Article Text

Abstract
Objectives: To evaluate the relationship between bone mineral density (BMD) and biomarkers of bone turnover and inflammation in patients with ankylosing spondylitis (AS) treated with infliximab.
Methods: Patients (n = 279) were randomly assigned (3:8) to receive placebo or 5 mg/kg infliximab every 6 weeks through week 96. At week 24, placebo-treated patients crossed over to infliximab 5 mg/kg. Starting at week 36, patients treated with infliximab received dose escalations to 7.5 mg/kg. Hip and spine BMD were measured (baseline, week 24, week 102) using dual-energy x-ray absorptiometry. Sera were analysed (baseline, week 24, week 102) for levels of bone alkaline phosphatase (BAP), osteocalcin, C-terminal cross-linking telopeptide of type I collagen (CTX), interleukin-6 (IL-6), vascular endothelial growth factor (VEGF) and transforming growth factor-β.
Results: Patients treated with infliximab showed significantly greater median increases in BMD of the spine (2.5%, p<0.001) and hip (0.5%, p = 0.033) at week 24 than those who received placebo (0.5% and 0.2% respectively). Baseline levels of IL-6, VEGF, osteocalcin, BAP and CTX were significantly correlated with increases in spinal BMD at weeks 24 and 102 in the infliximab group. In a multiple regression analysis, high baseline osteocalcin levels and early increases in BAP at week 2 were significantly associated with increases in BMD scores of the spine (week 102) and hip (weeks 24 and 102) in the infliximab group.
Conclusions: Patients with AS who received infliximab showed significant increases in BMD scores over 2 years. While many significant correlations were observed between BMD scores of the hip and spine and biomarker levels, high baseline osteocalcin levels and early increases in BAP were consistently associated with increases in BMD scores.
Statistics from Altmetric.com
Bone formation and bone resorption, such as syndesmophytes, ankylosis and erosions, are features of progressive ankylosing spondylitis (AS). However, studies of biochemical markers of bone turnover in patients with AS have yielded conflicting results. Some studies show normal1 2 or low3 4 levels of bone formation markers, such as osteocalcin or bone alkaline phosphatase (BAP), while other studies show elevated levels of these biomarkers.5 Studies examining markers of bone resorption (eg, pyridinium cross-linking telopeptide of type I collagen) in patients with AS also yield conflicting results.1 6–9 However, elevated levels of bone resorption markers have been shown to correlate with inflammatory markers and higher levels of acute-phase reactants in patients with AS1 as well as with inflammatory markers in patients with osteoporosis.10
In this study, we evaluated changes in the levels of markers associated with bone turnover and inflammation in patients with AS who received infliximab in the Ankylosing Spondylitis Study for the Evaluation of Recombinant Infliximab Therapy (ASSERT). We also determined the relationship between baseline levels and changes in these markers and increases in bone mineral density (BMD) after initiation of infliximab therapy. We hypothesise that changes in these biochemical markers after treatment with infliximab would be associated with an improvement in the disease processes corresponding with reduced inflammation and increased bone growth.
METHODS
Details of the ASSERT study have been previously published.11 12 Briefly, patients with AS for at least 3 months before screening were randomly assigned (3:8) to infusions of placebo or 5 mg/kg infliximab at weeks 0, 2, 6, 12 and 18. At week 24, patients assigned to placebo crossed over to 5 mg/kg infliximab, and both groups continued treatment every 6 weeks through week 96. Patients originally assigned to infliximab could receive dose escalations up to 7.5 mg/kg starting at week 36 if their Bath Ankylosing Spondylitis Disease Activity Index score was at least 3 for two consecutive visits.
Sera from patients were collected for biomarker testing at weeks 0, 2, 24 and 102. BAP (Quidel, San Diego, California, USA), osteocalcin (Nordic Biosciences, Herlev, Denmark), and C-terminal cross-linking telopeptide of type I collagen (CTX) (Nordic Biosciences) were evaluated as markers of bone turnover. Interleukin-6 (IL-6), vascular endothelial growth factor (VEGF), and transforming growth factor-β (TGF-β) were evaluated as markers of inflammation (R&D Systems, Minneapolis, USA).
The BMD of patients aged 20–84 (n = 276) was measured by dual-energy x-ray absorptiometry (DEXA) evaluations of the hip and spine (L1–L4) at baseline, week 24 and week 102. Vertebrae exhibiting abnormalities (eg, fracture or surgical alteration) were excluded from BMD analysis. Osteopenia was defined as a T score between −2.5 and −1, exclusive. Osteoporosis was defined as a T score of −2.5 or lower.
The presence of syndesmophytes was determined using radiography at baseline and week 102.13 Briefly, lateral radiographs of the cervical and lumbar spine were scored using the modified Stoke Ankylosing Spondylitis Spine Score (mSASSS).14 15 The anterior sites of the lower and upper portion of each vertebra were scored from the T12 lower border to the S1 upper border for the lumbar spine and from the C2 lower border to the T1 upper border for the cervical spine. Each of the 24 regions was assigned a score of 0 (normal), 1 (erosion, sclerosis, or squaring), 2 (syndesmophyte) or 3 (bridging syndesmophyte). Syndesmophytes were defined as regional scores of 2 or greater. A patient who had a vertebral region score less than 2 at baseline and greater than or equal to 2 at week 102 was considered to have developed a syndesmophyte.
Statistical analyses
This study is post hoc and exploratory; therefore, the statistics are descriptive only and are not adjusted for multiplicity. Changes from baseline to weeks 2 and 24 in biomarker levels and changes from baseline to week 24 in BMD scores, T scores and Z scores of the hip and spine were evaluated using an analysis of variance on the van der Waerden normal scores. Univariate correlations between individual biomarkers (at baseline and week 24) and between biomarker levels (at baseline and per cent change from baseline to weeks 2 and 24) and changes from baseline to weeks 24 and 102 in spinal and hip BMD scores were determined using Spearman’s ranking correlation coefficient. Multiple linear regression analyses were performed using baseline and change from baseline to week 2 in biomarker levels (IL-6, VEGF, BAP, osteocalcin and TGF-β), syndesmophyte development (from baseline to week 102), and change from baseline to weeks 24 and 102 in BMD scores (hip and spine) to determine whether serum biomarker levels or syndesmophyte development were significantly associated with increases in BMD scores of the spine or hip. Box plots were used to depict the actual and per cent changes from baseline in BMD and actual change from baseline in T scores at weeks 24 and 102. Statistical analyses were performed using the SAS system (SAS Institute, Cary, North Carolina, USA).
RESULTS
Baseline patient characteristics were comparable between treatment groups (table 1).
Correlations between biomarker levels
Spearman correlation coefficients (r) among biomarker levels at baseline and week 24 are summarised in table 2.
At baseline, the strongest relationship was observed between the markers of bone turnover osteocalcin and CTX (r = 0.476, p<0.0001). Significant but modest correlations were observed between the markers of bone formation BAP and osteocalcin (r = 0.336, p<0.0001) and between BAP and CTX (r = 0.367, p<0.0001). Significant but modest correlations among inflammatory markers were observed between IL-6 and VEGF (r = 0.264, p<0.0001) and between VEGF and TGF-β (r = 0.256, p<0.0001).
At week 24 in the infliximab group, the strongest correlations were observed between IL-6 and VEGF (r = 0.446, p<0.0001) and between VEGF and TGF-β (r = 0.494, p<0.0001). Modest correlations were observed between BAP and osteocalcin (r = 0.391, p<0.0001), IL-6 and osteocalcin (r = −0.268, p<0.005), VEGF and osteocalcin (r = −0.288, p<0.005), and CTX and osteocalcin (r = 0.273, p<0.005). In the placebo group at week 24, significant correlations were observed between TGF-β and VEGF (r = 0.564, p<0.0001), and modest correlations were observed between osteocalcin and CTX (r = 0.259, p<0.05) and between osteocalcin and BAP (r = 0.274, p<0.05).
Changes in biomarker levels following infliximab treatment
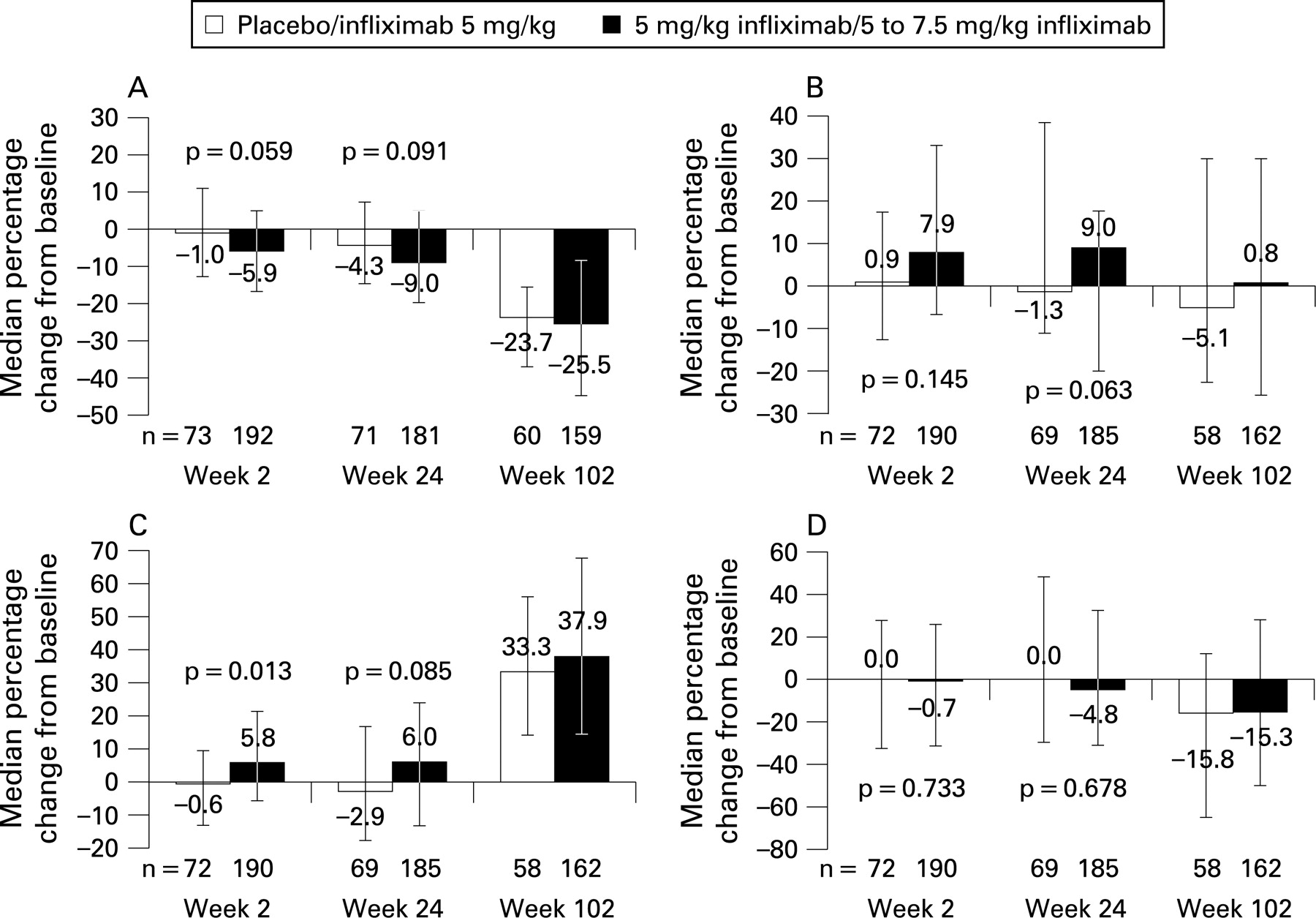
Percentage changes in biomarker levels from baseline to weeks 2, 24 and 102 are shown in fig 1. A significantly greater median per cent increase in BAP was observed in the infliximab group at week 2 (5.8%) compared with the placebo group (−0.6%, p = 0.013). The median per cent increase in BAP from baseline to week 24 in the infliximab group was similar to the value at week 2 (6.0%), but greater variability was observed in both the infliximab and placebo groups, and the difference between groups was not significant (p = 0.085). Trends toward a greater increase in osteocalcin at week 24 (p = 0.063) and a greater reduction in TGF-β at weeks 2 (p = 0.059) and 24 (p = 0.091) were observed among patients treated with infliximab. No differences were observed between the treatment groups in the changes in CTX levels from baseline to weeks 2 or 24.

After 2 years of therapy, greater median reductions in serum levels of TGF-β and CTX and greater median increases in BAP levels were observed as compared with weeks 2 and 24 (fig 1). Changes in serum marker levels for patients treated with placebo who crossed over to infliximab at week 24 were similar to those for patients who were originally assigned to receive infliximab.
The significant reductions from baseline to weeks 2 and 24 in serum levels of IL-6 and VEGF observed in patients treated with infliximab compared with patients treated with placebo in the ASSERT study have been previously reported.16
Changes in bone mineral density following infliximab treatment
At week 24, significant increases from baseline in BMD scores were observed in the spine (p<0.001) and hip (p = 0.040) of patients in the infliximab group (fig 2A). The corresponding median per cent increase in spinal BMD scores was 2.5% in patients treated with infliximab and 0.5% in patients treated with placebo (p<0.001), and the median per cent increase in hip BMD scores was 0.5% in patients treated with infliximab and 0.2% in patients treated with placebo (p = 0.033) (fig 2B). Similar increases were observed in the T scores of the spine (p<0.001) and hip (p = 0.017) at week 24 (fig 2C). Changes from baseline to week 102 in spine and hip T scores and total BMD increased further over the week 24 values for the infliximab group. The median per cent increase in spinal BMD scores was 6.8% in the infliximab group and 4.1% in the placebo/infliximab group; the median per cent increase in hip BMD scores was 1.8% and 0.9% respectively (fig 2B). Supplemental table 1 summarises the proportions of patients with osteopenia or osteoporosis at baseline and weeks 24 and 102.

{kind=link}
{kind=link}
Syndesmophytes
At baseline, approximately two-thirds of all patients had syndesmophytes as detected by the analysis of radiographs (table 1). No statistically significant differences were observed in the percentage increase in BMD from baseline to week 102 for patients who developed 1 or more syndesmophytes compared with those who did not, from baseline to week 102 (supplemental table 2).
Associations between biomarker levels and changes in bone mineral density of the spine
Univariate correlations
In the infliximab group, high baseline levels of IL-6 (r = 0.146, p = 0.0489), VEGF (r = 0.146, p = 0.0453), osteocalcin (r = 0.262, p = 0.0002), BAP (r = 0.262, p = 0.0002) and CTX (r = 0.189, p = 0.0088) correlated significantly with increases from baseline to week 24 in spinal BMD scores. Decreases from baseline to weeks 2 and 24 in IL-6 (r = −0.192, p = 0.0111 and r = −0.206, p = 0.0073 respectively) and VEGF (r = −0.245, p = 0.0007 and r = −0.226, p = 0.0025 respectively) and increases from baseline to week 24 in BAP (r = 0.153, p = 0.0382) also correlated with increases in spinal BMD scores from baseline to week 24. In the placebo group, no significant correlations were observed between baseline biomarker levels and increases in spinal BMD scores at week 24. However, decreases from baseline to week 2 in IL-6 (r = −0.258, p = 0.0392) and increases from baseline to week 24 in CTX (r = 0.241, p = 0.0479) correlated with increases in spinal BMD scores at week 24.
Data for both treatment groups were combined to evaluate correlations between BMD scores and biomarker levels and changes from baseline to week 102 because all patients were receiving infliximab after placebo crossover to infliximab at week 24. Results for the combined group at week 102 were similar to week 24. High baseline levels of IL-6 (r = 0.207, p = 0.0030), VEGF (r = 0.181, p = 0.0077), TGF-β (r = 0.143, p = 0.0356) and CTX (r = 0.179, p = 0.0084) correlated moderately with increases in spinal BMD scores at week 102. The strongest relationships were between the increase in spinal BMD scores at week 102 and high baseline osteocalcin (r = 0.335, p<0.0001) and BAP (r = 0.251, p = 0.0002) levels. Decreases in IL-6 (r = −0.255, p = 0.0003) and VEGF (r = −0.330, p<0.0001) and increases in BAP (r = 0.206, p = 0.0029) at week 2 correlated with increases in spinal BMD scores at week 102. A similar pattern was observed for changes at week 24 in the levels of IL-6 (r = −0.285, p<0.0001), VEGF (r = −0.280, p<0.0001) and BAP (r = 0.211, p = 0.0024). Additionally, there was a weak but statistically significant correlation between increases in osteocalcin at week 24 and increases in spinal BMD scores at week 102 (r = 0.168, p = 0.0165). Similar changes were observed when data for only patients with syndesmophytes at baseline were included in the analysis (data not shown).
Multiple regression analyses
In the infliximab group, results of a multiple linear regression analysis using a model including baseline biomarker levels (IL-6, VEGF, TGF-β, osteocalcin, BAP and CTX), syndesmophyte development (from baseline to week 102), and changes from baseline to week 24 in spinal BMD scores revealed that none of the variables were significantly associated with increases in spinal BMD scores (table 3). Similarly, per cent changes from baseline to week 2 in these biomarkers and syndesmophyte development were not significantly associated with changes from baseline to week 24 in spinal BMD scores.
Further, in a model that included baseline biomarker levels (IL-6, VEGF, TGF-β, osteocalcin, BAP, CTX), syndesmophyte development (from baseline to week 102), and changes in spinal BMD scores from baseline to week 102, osteocalcin was the only significant variable associated with increases in spinal BMD scores. In contrast, the results of a regression analysis using a model that included changes from baseline to week 2 in biomarker levels (IL-6, VEGF, TGF-β, osteocalcin, BAP, CTX), syndesmophyte development (from baseline to week 102), and changes from baseline to week 102 in spinal BMD scores revealed that BAP, CTX and VEGF were the only significant variables associated with increases in spinal BMD scores. None of the other markers were significantly associated with increases in spinal BMD scores.
Associations between biomarker levels and changes in bone mineral density of the hip
Univariate correlations
In the univariate analysis, no baseline biomarker levels correlated with increases from baseline to week 24 in hip BMD scores for either treatment group. However, in the combined group, high baseline levels of TGF-β (r = 0.170, p = 0.0140), CTX (r = 0.173, p = 0.0120), osteocalcin (r = 0.209, p = 0.0024) and BAP (r = 0.231, p = 0.0008) correlated significantly with increases in hip BMD scores from baseline to week 102.
In the placebo group, there were no significant correlations between changes in biomarker levels from baseline to weeks 2 or 24 and increases from baseline to week 24 in hip BMD scores. In the infliximab group, decreases from baseline in VEGF at weeks 2 and 24 (r = −0.201, p = 0.0061 and r = −0.156, p = 0.0379 respectively) and increases in BAP from baseline to week 2 (r = 0.187, p = 0.0111) correlated significantly with increases from baseline in hip BMD scores at week 24. Similarly, in the combined group, decreases in VEGF from baseline to weeks 2 and 24 (r = −0.187, p = 0.0071 and r = −0.232, p = 0.0010 respectively) and increases from baseline to week 2 in BAP (r = 0.154, p = 0.0286) correlated significantly with increases from baseline to week 102 in hip BMD scores. Also in the combined group, decreases from baseline to week 24 in IL-6 (r = −0.155, p = 0.0348) and TGF-β (r = −0.173, p = 0.0153) and increases from baseline to week 24 in osteocalcin (r = 0.155, p = 0.0295) correlated with increases in hip BMD scores from baseline to week 102. Similar changes were observed when data for only patients with syndesmophytes at baseline were included in the analysis (data not shown).
Multiple regression analyses
In the infliximab group, results of the multiple linear regression analysis using a model that included baseline biomarker levels (IL-6, VEGF, TGF-β, osteocalcin, BAP and CTX), syndesmophyte development (from baseline to week 102), and changes from baseline to week 24 in hip BMD scores revealed that osteocalcin was the only significant variable associated with increases in hip BMD scores (table 3). Osteocalcin was also the only significant variable associated with increases in hip BMD scores at week 102 using a model that included baseline biomarker levels (IL-6, VEGF, TGF-β, osteocalcin, BAP, CTX) and syndesmophyte development (from baseline to week 102). In contrast, in the infliximab group, the results of a multiple linear regression analysis using a model that included changes from baseline to week 2 in serum markers (IL-6, VEGF, TGF-β, osteocalcin, BAP, CTX), syndesmophyte development (from baseline to week 102), and changes from baseline to weeks 24 and 102 in hip BMD scores revealed that BAP and CTX were the only significant variables associated with increases in hip BMD scores at week 24 (table 3). BAP was also significantly associated with increases in hip BMD scores at week 102. None of the other markers were significantly associated with increases in hip BMD scores.
DISCUSSION
To our knowledge, these results represent the largest randomised controlled study of the effect of an antitumour necrosis factor antibody agent on BMD measurements (spine and hip). Increases in BMD following treatment with infliximab have been previously reported for patients with spondyloarthropathy,17 rheumatoid arthritis,18 19 and Crohn’s disease.20 In our study, greater increases in both spine and hip BMD scores were observed at week 24 in patients who received infliximab compared with placebo. The differences between the groups were greater for the spine than for the hip. Placebo-treated patients who crossed over to infliximab at week 24 showed increases in BMD scores at week 102; however, the magnitude of increase in BMD for patients initially assigned to infliximab treatment was greater at week 102, suggesting a benefit from earlier treatment with infliximab.
In the current study, treatment with infliximab resulted in stronger correlations between IL-6 and VEGF and between VEGF and TGF-β but weaker correlations between CTX and osteocalcin and between CTX and BAP. These results suggest that changes in levels of IL-6, VEGF and TGF-β are associated with the changes in disease processes that occur with infliximab treatment in AS. Significant univariate correlations were observed between baseline osteocalcin and both increases in spinal BMD scores at weeks 24 and 102 and increases in hip BMD scores at week 102 in the infliximab group. Further, in the multiple regression analysis that included all biomarkers and syndesmophyte development, only baseline osteocalcin levels were consistently associated with increases in spinal and hip BMD scores at week 102 for patients in the infliximab group. Baseline osteocalcin levels were also associated with increases in BMD hip scores at week 24. In comparison, two small-scale studies lacking follow-up of treatment effects in patients with AS did not show a relationship between osteocalcin levels and BMD scores.21 22 Our results suggest that baseline osteocalcin levels may have utility for predicting increases in hip and spinal BMD scores among patients with AS receiving infliximab.
Infliximab treatment significantly increased the levels of the bone formation marker BAP; although, the magnitude of median increases from baseline at weeks 2 and 24 were small (approximately 6%), with wide variability among patients within each treatment group. Greater increases from baseline in BAP were observed at week 102 (33–38%), but these changes cannot be specifically attributed to infliximab because the study was not placebo-controlled after week 24. Further, significant univariate correlations were observed in the infliximab group between baseline BAP and both increases in spinal BMD scores at weeks 24 and 102 and increases in hip BMD scores at week 102. The results of a multiple regression analysis showed that early increases from baseline to week 2 in BAP were significantly associated with increases in BMD hip scores at week 24 and increases in both spinal and hip BMD scores at week 102 in the infliximab group.
Treatment with infliximab in patients with Crohn’s disease has been previously shown to result in a significant increase in BAP but not in N-telopeptide of type I collagen, a marker of bone resorption.23 The increases in BAP might be a result of tumour necrosis factor-α inhibition and the steroid-sparing effect of infliximab in Crohn’s disease. However, this explanation is not applicable to our analysis given that patients were prohibited from corticosteroid use in ASSERT. In contrast, a study of patients with rheumatoid arthritis treated with infliximab showed a significant decrease in N telopeptide of type I collagen levels without an associated increase in BAP levels after treatment,24 supporting a disconnect between these markers of bone formation and resorption. These results suggest that BAP may be a good marker of early changes in spine and hip BMD scores in response to treatment with infliximab.
We have shown previously that treatment with infliximab results in significant, early decreases in the inflammatory markers IL-6 and VEGF in patients with AS as compared with placebo.16 In our study, early median decreases in TGF-β were greater in the infliximab group than in the placebo group, but this difference was not statistically significant. Significant univariate correlations in the infliximab group were observed between early decreases in IL-6 and VEGF levels and increases in spinal BMD scores at weeks 24 and 102, and early decreases in VEGF were also associated with increases in hip BMD scores at weeks 24 and 102. Additionally, baseline VEGF levels correlated significantly with increases in spinal BMD scores from baseline to weeks 24 and 102, and baseline TGF-β levels correlated significantly with increases in hip BMD scores from baseline to week 102.
Increases in BMD scores in patients with AS may be confounded by the formation of syndesmophytes. However, in this study, patients who developed syndesmophytes had similar changes in BMD as those who did not develop syndesmophytes. Further, syndesmophyte development was not a significant variable associated with changes in either hip or spinal BMD scores at week 24 or 102 in our multiple regression models. Thus, the increases in BMD scores observed in patients treated with infliximab do not appear to be linked to syndesmophyte development in this study.
There are several important limitations to this study. This secondary analysis from the ASSERT study was not powered to assess the significance of relationships between changes in biomarker levels and the BMD of patients with AS who received infliximab. Changes in BMD were only assessed at two time points (weeks 24 and 102), and changes in biomarker levels were only assessed at three time points (weeks 2, 24 and 102); fluctuations of these variables between time points were not studied. A more frequent, and perhaps longer, follow-up of patients would provide a more complete understanding of the long-term effects of infliximab therapy on both fluctuations in biomarker levels and BMD of the spine and hip in patients with AS. The variability in the changes in biomarker levels, particularly at weeks 2 and 24, limits the utility of these surrogate markers of BMD at the individual patient level.
In conclusion, patients with AS who received infliximab showed significant increases in BMD of the hip and spine at 24 weeks and 2 years. High baseline osteocalcin levels and early increases in BAP were consistently associated with these increases in BMD.
Acknowledgments
The authors wish to thank the patients, investigators and study personnel who made the ASSERT trial possible. We acknowledge Joseph Marini, Eva Silvestro and Elizabeth Lee-Rykaczewski of Centocor Research and Development, Inc. for their laboratory expertise, Scott Newcomer of Centocor, Inc. for his expertise and assistance with the development of the manuscript, and Stephen Xu of Centocor, Inc. for his biostatistical support.
REFERENCES
Supplementary materials
web only appendices 68/2/175
Files in this Data Supplement:
Footnotes
Funding: This study was funded by Centocor Research and Development, Inc.
Competing interests: DvdH, AD and DGB have received research funding and/or consulting fees from Centocor and Schering-Plough. SV, CW, DGB and JH are employees of Centocor and own Johnson & Johnson stock.
▸ Additional supplemental tables 1 and 2 are published online only at http://ard.bmj.com/content/vol68/issue2
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.