Article Text

Abstract
Objectives: To assess the association of body mass index (BMI) with modifiable cardiovascular disease (CVD) risk factors in patients with rheumatoid arthritis (RA).
Methods: BMI, disease activity, selected CVD risk factors and CVD medication were assessed in 378 (276 women) patients with RA. Patients exceeding accepted thresholds in ⩾3 CVD risk factors were classified as having the metabolic syndrome (MetS).
Results: BMI independently associated with hypertension (OR = 1.28 (95% CI = 1.22 to 1.34); p = 0.001), high-density lipoprotein (OR = 1.10 (95% CI = 1.06 to 1.15); p = 0.025), insulin resistance (OR = 1.13 (95% CI = 1.08 to 1.18); p = 0.000) and MetS (OR = 1.15 (95% CI = 1.08 to 1.21); p = 0.000). In multivariable analyses, BMI had the strongest associations with CVD risk factors (F1–354 = 8.663, p = 0.000), and this was followed by lipid-lowering treatment (F1–354 = 7.651, p = 0.000), age (F1–354 = 7.541, p = 0.000), antihypertensive treatment (F1–354 = 4.997, p = 0.000) and gender (F1–354 = 4.707, p = 0.000). Prevalence of hypertension (p = 0.004), insulin resistance (p = 0.005) and MetS (p = 0.000) was significantly different between patients with RA who were normal, overweight and obese, and BMI differed significantly according to the number of risk factors present (p = 0.000).
Conclusions: Increasing BMI associates with increased CVD risk independently of many confounders. RA-specific BMI cut-off points better identify patients with RA at increased CVD risk. Weight-loss regimens should be developed and applied in order to reduce CVD in patients with RA.
Statistics from Altmetric.com
Rheumatoid arthritis (RA) associates with increased risk for cardiovascular disease (CVD).1 This is most likely a combination of genetic predisposition,2 modifiable CVD risk factors and the inflammatory burden of the disease.3 Patients with RA have a significantly higher body fat content compared with healthy individuals of the same height and weight.4 This led to the development of RA-specific body mass index (BMI) thresholds for overweight and obesity that better identify patients with RA with increased body fat,4 and possibly CVD risk.
In the general population, obesity is a major contributor to dyslipidaemia, hypertension and insulin resistance5 and the underlying cause of the metabolic syndrome (MetS).5 The associations between obesity and CVD risk factors or the MetS in RA have not been extensively investigated. Obesity in this population is usually considered a confounder, against which data should be standardised, but not as the possible underlying cause for several CVD risk factors. The aim of this study was to quantify the associations of BMI with classical CVD risk factors in a large sample of patients with RA.
METHODS
Participants
The study had ethical approval and all volunteers provided informed consent. A total of 400 (289 women) consecutive patients with RA were assessed; of these, none had uncontrolled thyroid disease, but 22 were excluded due to cancer. The analyses from the remaining 378 (276 women) patients are reported: their characteristics appear in table 1.
Assessments
Standing height, weight, BMI (kg/m2) and waist circumference were measured. CVD risk factors (blood pressure (BP), lipids) were assessed, smoking status noted and the Framingham 10-year CVD event probability was calculated. The Homeostasis Model Assessment of insulin resistance (HOMA) and the Quantitative Insulin sensitivity Check Index (QUICKI),were used to determine insulin resistance (IR). The NCEP ATP III criteria5 were used to identify patients with the MetS. Erythrocyte sedimentation rate, C-reactive protein, disease activity score (using 28 joint counts) (DAS28) and the Stanford Health Assessment Questionnaire (HAQ) were also assessed.
Data analysis
The Statistical Package for Social Sciences version 15.0 was used (SPSS Inc. Chicago, Illinois, USA). Dispersion of the variables was assessed using the Kolmogorov–Smirnov test. Spearman’s correlations explored the associations of CVD risk factors and 10-year CVD event probability with BMI. Results were standardised for gender, age, smoking status, RA characteristics and CVD medication using univariable analyses. Multivariable analyses were used to asses the overall association of each of the possible confounders with the CVD risk factors and the 10-year CVD event probability.
Following grouping according to RA-specific BMI4 in those who were underweight, normal weight, overweight and obese, analysis of variance (ANOVA) was used to assess differences in BP, lipids and IR between groups. Analysis of co-variance (ANCOVA) was then used to standardise for the same possible confounders as above. χ2 analyses were used to identify differences in the prevalence of each risk factor or the MetS between BMI groups. Binary logistic models were used to test the independence of these associations from the same possible confounders.
Finally, patients were grouped according to the total number of risk factors they had. ANOVA was used to assess differences in BMI among these latter groups and ANCOVA to adjust for the same possible confounders. Data are reported as median (interquartile range). Statistical significance was set to p<0.05.

RESULTS
Body mass index and cardiovascular disease risk factors
BMI correlated significantly with systolic BP (r = 0.240, p = 0.000), high-density lipoprotein (r = −183, p = 0.000), HOMA (r = 0.302, p = 0.000) and QUICKI (r = −0.300, p = 0.000). BMI also correlated with erythrocyte sedimentation rate (r = 0.128, p = 0.011), C-reactive protein (r = 0.155, p = 0.002) and HAQ (r = 0.133, p = 0.009); therefore, results were standardised for these parameters as well as for gender, age, smoking and CVD medication. BMI retained its association with systolic BP (F1–354 = 23,372, p = 0.000), high-density lipoprotein (F1–354 = 10.439, p = 0.001), HOMA (F1–354 = 11.311, p = 0.001) and QUICKI (F1–354 = 34.678, p = 0.000) and also associated with diastolic BP (F1–354 = 7,593, p = 0.006), triglycerides (F1–354 = 4.496, p = 0.035) and 10-year CVD event probability (F1–354 = 5.857, p = 0.016). Different multivariate models, using BP, lipids and IR as dependent variables, gender and smoking status as factors and BMI, age, RA characteristics and CVD medication as covariates indicated that the variance observed in all CVD risk factors was more closely associated with BMI (F1–354 = 8.663, p = 0.000), followed by lipid-lowering treatment (F1–354 = 7.651, p = 0.000), age (F1–354 = 7.541, p = 0.000), antihypertensive treatment (F1–354 = 4.997, p = 0.000) and male gender (F1–354 = 4.707, p = 0.000).
ANCOVA, with corrections for gender, age, smoking, RA characteristics and usage of CVD medication, showed significant differences between BMI subgroups (underweight, normal weight, overweight and obese) for systolic BP (F1–354 = 14.707, p = 0.000), diastolic BP (F1–354 = 6.457, p = 0.011), triglycerides (F1–354 = 4.700, p = 0.031), high-density lipoprotein (F1–354 = 7.545, p = 006), HOMA (F1–354 = 9.720, p = 0.002), QUICKI (F1–354 = 30.332, p = 0.000) and 10-year CVD event probability (F1–354 = 3.981, p = 0.046).
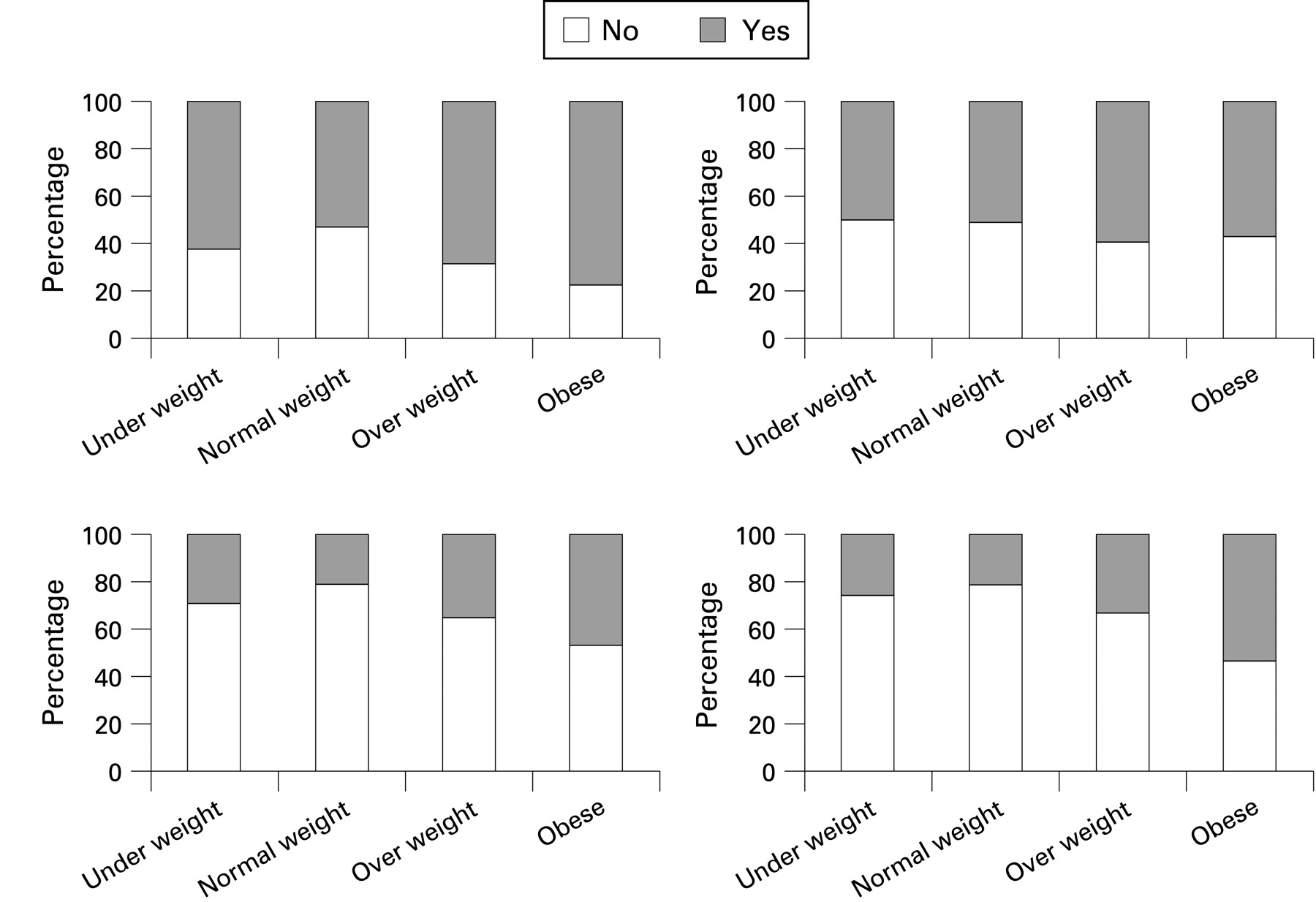
Body mass index subgroups and the prevalence of cardiovascular disease risk factors
Cross-tabulation of BMI subgroups with presence or absence of each risk factor or the MetS demonstrated significant differences between groups for the prevalence of hypertension (p = 0.004), insulin resistance (p = 0.005) and the MetS (p = 0.000) (fig 1). The binary logistic models indicated that BMI associated with hypertension (OR = 1.28, 95% CI = 1.22 to 1.34; p = 0.001), high-density lipoprotein (OR = 1.10, 95% CI: 1.06 to 1.15; p = 0.025), IR (OR = 1.13, 95% CI = 1.08 to 1.18; p = 0.000) and the MetS (OR = 1.15, 95% CI: 1.08 to 1.21; p = 0.000) independently of confounding factors.

{kind=link}
{kind=link}
Following grouping for the total number of risk factors present, ANOVA showed significant differences in BMI between groups (p = 0.000; table 1), while ANCOVA revealed that this association was independent of gender, age, smoking, RA characteristics and use of CVD medication (p = 0.000).
DISCUSSION
These results suggest an almost linear relationship between BMI and CVD risk in this patient group, with the risk profile worsening as BMI increases, in a pattern similar to that described in the general population.5 These associations were independent of multiple confounders, and if anything, they became stronger following inclusion of CVD medication in the models. It must be emphasised that these are all cross-sectional associations, and they do not provide definitive evidence for causality or directionality: longitudinal studies are required for this.
There is no reason to suggest that the mechanisms by which obesity increases CVD risk in RA are different from those in the general population. Excess adipose tissue releases non-esterified fatty acids in the circulation, which overload the liver and muscles with lipids and increase lipolysis, while reducing glucose utilisation. Circulating glucose stimulates insulin production, leading to insulin resistance.6 Endothelial function is often impaired causing arterial stiffness and hypertension.7 Obesity may also increase CVD risk by reducing adiponectin, activating the rennin–angiotensin–aldosterone system, and increasing sympathetic activity and renal sodium reabsorption.6 However, as we did not measure any of these parameters we can only postulate about their contribution to our observations.
Recent studies in RA have shown no relation8 or even a “paradoxical” protective effect of obesity against CVD,9 although no potential mechanisms were described. In our study, lipid-lowering and antihypertensive drugs strongly associated with CVD risk factors; their inclusion in the models strengthened the association of BMI with all risk factors assessed. Such drugs, known to improve CVD risk and reduce mortality, are more frequently prescribed in obese than in non-obese individuals.10 Thus their inclusion in the analyses of studies investigating CVD risk and outcome in RA is of paramount importance.
In the present study, neither disease characteristics nor smoking affected the associations of BMI with CVD risk. This finding is similar to our previous observations indicating that alterations in body composition of patients with RA occur in the early years of the disease4 or even prior to it. This could be the case for some CVD risk factors as “the risk of coronary heart disease in RA patients precedes the ACR criteria-based diagnosis of RA”.11 Similarly, smoking appears to confer less CVD risk in RA than in the general population.3 Most likely, this is the result of the smoking-induced weight-loss we recently described in RA,12 which may counteract the known negative effects of smoking on risk factors. However, disease characteristics and smoking were treated solely as possible confounders, thus their direct associations with CVD risk in RA cannot be assessed in this study.
An important finding of the present study is the BMI level at which CVD risk increases. Patients with one risk factor had a median BMI of <25 kg/m2, whereas those with MetS <30 kg/m2 and by applying general BMI thresholds would be classified as normal weight and overweight respectively; however, based on RA-specific BMI thresholds they would be classified as overweight or obese. This could be important in routine clinical practice, where such classifications may be used to target patients at increased risk for screening, early identification and management of risk factors.
In the general population, weight loss can reverse the adverse effects of obesity. However, in a population with significant muscle wasting, such as RA, the type of weight-loss intervention has to be carefully considered. Among existing weight-loss regimens, exercise and especially resistance training, is the only one proven to increase muscle mass in the general population13 and may be applied in patients with RA without aggravating their disease.14 Moreover, exercise is known to further reduce CVD risk irrespective of weight loss.15 Research focusing on weight-loss interventions and their effects on CVD in RA are necessary.
Within its limitations, this study shows that increasing BMI in patients with RA associates with increased CVD risk. The use of RA-specific BMI thresholds better identifies patients with RA at increased CVD risk. Weight-loss regimens specific for patients with RA need to be developed and evaluated.
Acknowledgments
This study was funded by the Dudley Group of Hospitals R&D directorate cardiovascular programme grant and a Wolverhampton University equipment grant. The Department of Rheumatology has an infrastructure support grant from the Arthritis Research Campaign (no. 17682).
REFERENCES
Footnotes
Competing interests: None.