Article Text

Abstract
Background: Systemic sclerosis (SSc) is a vasculopathy with increased tissue deposition of collagen. The aetiology is unknown. Genetic and environmental susceptibility factors have been implicated. It is unknown whether disease presentation varies within Europe.
Aims and Methods: The baseline data of all SSc patients entered in the EULAR Scleroderma Trials and Research (EUSTAR) database up to April 2007 were analysed for geographical differences with regard to organ involvement, and geographical clusters with regard to clinical subsets (diffuse vs limited SSc) and autoantibodies (anticentromere vs anti-Scl70).
Results: 3661 patients from 79 centres in 62 cities and 23 countries were analysed. There was no clear trend between geographical coordinates and SSc subsets, although there appeared to be an increased prevalence of Scl70 in the more eastern centres. There was no association between geographical longitude or latitude and the age at the onset of Raynaud’s phenomenon or the onset of non-Raynaud’s symptoms. There was also a trend for the more eastern centres to care for patients with a higher prevalence of more severe organ manifestations (pulmonary arterial hypertension, cardiac involvement). Between different centres within one city there was a large variability in the frequency of organ complications.
Conclusion: This analysis suggests that eastern centres care for more severe SSc manifestations in Europe. Large differences in patient referral account for a large local variability of SSc presentations and preclude the identification of genetic or environmental factors.
Statistics from Altmetric.com
Systemic sclerosis (SSc) is a fibrotic vasculopathy of autoimmune origin. According to the extent of skin involvement, SSc is phenotypically subdivided into two prognostically relevant subsets, a limited form (lcSSc) and a diffuse form (dcSSc).1 In addition to these clinical SSc subsets, the presence of two specific autoantibodies, the anticentromere antibodies (ACA) and the antitopoisomerase I (anti-Scl70) are associated with organ manifestations.2
The aetiology of SSc is unknown but genetic susceptibility factors have been associated with autoantibody status3 4 and the disease itself. Choctaw native Americans, for example, have a markedly increased incidence of SSc.5 SSc also occurs significantly more frequently in families with SSc than in the general population.6 Further evidence for genetic factors in the aetiology of SSc stems from twin studies in which monozygotic twins were found to have a significantly higher concordance rate for antinuclear antibodies (95%) than dizygotic twins (60%).7 The overall concordance of SSc in twin studies was, however, low and was identical between monozygotic and dizygotic twins, indicating that genetic factors are not sufficient to explain the onset of the disease.7
Environmental factors have also been reported to cause skin sclerosis. Occupational exposure to silica dust, vinyl chloride, epoxy resins, organic solvents and exposure to certain toxins (bleomycin, l-5-hydroxytryptophan, l-tryptophan and gadolinium), for example, are known to induce a SSc-like syndrome.8–12 None of the environmental exposures, however, were found to be associated with true SSc.13 14
The analysis of geographical variations among different SSc presentations and autoantibody associations could help in identifying genetic or environmental factors. Large geographical variations in SSc prevalence and incidence have been described,15 but differences with regard to the individual disease presentations have mostly not been studied. In this rare disease, the total number of patients in a region is usually small. Therefore both SSc subtypes were pooled in most analyses, thus rendering it more difficult to interpret the data and possibly also obscuring a significant increase in individual disease presentations. Geographical variations may also vary with regard to autoantibody associations and in the female-to-male ratio. Finally, the geographical clustering reported so far examined the prevalence of SSc in a relatively small geographical area.
The availability of the large EULAR Scleroderma Trials and Research group (EUSTAR) database, which was formed in June 2004, and since then has prospectively followed SSc patients in most European countries, and the limitations of previous studies prompted us to examine the geographical variations of SSc disease manifestations. We aimed to obtain data on the regional distribution of SSc presentations that could be indicative of genetic or environmental risk factors and at the same time could be used in determining the cost of SSc to the economy of countries and thus more accurately allocating healthcare resources.
PATIENTS AND METHODS
The EUSTAR database and geographical coordinates
The structure and the minimal essential dataset of the EUSTAR database have been described previously.2 SSc cases in the EUSTAR database entered up to 6 April 2007 were analysed cross-sectionally. For each patient, only the baseline data from the first visit in European EUSTAR centres were analysed.
Geographical coordinates were gathered using the ArcGIS software and data package (version. 9.2). Latitude is represented by degrees ranging from 0° at the equator to 90° at the north pole. Longitude is represented as a measurement ranging from 0° at the prime Greenwich meridian to +180° eastward and −180° westward and the west/east suffix is replaced by a negative sign in the western hemisphere. Decimal fractions of degrees and minutes were used for statistical calculations (table 1).
Bivariate and partial correlations
In a first step, bivariate correlations (Pearson) between geocoded data and SSc disease presentations were generated using the SPSS (version 15.0) statistical package. In a second step, partial correlations were computed in order to confirm bivariate correlations. In these partial correlations, adjustment was made for the confounding effect of variables previously shown to be the principal determinant of this particular organ manifestation in the same cohort.2 These confounders, which were controlled for, included autoantibody status, clinical SSc subtype and the patients’ age at the onset of Raynaud’s phenomenon (table 2).
Cluster analysis
Clustering is the classification of objects into different groups, or more precisely, the partitioning of a dataset into subsets (clusters), so that the data in each cluster ideally share some common trait. Cluster analyses were run on disease presentations and autoantibody status (Scl70 and ACA). Cluster analysis was performed using Latent Gold (version 4.0) with the aim of identifying latent subgroups and to generate models.16
Within-city variations
In order to assess referral bias as a cause of variations between centres, we analysed the distribution of disease presentations and autoantibody status in single cities, provided that these cities had at least two different EUSTAR centres, each with at least 15 SSc patients. The frequencies of SSc subsets and autoantibodies and their variances were calculated for the different EUSTAR centres within a single European city and their variances were then compared using Levene’s testing. Levene’s test assesses the null hypothesis that the population variances are equal. Significant differences in sample variances are unlikely to have occurred based on random sampling, and therefore indicate that the populations are not equal between a single geographical location.
RESULTS
As of April 2007, a total of 4712 patients fulfilling the American College of Rheumatology (ACR) criteria for SSc was enrolled in EUSTAR. On a worldwide basis, data were from 122 centres in 102 cities and 23 countries. A total of 1770 (37.6%) patients had dcSSc, 2717 (57.7%) patients had lcSSc and 225 (4.8%) had scleroderma in combination with another connective tissue disease. There were 3847 documented patients with ACR-confirmed SSc in Europe. Data were restricted to SSc patients from European cities with more than 15 documented patients. A total of 3661 patients in 79 centres in 61 cities and 23 countries was thus subsequently analysed (table 1).
Among these 3661 patients, 1390 (38.0%) patients had dcSSc and 2263 (62.0%) patients had lcSSc. The clinical subset was not known in eight patients; 86.5% of the 3661 patients were women. The mean age of all 3661 SSc patients was 54.9 years (SD 13.6), 51.8 years for patients with dcSSc and 56.9 years for patients with lcSSc.
Bivariate correlations
On bivariate analysis, there was no association between either clinical SSc subset (dcSSc or lcSSc) and geographical longitude or latitude. Similarly, there was no association between geographical position and the patient’s age, the patient’s age at the onset of Raynaud’s phenomenon and the age of onset of the first non-Raynaud’s symptoms of the disease. Furthermore, there was no regional imbalance with respect to the modified Rodnan skin score (mRSS) and disease activity, either with regard to a composite score from the minimal essential dataset features according to the preliminary index for SSc,17 or with regard to acute-phase reactants (erythrocyte sedimentation rate or C-reactive protein).
Interestingly, however, women with SSc were significantly more frequently reported in western regions compared with eastern regions (r = −0.35, p = 0.005). Scl-70 positivity was more frequently represented in eastern regions (r = 0.28, p = 0.03). Notably, digital ulcers were more frequent in western regions (r = −0.32, p = 0.01). The frequency of digital ulcers was, however, not associated with geographical latitude. Interestingly, an increased frequency of pulmonary arterial hypertension (PAH) was not only more frequently assessed by echocardiography in eastern centres (r = 0.29, p = 0.02), but was also more prevalent at low geographical latitudes (eg, in the south, r = −0.32, p = 0.002). Similarly, a diminished diffusion capacity of the lung for carbon monoxide (DLCO) was also more prevalent in the south (r = −0.35, p = 0.01).
Partial correlations
After adjusting for autoantibody status, the significant association of an increased prevalence of women in western longitudes detected in the bivariate correlations persisted (r = −0.29, p = 0.02), but vanished after controlling for clinical SSc subsets (r = −0.079, p = 0.54).
Similar to the bivariate correlations, there was no association between geographical longitude or latitude and the age at the onset of Raynaud’s phenomenon, the onset of Raynaud’s and non-Raynaud’s symptoms after adjusting for SSc subsets, autoantibody status, or gender.
We then adjusted disease characteristics (“variables”) for confounders previously identified to influence disease presentations (table 2).2 An association between pulmonary fibrosis and longitude, which was identified in bivariate correlations, was lost after adjusting for autoantibody status. All the other associations identified in the bivariate analysis persisted after adjustment. After adjustment for autoantibody status, the increased prevalence of digital ulcers in centres located more westerly had almost completely lost significance (r = 0.25, p = 0.049). Unlike in the bivariate correlations, arterial hypertension was more frequently represented in eastern Europe after adjusting for autoantibody status.
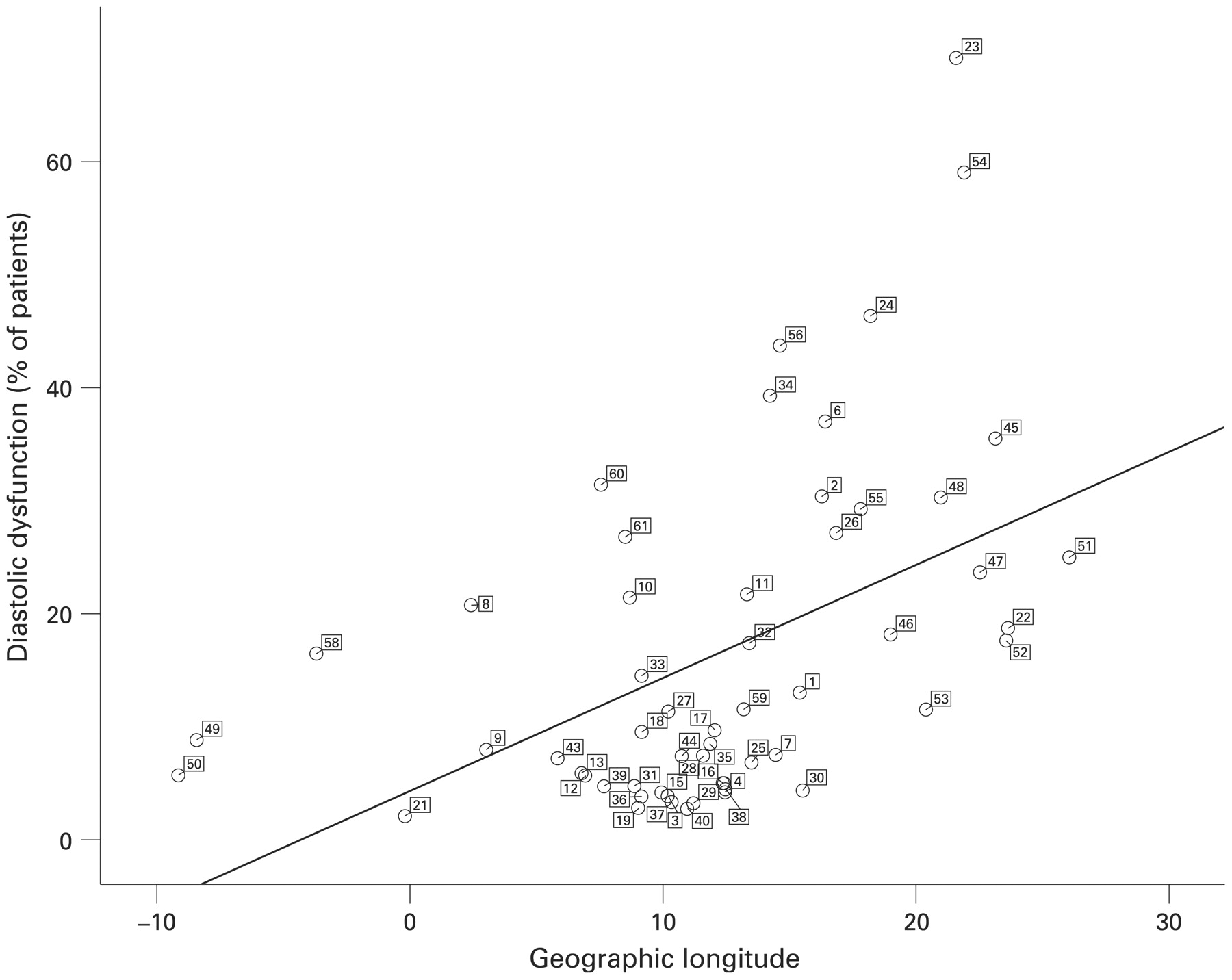
The highest correlation coefficient between disease presentations and geographical position was observed between diastolic dysfunction and longitude (r = 0.51, p = 0.005). The visualisation of the distribution of centres (fig 1) shows, however, that centres that are characterised by a relatively short distance from each other are not characterised by similar frequencies of diastolic dysfunction (fig 1). For example, Frankfurt/Germany and Bad Nauheim/Germany are only 30 km apart, yet the proportion of patients with diastolic dysfunction in Bad Nauheim is relatively high (21.0%) but very low (0.0%) in Frankfurt am Main. Similar observations also apply to Tubingen and Zurich (two cities that are approximately 170 km apart) and to the other significant correlations including the frequency of PAH (not shown).

Frequency of diastolic dysfunction in relation to geographical longitude as a degree measurement in reference to the prime Greenwich meridian. The numbers represent the city ID as indicated in table 1; the line represents the significant positive correlation (r = 0.51, p<0.001).
Cluster analysis
Cluster analysis (also called “latent class analysis”) was performed in order to evaluate data without an a priori hypothesis, and in our setting mainly to identify imbalances in autoantibody status and SSc subsets that do not follow an east–west or north–south trend, but rather are distributed in “pockets”. Variables entered in the cluster analysis were either SSc subsets (dcSSc and lcSSc) or autoantibody status (Scl70 and ACA). Various models with different cluster sizes were computed.
Three cluster solutions turned out to be most informative in that the clusters were clearly distinct from each other. With regard to the three SSc clusters, SSc cluster 1 contained 43%, SSc cluster 2 contained 41% and SSc cluster 3 contained 16% of all centres. SSc cluster 1 was characterised by a low frequency of dcSSc (24.4%) and a high frequency of lcSSc (75.5%). Cluster 2 had a similar distribution of dcSSc and lcSSc (43.8% and 56.2%, respectively) and cluster 3 had a high proportion of dcSSc (76.2%) and a low proportion of lcSSc (23.8%). The cities allocated to each of these clusters are indicated in fig 2.

Cities allocated to each of the three systemic sclerosis (SSc) subset clusters. The figures in the table indicate the frequency of SSc subsets in each cluster. dcSSC, diffuse form of systemic sclerosis; lcSSC, limited form of systemic sclerosis.
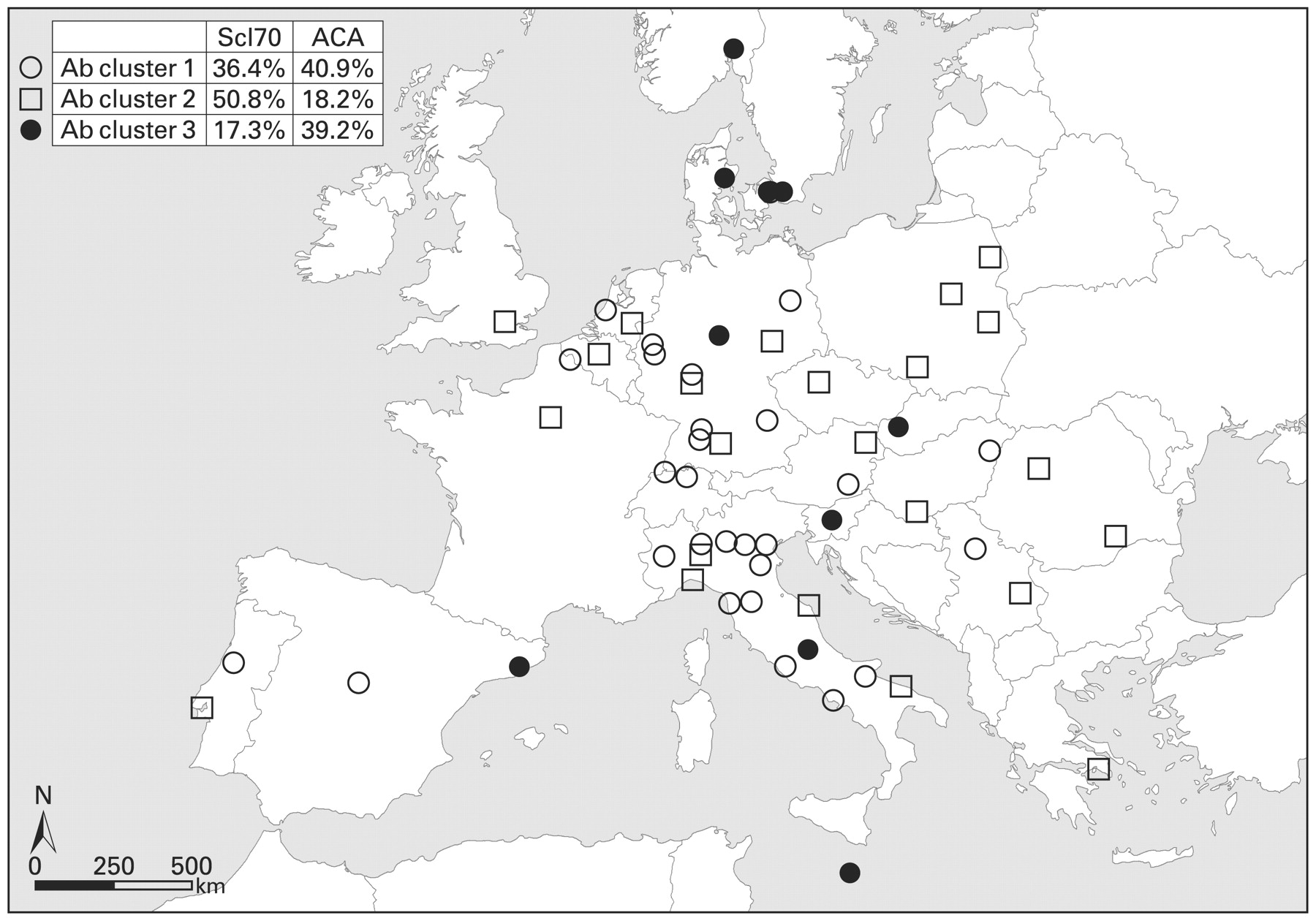
With respect to autoantibody status, the cities also segregated best in three clusters. The first antibody cluster contained 46% of all EUSTAR centres; 36.4% of patients in this cluster had Scl70 autoantibodies and 40.9% had ACA. The second autoantibody cluster contained 38% of all centres and was characterised by a high frequency of Scl70 autoantibodies (50.8%) and a low frequency of ACA (18.2%). The third autoantibody cluster contained the remaining 16% of centres and was characterised by a low frequency of Scl70 autoantibodies (17.3%) and a higher frequency of ACA (39.2%). The cities falling into each of these clusters are displayed in fig 3.
{kind=link}
{kind=link}
{kind=link}
Cities allocated to each of the three autoantibody (Ab) clusters. The figures indicate the frequency of Scl70 autoantibodies or anticentromere autoantibodies (ACA) in each cluster.
Within-city variations
In order to assess geographical variations in referral bias between centres, we analysed the distribution of disease presentations and autoantibody status in different centres within single cities. Twelve cities had more than one EUSTAR centre (table 1). Twelve cities (Berlin, Lublin, Madrid, Milan, Paris and Prague) had two centres with more than 15 SSc patients each (table 3). In five of these six cities, there were significant differences in the distribution of SSc subsets. Significant differences in the prevalence of autoantibodies were noted in two cities. These data demonstrate significant centre per centre variation of key SSc determinants in the absence of geographical difference.
DISCUSSION
We have analysed geographical differences of SSc disease presentations among EUSTAR centres in Europe. Our main finding is that significant differences exist with regard to some disease presentations. There was, however, no clear geographical trend with regard to key factors thought to influence organ involvement of SSc, such as clinical SSc subsets, gender and mRSS. In addition, manifestations relating to ambient temperature such as Raynauds’ phenomenon did not differ. In three regions of Ontario, no significant differences of disease type were found, but the regions did not span a large geographical area and the numbers were limited.14
In northern countries of Europe (England and Iceland), the prevalence rates of SSc were lower, compared with countries within southern Europe (France and Greece).15 Of note, however, our study did not assess SSc prevalence, but rather focused on the disease presentation in those individuals already affected by the disease.
As in any cross-sectional study, ours has limitations. First there is multiple statistical testing, which we have not corrected for and which may have introduced false-positive correlations. Second, only 77.4% of the total of 4733 SSc patients in the EUSTAR database were evaluated. Most of the subjects not analysed were, however, not from European centres, but were distributed over four other continents. Therefore, we expect any selection bias to be small.
The EUSTAR database was inaugurated in 2004. Given the relatively short recruitment period into the EUSTAR database, regional differences in the availability of drugs improving survival are therefore an unlikely explanation for the observed variability of disease presentations.
In our study, however, large differences in SSc disease presentations were observed within a single city and between centres of close geographical proximity. Whereas this fact could be explained by differences in antinuclear antibody assessment between centres and by a variability between observers to differentiate lcSSc from dcSSc,18 a more likely explanation is recruitment bias. Such recruitment bias may arise by the fact that different medical specialties take care of the patients in a given city, attract different patient populations, participate in EUSTAR documentation, or refrain from participation. In Madrid, where only rheumatologists participated in the EUSTAR documentation, SSc subsets and autoantibody prevalence data were similar, whereas SSc populations were dissimilar in cities documented by dermatologists and rheumatologists (table 3).
We cannot, however, rule out ascertainment bias for some of the more observer-dependent variables, as illustrated by the inhomogeneous frequencies of diastolic dysfunction between centres of close geographical proximity (fig 1). In the case of diastolic dysfunction, such differences may be attributed to observer-dependent differences in unstandardised echocardiographic assessment. With regard to similar discrepancies between centres in less observer-dependent parameters (such as DLCO), such ascertainment bias is, however, less likely.
A study in London identified a higher prevalence of SSc close to major airports.19 A high proportion of male patients was observed in Australia and was attributed to the inhalation of silica dust.20 Our study analysed by cluster analysis whether possible hidden risk factors could operate in modulating individual disease presentations, but failed to detect evidence of environmental exposure in definable geographical pockets. Our geographical grid was, however, very coarse in some countries and was also unlikely to represent a large proportion of the population in some countries and regions. It is therefore not possible to generalise our findings beyond this resolution.
Our data may also be influenced by differences in socioeconomic status between countries or regions. An Australian study, however, found no difference in socioeconomic disadvantage scores between dcSSc and lcSSc at disease onset and follow-up.21 Differences in socioeconomic status could nevertheless be linked to differences in the accessibility of the healthcare system and could explain some of the regional variability, for example the higher proportion of Scl70 in eastern centres. Accessibility to EUSTAR centres could also vary, if some centres served a more urban and others a more rural population. The latter may be expected to have a higher proportion of more severe cases. Such bias could explain many of the correlations and some of the clustering in fig 2, and could be overcome by a much more cumbersome analysis for residential longitude and latitude. A British study, in fact, examined the prevalence of SSc in an urban area (Newcastle city) and in outer, more rural areas, but did not detect differences in SSc prevalence between areas.22 In a rural area in the province of Rome, a higher than expected prevalence of scleroderma and related features was identified.19 A similar study conducted in Ontario (Canada) found a greater prevalence of SSc in the more rural Woodstock area (280 per million) than in two other towns of the region, Sarnia (96 per million) and Windsor (71 per million).14 All these studies, however, did not examine different disease presentations.
Our analysis thus suggests that eastern European centres care for SSc patients with more severe manifestations than seen in other centres. A large local variability of SSc manifestations within adjacent centres suggests a substantial referral bias and precludes the identification of genetic or environmental factors.
Acknowledgments
The authors would like to thank P Cerboni for data management, J Wendel (Basle University Department of Geography) for assistance with the geographical information system and M Enters (Statsolutions, Freiburg, Germany) for expert statistical assistance.
REFERENCES
Supplementary materials
Web Only Data 68;6:856-862
Files in this Data Supplement:
Footnotes
Competing interests: None.
Funding: EUSTAR is supported by a research grant from EULAR and is under the auspices of the Standing Committee for International Studies including Clinical Trials (ESCISIT).
Ethics approval: Ethics approval was obtained.
Patient consent: Obtained.
▸ The appendix is published online only at http://ard.bmj.com/content/vol68/issue6