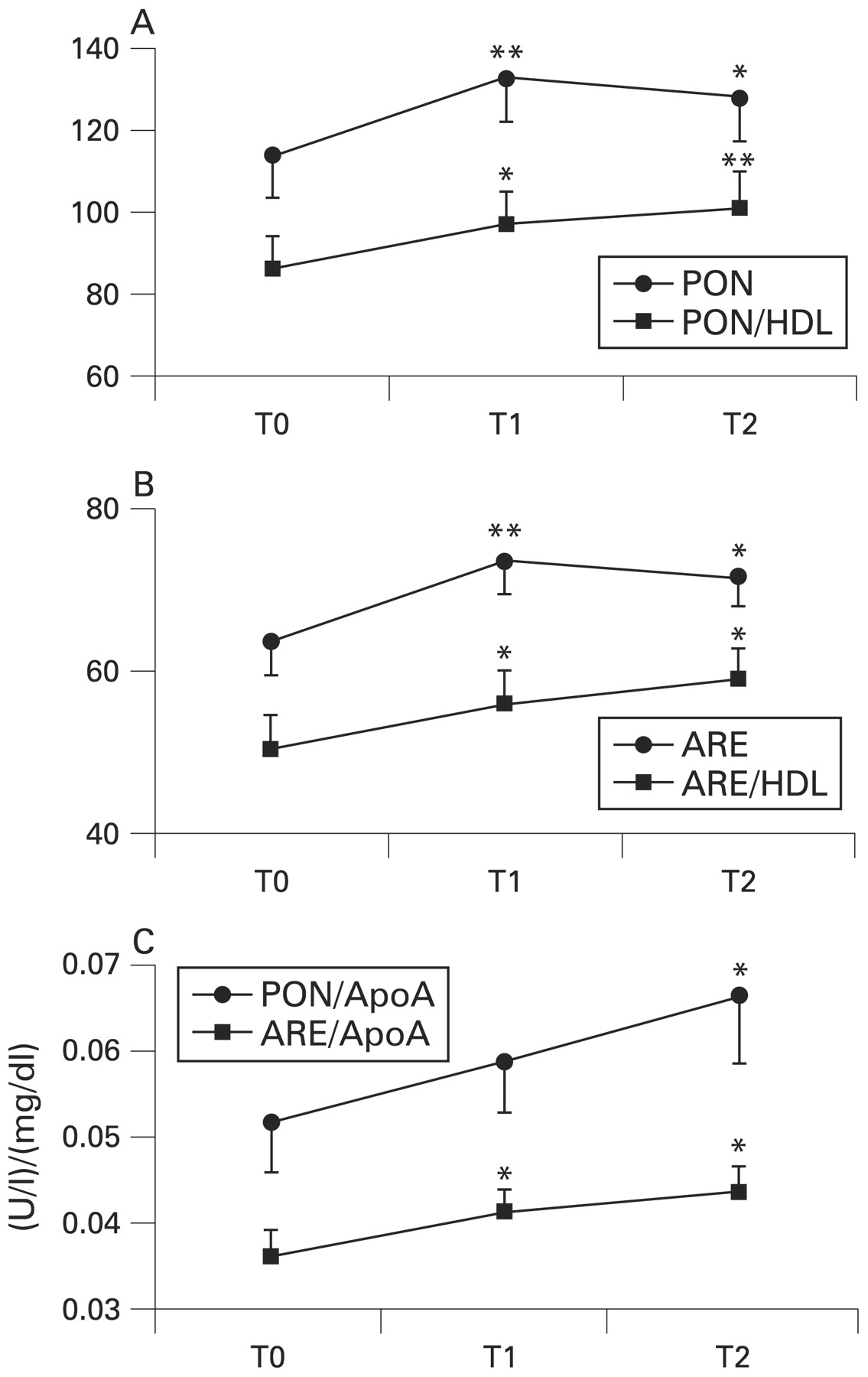
PON-1 was further investigated as the main enzyme situated on HDL responsible for its antioxidative capacity. In our study population, the paraoxonase activity of PON-1 significantly increased after 2 weeks from the first infusion (p = 0.002) and also remained high after 6 months (p = 0.018) (fig 1A). The same trend was observed in arylesterase activity after 2 weeks and 6 months (p = 0.003 and p = 0.022, respectively) (fig 1B). To assess better the capacity of one HDL molecule to neutralise the effects of oxidised lipids, we investigated the ratios between paraoxonase activity and HDL on the one hand, and arylesterase activity and HDL on the other, respectively. A higher value of this ratio would indicate a higher antioxidative capacity of one single HDL molecule. Both paraoxonase : HDL and arylesterase : HDL ratios had increased significantly already 2 weeks after the initiation of therapy with infliximab (fig 1A) and, unlike paraoxonase and arylesterase activities, continued to increase slightly up to 6 months of therapy (p = 0.008 for the paraoxonase : HDL ratio and p = 0.011 for the arylesterase : HDL ratio, respectively) (fig 1B). The same results were seen when the enzyme activities were related to ApoAI concentrations (fig 1C). The ratio between paraoxonase and arylesterase remained stable throughout the study period (not shown).

Changes in paraoxonase (PON) activity (PON (U/l), PON/HDL (U/mmol)) (A), arylesterase (ARE) activity (ARE (U/l), ARE/HDL (U/mmol)) (B), and the ratio of them with high-density lipoprotein (HDL) cholesterol and, respectively, with apolipoprotein AI (ApoAI) (C) plasma concentrations during anti-tumour necrosis factor therapy. T0, baseline; T1, 2 weeks; T2, 6 months. **p<0.01, *p<0.05 versus baseline.
Anti-TNF effects on total HDL antioxidative capacity
In order to test the impact of PON-1 activity changes on HDL overall antioxidative capacity, we isolated HDL of the last 15 patients consecutively enrolled in the study and tested its capacity to inhibit LDL oxidation in vitro. Due to our initial observations indicating no effect of long-term therapy with infliximab on plasma HDL concentrations, we only tested the antioxidative capacity of HDL before and 6 months after anti-TNF therapy was initiated. We observed an increased lag time of LDL oxidation in the presence of HDL obtained 6 months after anti-TNF was initiated compared with baseline HDL (p = 0.015) (fig 2). The LDL oxidation rate and maximal amount of dienes formed did not significantly differ between both conditions. These findings suggest that the overall HDL antioxidative capacity improved after long-term infliximab therapy.

Changes in high-density lipoprotein antioxidative capacity as measured by means of an in-vitro low-density lipoprotein oxidation assay. Black horizontal lines represent the means. T0, baseline, T2, 6 months. *p<0.05 versus baseline.
Inflammatory markers and PON-1 activity
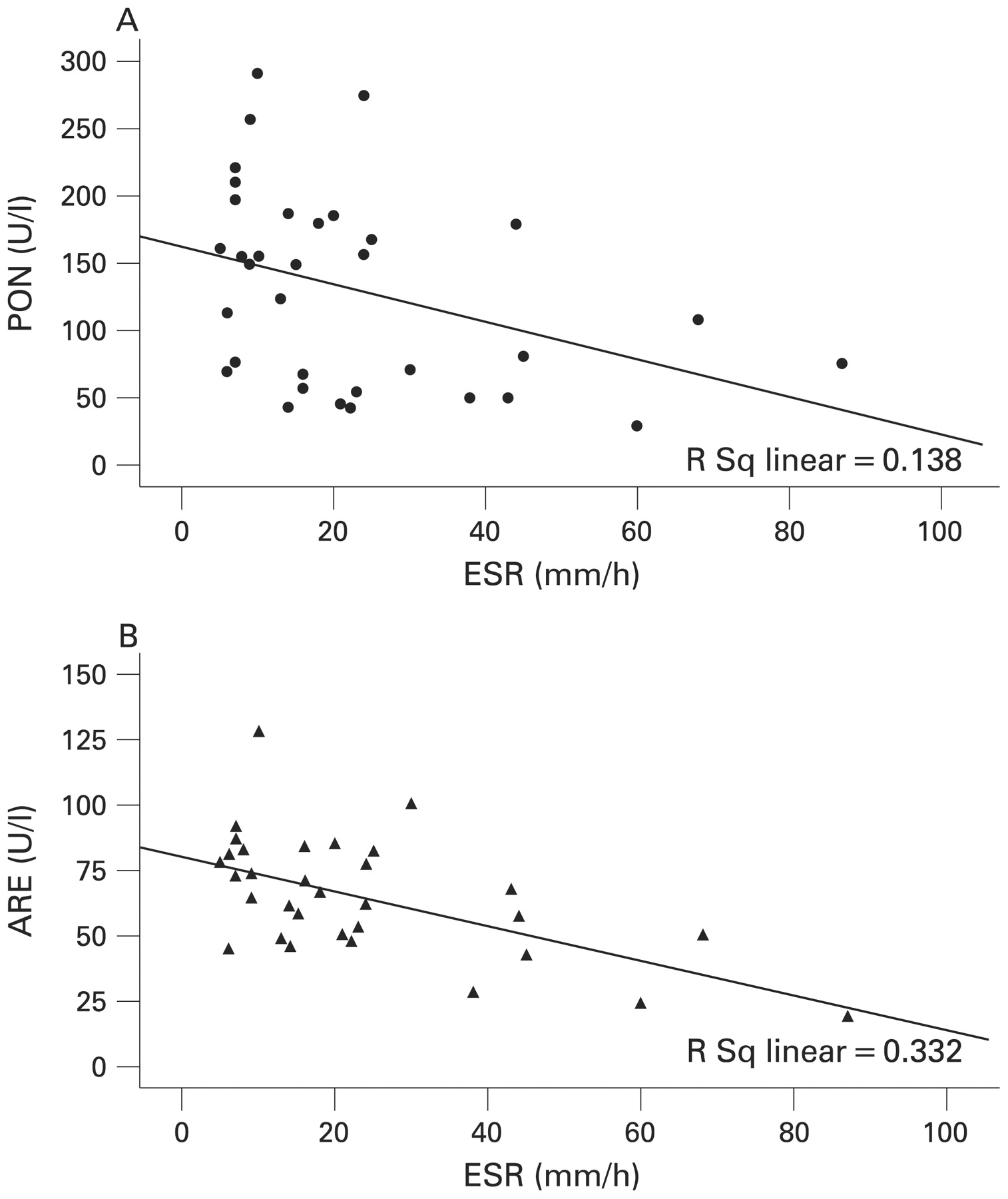
In order to investigate whether these changes in PON-1 activities were due to specific TNF inhibition or an overall decrease in inflammation, correlations between PON-1 activities and ESR and DAS28 were performed (table 2). Inverse correlations with ESR were observed for paraoxonase (r = −0.37, fig 3A) and for arylesterase activities (r = −0.58, fig 3B) 2 weeks after the start of therapy, but these relations became weaker after a half year of TNF blockade (table 2).
{kind=link}
{kind=link}
{kind=link}
Correlations between erythrocyte sedimentation rate (ESR) and high-density lipoprotein (HDL) paraoxonase (PON) activity (A) and HDL arylesterase (ARE) activity (B) at 2 weeks after the initiation of therapeutic tumour necrosis factor blockade.
DISCUSSION
In the present study we report for the first time that in RA patients therapy with infliximab causes sustained increases in paraoxonase and arylesterase activities of PON-1 on HDL-cholesterol molecules, whereas it only transiently raises the concentrations of HDL-cholesterol. We suggest that by increasing the antioxidative capacity of HDL, infliximab may improve HDL antiatherogenic capacity.
RA patients treated with anti-TNF therapy were recently reported to show a decreased incidence of cardiovascular events compared with those on other antirheumatic medication.2 3
HDL is one of the most stable clinical predictors of future CVD events. Two mechanisms are mainly responsible for its antiatherogenic effects: (1) its antioxidative capacity, neutralising oxidised lipids and (2) its capacity to promote cholesterol efflux from vessels and to transport it to the liver for excretion.14 In order to exert its antioxidative function, the HDL particle harbours the antioxidative enzyme PON-1, which is one of the most potent circulating enzymes in counteracting the pro-atherogenic effect of oxidised lipids.15 In our study we show for the first time that therapeutic TNF blockade using infliximab is able robustly to improve HDL antioxidative capacity by increasing its PON-1 activities. This was further emphasised and corroborated in an additional smaller group of patients, using a direct cell-free assay. Besides the increase in PON-1 activities, this therapy induced a significant improvement of the whole HDL antioxidative capacity in this group. Proinflammatory cytokines, including TNF, have previously been shown to suppress the hepatic synthesis of PON-1.16 17 Although we have not directly assessed circulating PON-1 levels, it is likely that they may increase when TNF is blocked. Therefore, we hypothesise that the increase in PON-1 activities during anti-TNF can be explained by an increase in hepatic PON-1 synthesis, which is now free of TNF inhibitory effects. In addition, the decrease in other TNF-driven pro-inflammatory cytokine concentrations could also have the same effect on hepatic PON-1 synthesis during therapy.
We tried to elucidate whether these changes in PON-1 activities are due to the overall decrease in inflammation or to the therapy itself. Our results suggest that early after therapy was initiated the overall decrease in inflammatory status plays an important role in the HDL antioxidative capacity. However, this role appears to have diminished after 6 months of therapy. This is mainly suggested by the fact that between 2 weeks and 6 months HDL antioxidative capacity, as assessed by PON : HDL, ARE : HDL, PON : ApoAI and ARE : ApoAI ratios, preserved its tendency to increase, whereas inflammatory status changed its initial decreasing trend into a slight increase. These findings would further suggest that the prevention of TNF-induced suppression of hepatic synthesis of PON-1 by anti-TNF antibodies is also important in improving HDL antioxidative capacity, especially later in the course of therapy. Increasing the capacity of HDL to dampen the atherogenic effects of oxidised lipids could represent one mechanism through which infliximab might be antiatherogenic and contributes to the recently reported reduction in the incidence of CVD in RA patients treated with these drugs.2 3 One note of caution should be emphasised, however, as it is not clear whether this increase in HDL antioxidative capacity reported here contributes to diminished CVD morbidity, because TNF blockade has been shown previously also to improve other CVD risk factors in RA, including endothelial function and insulin sensitivity.18–20 On the other hand, the increase in the atherogenic index following long-term therapy with infliximab suggests that the lipid concentration pattern in RA patients appears to be less predictive of CVD risk than in the general population. This would also explain the progression of subclinical atherosclerosis found by some investigators in patients on long-term anti-TNF therapy.21 Conversely, others have indicated neutral long-term effects of TNF blockers on lipid concentrations of RA patients,22 with factors related to disease activity, (co)medication, dietary intake and physical activity being most probably responsible.
In our study, the immediate effects of the overall decrease in inflammation were difficult to delineate from those produced by the specific blockade of TNF effects on the circulating lipid pattern. Although it is very likely that the antioxidative effects observed with infliximab in the present study would also occur in response to other anti-TNF agents, further studies are needed in order to prove this hypothesis.
In conclusion, our study shows a beneficial effect of infliximab through changes in the composition of the HDL particle leading to improved antioxidative properties. Such changes are clinically relevant because they could contribute to the protective effect of anti-TNF therapy on CVD morbidity in RA. Furthermore, our results underline the importance of evaluating HDL antioxidative properties in addition to HDL concentrations, especially in those populations in which the predictive value of traditional cardiovascular risk factors is limited.
REFERENCES
Footnotes
Competing interests: None.
Funding: CP was supported by “De Drie Lichten” Foundation in The Netherlands. MGN and TRDJR were supported by a VIDI and, respectively, VENI grant from the Netherlands Organization for Scientific Research (NWO).
Ethics approval: The Regional Medical Ethical Committee approved the study.
Patient consent: Obtained.