Article Text

Abstract
Objective: To determine if treatment with a B cell-targeted therapy can inhibit the progression of structural joint damage in patients with rheumatoid arthritis (RA), exhibiting an inadequate response to tumour necrosis factor (TNF) inhibitors.
Methods: In this phase III study, patients with an inadequate response to a TNF inhibitor and receiving methotrexate were randomised to rituximab or placebo. Radiographs were obtained at baseline, week 24 and week 56 after randomisation. Patients with an inadequate response to their randomised therapy could receive rescue medication from week 16. From week 24, eligible patients from both treatment arms could receive open-label rituximab. Patients were analysed according to their original treatment group. Radiographs were scored using the Genant-modified Sharp method. The primary radiographic endpoint was change in total Genant-modified Sharp score at week 56.
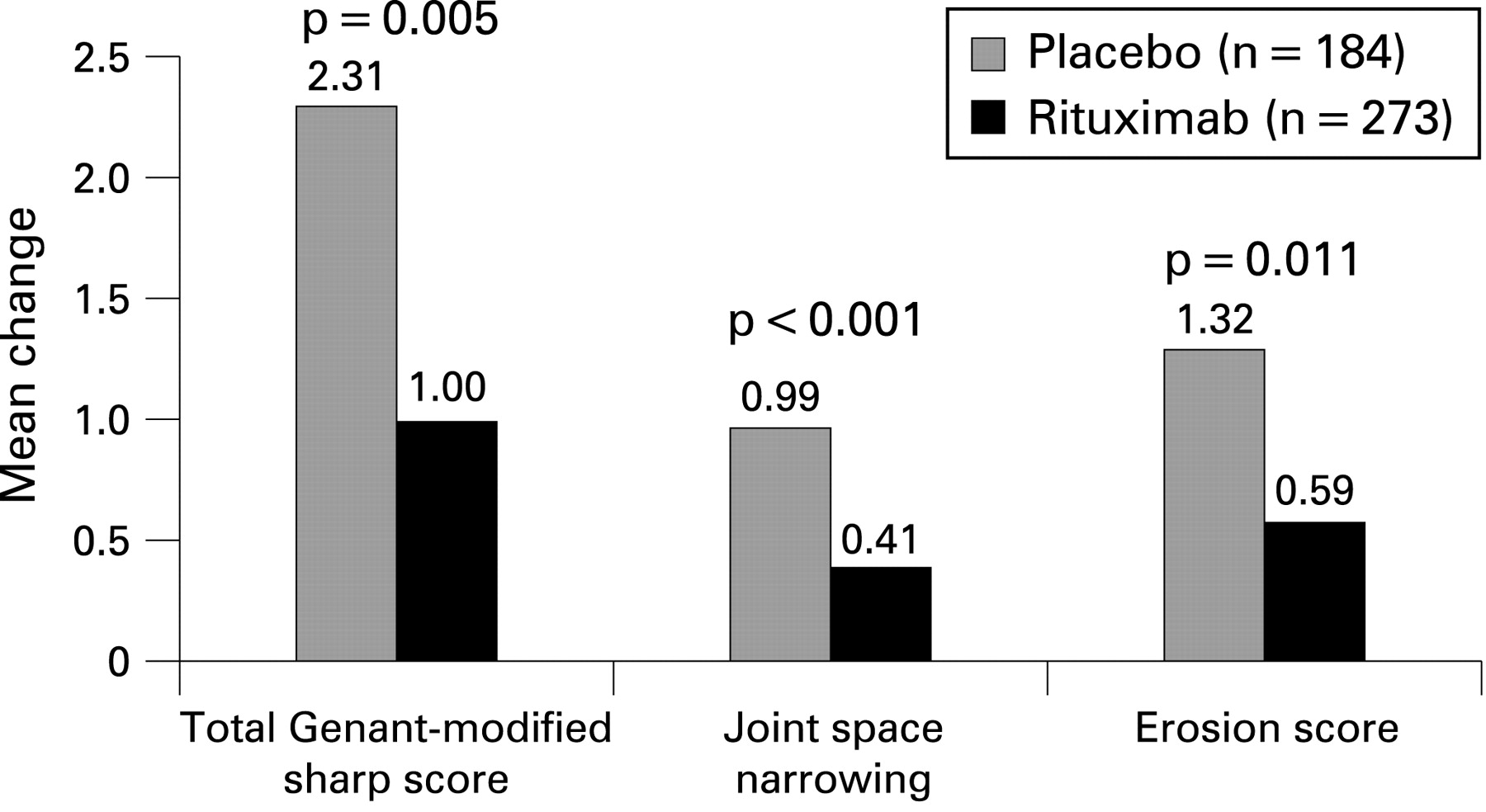
Results: Rituximab treatment caused significant reduction in joint damage progression compared with placebo. The mean change from baseline in the total Genant-modified Sharp score at week 56 was significantly lower for patients treated with rituximab than for patients treated with placebo (1.00 vs 2.31; p = 0.005), and was supported by changes in erosion score (0.59 and 1.32 for rituximab plus methotrexate vs placebo plus methotrexate, respectively; p = 0.011) and joint space narrowing score (0.41 and 0.99, respectively; p<0.001).
Conclusions: This study provides the first evidence that a B cell-targeted therapy—rituximab—can significantly inhibit the progression of structural joint damage in patients with RA with long-standing, active and treatment-resistant disease.
Statistics from Altmetric.com
Rheumatoid arthritis (RA) is a chronic systemic autoimmune disease that causes significant disability1 2 through irreversible joint destruction. The goals of RA treatment are to alleviate signs and symptoms, preserve joint structure and function, improve quality of life and prevent disability. Structural joint damage is detectable early in the course of the disease3 4 and over time causes disability in a significant proportion of patients.5 Over the past 10 years, new therapies, particularly those inhibiting tumour necrosis factor (TNF), have provided substantially improved efficacy compared with what was previously achievable. Nevertheless, approximately 20–40% of patients treated with a TNF inhibitor fail to achieve an adequate response, have a secondary loss of response, or are intolerant to these agents.6 7 Furthermore, no biological RA therapy has been proven to retard or inhibit joint damage in this important patient population.
Rituximab is a monoclonal antibody that selectively targets CD20-positive B cells.8 Rituximab was recently approved for the treatment of patients with active RA who have had an inadequate response or intolerance to TNF inhibitor therapies on the basis of several randomised placebo-controlled studies.9–11 Preliminary 6-month data from a phase III study suggested early trends of inhibition of the progression of joint damage,10 however longer term follow-up of these patients is necessary.
METHODS
Patients
The patients included in this analysis were drawn from those recruited into the “Randomised Evaluation oF Long-term Efficacy of rituXimab in RA” (REFLEX) phase III study. Patients were recruited from 114 rheumatology centres in the USA, Europe, Canada and Israel. Eligibility criteria for REFLEX have been previously published;10 briefly, patients were at least 18 years of age and had been diagnosed with RA for at least 6 months, according to the American College of Rheumatology (ACR) 1987 revised criteria,12 with active disease despite treatment with methotrexate ⩾10 mg/week. Active disease was defined by the presence of at least eight tender (68 joint count) and eight swollen joints (66 joint count) and a serum C-reactive protein (CRP) level of ⩾15 mg/litre or an erythrocyte sedimentation rate (ESR) of ⩾28 mm/h. Enrolled patients had experienced an inadequate response (lack of efficacy or intolerance) to previous or current treatment with at least one TNF inhibitor. Withdrawal of TNF inhibitor treatment for reasons of intolerance was at the treating physician’s discretion, whereas withdrawal of TNF inhibitor treatment for reasons of lack of efficacy required minimum treatment periods (at least 3 months of treatment of adalimumab at 40 mg every other week, at least 3 months of treatment of etanercept at 25 mg twice weekly or at least four infusions of infliximab of a minimum dose of 3 mg/kg). All patients had at least one joint erosion attributable to RA. Continued, stable glucocorticoid (⩽10 mg/day of prednisone or equivalent) and non-steroidal anti-inflammatory drug use was allowed. Concurrent treatment with any disease-modifying antirheumatic drug (DMARD) other than methotrexate, or TNF inhibitor therapy, was prohibited during the study.
The study was performed in accordance with the Declaration of Helsinki. All participating sites received approval from their governing institutional review board (or equivalent) and all patients provided written informed consent.
Study protocol
REFLEX was a 2-year, randomised, double-blind, placebo-controlled, phase III study. Patients continued background methotrexate and were randomly assigned to placebo or rituximab (MabThera, Roche, Welwyn Garden City, UK; Rituxan, Genentech and Biogen Idec, Inc. San Diego, California, USA). Rituximab was administered as a 1000 mg intravenous infusion on days 1 and 15 (fig 1). Both groups received 100 mg of methylprednisolone intravenously 30 min before each infusion of rituximab/placebo, and 60 mg/day of oral prednisone on days 2–7 and 30 mg/day on days 8–14. All patients also received folate at a dose of ⩾5 mg/week or equivalent.

The primary efficacy (20% improvement according to ACR criteria; ACR20) and safety endpoints were evaluated at 24 weeks. Beyond week 24, patients continued to be followed every 2 months for an overall study duration of 24 months.
From weeks 16 to 24, patients who had failed to respond to treatment (<20% improvement in swollen joint counts) could receive rescue therapy. Patients randomised to placebo could receive rituximab, whereas patients randomised to rituximab could receive standard of care.
Patients completing week 24 who had some response to treatment (defined as a reduction in swollen and tender joint counts of ⩾20%), but who had more than eight swollen and tender joints and had no contraindications to receiving rituximab, could receive further courses of rituximab within an open-label extension study (fig 1). Further courses of rituximab were also available for placebo patients who had responded to rescue treatment with rituximab.
Patients withdrawing from either the randomised study or the extension study entered a safety follow-up period and were followed for at least 48 weeks from the point of withdrawal. After withdrawal, patients could receive any additional therapy (including TNF inhibitors) as required.
Radiographs of the hands, wrists (posterior/anterior) and feet (anterior/posterior) were performed at screening (baseline), week 24 and week 56. Radiographs were taken at times relative to initial randomisation and included patients who had withdrawn into safety follow-up. Radiographs were read at a central reading facility by two independent expert radiologists and scored using the Genant-modified Sharp scoring system,13–17 which quantifies articular erosions and joint space narrowing (JSN). The total score is the sum of the erosion and JSN scores. Radiologists were blinded to the treatment group assignment, chronological order of the radiographs and patients’ clinical response.
Radiographic outcome measures
The primary radiographic endpoint was the mean change in total Genant-modified Sharp score (TSG) between screening and week 56. Secondary radiographic endpoints included the erosion score, the JSN score and the proportion of patients with no further erosive damage (defined as a change in erosion score of zero or lower).
Statistical analysis
The primary population for the radiographic analysis was a subset of the intention-to-treat (ITT) population (hereafter designated as the radiographic ITT subset), defined as all patients randomised who received at least a part of the first treatment (any part of two study infusions), and for whom at least one post-baseline radiograph (either 24 weeks or 56 weeks) was available. For the primary radiographic analysis, the week-56 radiograph was only included if it fell within a specific time window (days 350 to 434). All missing data (including radiographs outside this window) were imputed using linear extrapolation (LE) of the progression observed from screening/baseline to the week-24 radiographs (if available). As changes in radiographic outcomes are known to be skewed, primary analyses were conducted using a nonparametric analysis (Van Elteren test), stratifying by region (US/non-US) and baseline rheumatoid factor (positive/negative). Cumulative distribution plots were also produced to show individual patient progression. Several sensitivity analyses were also conducted, repeating these analyses in different populations and accounting for missing data using alternative imputation assumptions.
RESULTS
Patient characteristics and disposition
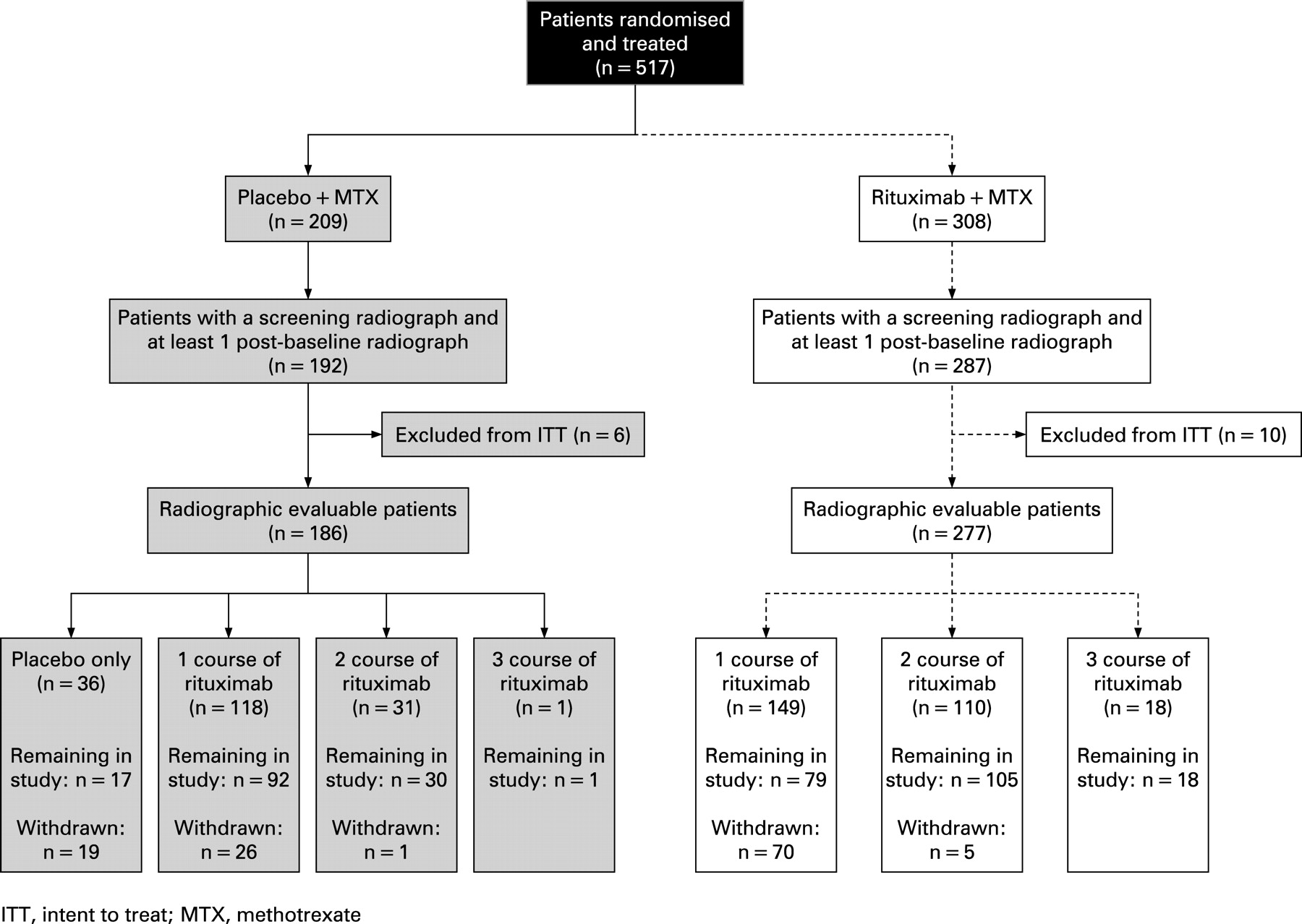
A total of 517 patients were randomised in a 3:2 ratio and treated with rituximab plus methotrexate (n = 308) or placebo plus methotrexate (n = 209). Of these, 479 patients (287 patients on rituximab and 192 patients on placebo) had a screening and at least one post-baseline radiograph. A total of 16 patients were excluded from the efficacy analysis because of major protocol violations, including unblinding because of rituximab vial breakage, treatment of patients before randomisation, or enrolment of patients at a centre where efficacy assessor blinding was potentially compromised. Therefore, the radiographic ITT subset population comprised 186 patients from the placebo plus methotrexate arm and 277 patients from the rituximab plus methotrexate arm (463 patients in total) (fig 2).

The baseline characteristics and measures of disease activity were similar in both treatment groups (table 1) and were consistent with long-standing, highly active and treatment-resistant disease.
At week 56, a total of 75/277 patients (27%) randomised to rituximab had withdrawn into the safety follow-up; 29 of these patients (10.5%) received subsequent treatment with a TNF inhibitor. A total of 128 patients (46%) had received further courses of rituximab (fig 2). A total of 149 patients (54%) had received a single course of rituximab, 110 patients (40%) had received two courses, and 18 patients (7%) had received three courses.
At week 56, 150/186 patients (81%) randomised to placebo had received at least one dose of rituximab. Of these, 118 patients (63%) received a single course, 31 patients (17%) received two courses, and 1 patient (<1%) received three courses of rituximab. Only 36 patients (19%) initially randomised to placebo had still not received rituximab by week 56. A total of 46 patients (25%) initially randomised to placebo withdrew and entered safety follow-up; 12 of these patients (6.5%) received subsequent treatment with a TNF inhibitor.
Radiographic efficacy
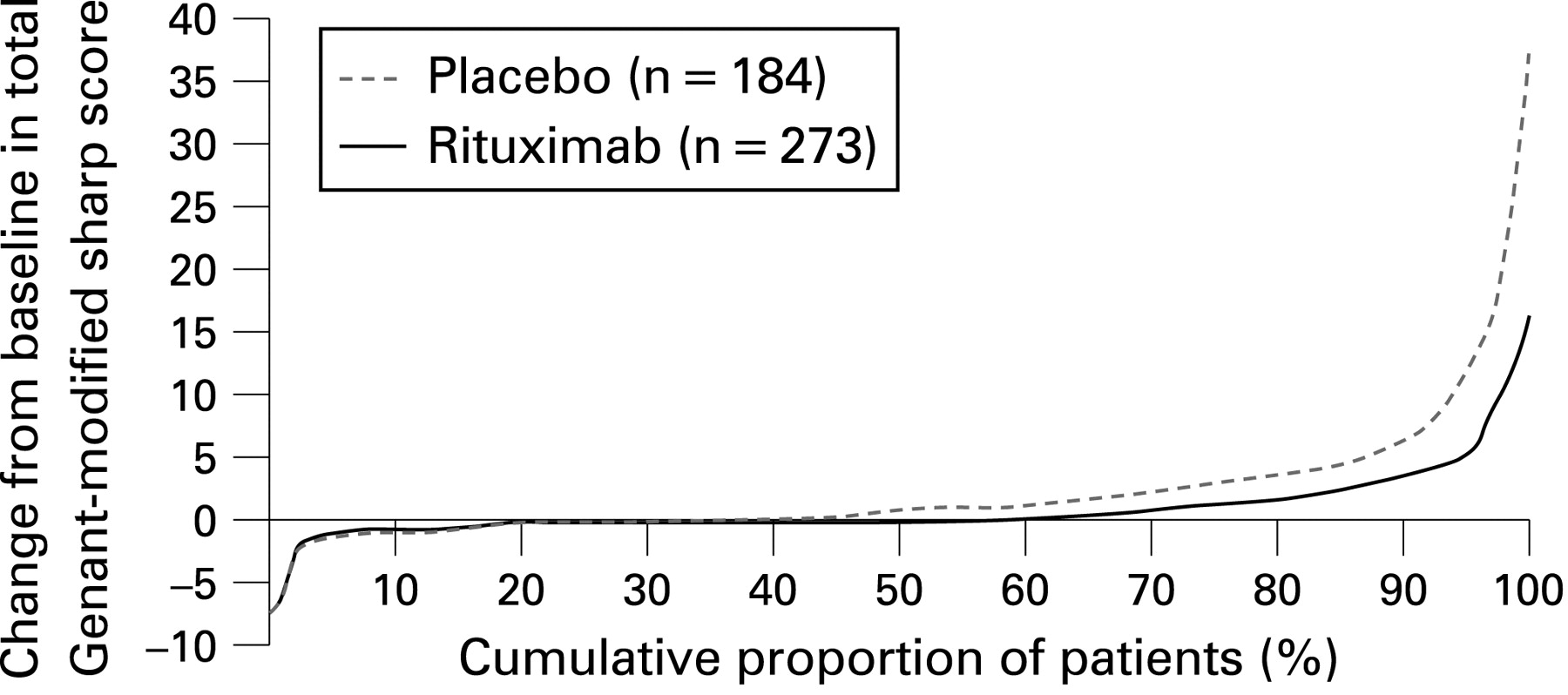
The primary radiographic outcome (mean change in the total Genant-modified Sharp score at week 56) as determined for the radiographic ITT subset was significantly lower for patients randomised to rituximab plus methotrexate than for patients who were randomised to placebo plus methotrexate (1.00 vs 2.31; p = 0.005) (fig 3). The inhibitory effect of rituximab therapy upon structural damage progression was also evident when erosions and joint space narrowing were assessed. At week 56, the mean changes from baseline in the erosion score (0.59 vs 1.32; p = 0.011) (fig 3) and JSN score (0.41 vs 0.99; p<0.001) (fig 3) were also significantly lower for patients randomised to rituximab plus methotrexate than for patients randomised to placebo plus methotrexate. The cumulative distribution plot of the change from baseline in the total Genant-modified Sharp score also supported the observation that a smaller proportion of patients receiving rituximab plus methotrexate had progression of joint damage and that the degree of progression in this group was substantially lower compared to the MTX plus placebo group (fig 4).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Additional analyses further substantiated the effect of rituximab treatment upon structural damage progression. The proportion of patients with no erosive progression between baseline and week 56 was significantly greater in the rituximab plus methotrexate group than in the placebo plus methotrexate group (61% vs 52%; p = 0.049). The proportion of patients with no change from baseline in their total Genant-modified Sharp score was numerically greater in the rituximab plus methotrexate group compared with the placebo plus methotrexate group (53% vs 46%, respectively), but did not reach statistical significance (p = 0.090).
Additional sensitivity analyses were conducted to assess the potential impact of missing data including assessments using the full primary ITT analysis population,10 irrespective of whether or not a post-baseline radiograph had been obtained or whether the week 56 x ray was obtained within the pre-specified visit window. These analyses were highly consistent with the primary analysis, with all showing statistical significance in favour of rituximab plus methotrexate (see table 2, web only). Sensitivity analyses that were strongly biased in favour of the patients on placebo, imputed third-quartile changes for missing data in the rituximab group and first-quartile changes for missing data in the placebo group showed a numerical difference in favour of rituximab, although a statistical difference was not achieved.
Patients who withdrew into safety follow-up were permitted to receive any RA therapy that was required, including biologicals. It was therefore important to determine if this additional treatment had influenced radiographic outcomes in any way. The most conservative analysis retained patients randomised to placebo who received subsequent treatment with another biological agent, while excluding those patients on rituximab who subsequently received a biological therapy. The outcome of this analysis found that, despite a bias that favoured the placebo group, treatment with rituximab was still strongly associated with inhibition of structural damage progression (change in total Sharp score of 2.31 vs 0.88; p = 0.0021).
Furthermore, the mean change in total Genant-modified Sharp score observed in the placebo group did not appear to be influenced by greater progression in those patients who had received placebo alone throughout the 56-week period; mean change in this subgroup was 1.99 compared with a mean change of 2.31 for the placebo group as a whole.
The robustness and consistency of the inhibitory effect of rituximab treatment upon structural damage progression was further demonstrated in subgroup analyses based on quartiles of baseline disease characteristics. Such parameters included baseline 28-joint Disease Activity Score (DAS28), CRP, Health Assessment Questionnaire Disability Index (HAQ), disease duration and total Genant-modified Sharp score. As the study was not powered to assess efficacy in these subgroups, not statistical analyses were conducted; nevertheless, strong trends supportive of the primary analysis were observed (table 3). Retardation of progression of structural damage was also observed in the population of patients who were RF negative at baseline (mean change in total score 3.30 vs 1.10 for placebo and rituximab groups, respectively).
DISCUSSION
The primary objective of the REFLEX study was to assess the efficacy and safety of rituximab in patients with active, erosive disease that had not been successfully treated with TNF inhibitor therapies and therefore required treatment with an alternative therapy. While two recent studies have now demonstrated that control of disease symptoms in these patients is achievable,10 18 the ability to inhibit further joint damage in these patients has remained unstudied.
The primary radiographic endpoint in the current study (mean change from baseline in the total Genant-modified Sharp score) at week 56 demonstrated that treatment with rituximab resulted in statistically significant inhibition of joint damage. This finding was supported by significantly less progression for erosion and JSN scores. Multiple sensitivity analyses that assessed the potential impact of missing data as well as subgroups based on clinically important baseline characteristics also supported the primary analyses, with many continuing to show statistically significant differences in favour of the rituximab group.
Cumulative distribution analysis also showed that the proportion of patients who progressed and the degree of progression in these patients was substantially lower with rituximab treatment. This was supported by the observation that significantly lower proportions of patients displayed erosive progression in the rituximab group compared with the placebo group and that retardation of joint damage was observed in clinically important subgroups, including patients with high DAS and high CRP levels, as well as in patients who were RF negative.
These data therefore demonstrate the significant and consistent benefit of treatment with rituximab plus methotrexate, compared with continued methotrexate therapy, on all indicators of progressive joint damage.
The use of placebo controls in studies of patients with active RA requires that access to active therapies be made available. Consequently, the design of the REFLEX study incorporated a rescue option whereby patients on placebo plus methotrexate withdrawing owing to lack of response could receive treatment with rituximab, and an open-label extension was carried out in which patients who completed 24 weeks of the study could potentially receive rituximab. By week 56, a high proportion (81%) of patients initially randomised to placebo plus methotrexate had received at least one course of rituximab. The study also permitted patients treated with rituximab to receive further courses of rituximab treatment.
A potential impact of this switch of patients treated with placebo to rituximab would be to slow progression in the placebo group and narrow treatment differences between the two study arms. In a review of randomised placebo-controlled studies, the observed yearly progression in the placebo groups was shown to approximate to—or exceeded—the estimated yearly progression.17 19 However, in studies where patients in the control group were permitted access to active medications (as in this study), the observed rate of progression for placebo was lower than the corresponding estimated yearly rate. This suggests that the influence of switching to active treatment in the REFLEX study may well have reduced the progression of the placebo group and consequently reduced the true difference between the two study arms.
Patients on rituximab were required to have responded to treatment and later flared (defined as eight or more swollen and tender joints) before further treatment courses could be given. As higher disease activity correlates with greater progression of joint damage, the requirement for a flare before repeat treatment may have accentuated radiographic progression. This concept is supported by a recent study showing that radiographic progression is significantly increased in patients with periodic flares compared with those with sustained disease control.20
A potential confounding factor is that patients who withdrew into safety follow-up were allowed to receive other RA therapies as clinically required, including TNF inhibitor therapies. Importantly, sensitivity analyses showed that this did not influence the study conclusions. Similarly, glucocorticoids are known to influence joint damage progression.21 Glucocorticoids were used as premedication prior to infusions in this study; however, as this was the case for all infusions (including placebo), exposure to glucocorticoids was balanced between the treatment arms and therefore was unlikely to have influenced the study outcomes.
In conclusion, this study provides the first evidence that a B cell-targeted therapy, rituximab, inhibits the progression of structural joint damage in RA. These data also show for the first time that, in patients with RA with long-standing, active disease inadequately controlled by prior biologic therapy, inhibition of progressive joint damage is an achievable therapeutic goal.
Acknowledgments
The authors wish to thank the REFLEX study group principal investigators: Drs J Alloway, C Appleboom, E Arthur, A Ashafzadeh, A Baldassare, J Bathon, G Bayliss, M Bell, S Berney, M Bingham, K Blocka, E Boling, S Bombardieri, R Brasington, B Bresnihan, S Bruno, G Burmester, H Busch, G Butler, M Carrabba, D Caspi, A Chubick, A Cividino, W Clair, C Codding, S Cohen, J Condemi, S Cooper, J Cush, S De Vita, J Devogelaer, R Digiovanni, J Donohue, A Dooley, M Dougados, D Doyle, M Ellman, P Emery, M Fairfax, G Ferraccioli, J Fiechtner, R Fife, J Forstot, P Freeman, E Fung, R Furie, M Genovese, R Gorla, M Greenwald, D Halter, J Isaacs, C Jackson, A Kaell, R Katz, C Kaufmann, A Kavanaugh, E Keystone, J Kim, J Kremer, T Kvien, P Langevitz, X Le Loet, M Liam, J Loveless, C Lue, M Luggen, D MacCarter, W Maksymowych, E Malaise, D Malone, D Mandel, X Mariette, A Martin, E Matteson, B Mazieres, F McKenna, P Mease, K Mikkelsen, K Miller, Y Molad, J Molitor, M Molloy, L Moreland, F Murphy, M Nahir, S Newell, D Noritake, H Nuesslein, R Pappu, E Peters, J Pope, E Quaidoo, T Riise, I Rosner, A Rubinow, E Ruderman, C Saadeh, J Sany, P Saxe, F Scott, T Sheeran, Y Sherrer, J Sibilia, D Smith, D Stahl, J Sundy, J Taborn, P Tak, H.P Tony, J Udell, A Uknis, M Veys, D Wallace, S Wassenberg, C Wiesenhutter, W Wilke, S Wolfe, D Yocum. The study was co-sponsored by F Hoffmann-La Roche Ltd. and Biogen Idec, Inc., who were responsible for data collection. Statistical analyses were conducted by qualified statisticians who were employees of the sponsors. All the authors had access to—and involvement in—the interpretation of the data and input into and control over the content of this manuscript (supervised by EK).
REFERENCES
Footnotes
Competing interests: EK has received consulting and speaker fees from Roche and Genentech and research grants from Roche. PE, PPT, GRB and TKK have received consulting and speaker fees and research grants from Roche. MCG has received speaker fees and research grant support from Roche and has served as a consultant for Roche, Biogen Idec and Genentech. MG has received research funds and consultancy fees from Biogen Idec, Genentech and Roche. DH and MWC are employees of Biogen Idec. SW and TS are employees and own shares in Roche Products Ltd. CGP, SC and MD have not declared any competing interests.
Funding: This study was sponsored by F Hoffmann-La Roche Ltd. and Biogen Idec, Inc. A portion of this work (Stanford University) was supported in part by a grant (5 M01 RR000070) from the National Center for Research Resources, National Institutes of Health. The authors are also grateful to the following from Roche Products Ltd: F Magrini, P Lehane, S Safa-Leathers, J Kalsi, A Donohoe, J Smith, K Rowe and B Mistry and the following from Biogen Idec: T Kheoh, K Gilder, J-W Wan, J Torrington and M Weaver.
Ethics approval: The study was performed in accordance with the Declaration of Helsinki. All participating sites received approval from their governing institutional review board (or equivalent) and all patients provided written informed consent.
Linked Articles
- Miscellaneous