Article Text

Abstract
Objectives: To compare the ability of two different dedicated extremity MRI (E-MRI) units and conventional radiography (CR) for identifying bone erosions in rheumatoid arthritis (RA) metacarpophalangeal (MCP) and wrist joints.
Methods: CR and two MRI examinations (using 0.2 T Esaote Artoscan and 0.2 T portable MagneVu MV1000 units) of 418 bones in the dominant wrist and second to fifth MCP joints of 15 patients with RA and 4 healthy controls were performed and evaluated blindly for bones being visible and for erosions.
Results: In MCP joints, MagneVu visualised 18.5% of bones entirely and 71.1% were 67–99% visualised. In wrists, MagneVu visualised 1.5% of bones entirely, 39.8% were 67–99% visualised and 19% were not visualised at all. Artoscan and CR visualised all bones entirely. Artoscan, MagneVu and CR found 22, 19 and 15 bones with erosions in MCP joints and 66, 40 and 13 bones with erosions in wrist joints, respectively. With the previously validated Artoscan unit as standard reference, MagneVu and CR had sensitivities of 0.82 and 0.55, respectively, in MCP joint bones and 0.41 and 0.14 in wrist bones. Specificities of CR and MagneVu were comparable (0.82–0.99). The MagneVu unit was particularly more sensitive than CR for metacarpal heads and carpal bones. MagneVu MRI and CR detected 100% and 89%, respectively, of large erosions (Outcome Measures in Rheumatoid Arthritis Clinical Trials–Rheumatoid Arthritis MRI Scoring System (OMERACT-RAMRIS) score >1 on Artoscan) in MCP joints and 69% and 15.8% of large erosions in wrists.
Conclusions: Both E-MRI units detected more erosions than CR, in particular due to a higher sensitivity in metacarpal heads and carpal bones. The MagneVu unit detected fewer erosions than the Artoscan unit due to a lower average image quality and a smaller proportion of bones being visualised.
Statistics from Altmetric.com
Magnetic resonance imaging has been shown to be more sensitive than conventional radiography (CR) in visualising erosive damage in rheumatoid arthritis (RA)1 and bone lesions detected by MRI (erosions and bone oedema) are known to predict subsequent development of radiographic erosions.2–4
Further, a high soft tissue contrast makes MRI useful for detecting synovitis, tenosynovitis, enthesitis and bone oedema. Consequently, MRI has great potential as a powerful tool for monitoring disease activity and for prognosticating erosive disease in RA.
Dedicated extremity MRI (E-MRI) units (fig 1) are less expensive and more patient-friendly than the conventional whole-body units, in which patients are positioned in a narrow cylinder. The majority of the E-MRI units are low-field (<1.0 T) units. In recent studies, MRI findings using one of these units (the Esaote Artoscan) correlated very closely with high-field MRI results with respect to detection of erosion and synovitis, while the sensitivity for detecting bone oedema was low.5 6

The MagneVu, MV1000 (0.2 T) unit is a unique E-MRI unit since it is transportable (on wheels), does not need shielding and can be plugged in an ordinary wall power outlet and therefore has the potential to be an office-based tool in rheumatology clinics.
Recent studies using this machine report it to be superior to CR for detection of bone erosions in RA, but minimal data on validation has been published.7 8
The objective of the present study was to compare the ability of two different E-MRI units (the Esaote Artoscan and the MagneVu MV1000) and CR for identifying bone erosions in RA metacarpophalangeal (MCP) and wrist joints. Furthermore, we wanted to determine the sensitivity and specificity of MagneVu and CR for detecting bone erosion, with the Artoscan unit as the standard reference.
MATERIALS AND METHODS
A total of 15 patients (10 women, 5 men), all fulfilling the American College of Rheumatology (ACR) 1987 criteria for RA were included, as was a control group (4 healthy controls (2 women, 2 men, median age 56 years (range 35–67)). A total of 60% of the patients were positive for rheumatoid factor (>27 IU/litre) and 67% had a C- reactive protein (CRP) level <8 mg/litre (max 29 IU/litre). The median age of the patients was 58 years (range 25–79), and the median disease duration was 7.5 years (range 1–33). Median clinical and laboratory values for measures of disease activity were as follows: number of swollen joints 2.5 (range 0–9), number of tender joints 0.5 (range 0–20), 28-joint Disease Activity Score (DAS28) 2.7 (range 0–5.4). No members of the control group had signs or symptoms of joint disease.
A total of 13% of patients did not receive any disease-modifying antirheumatic drugs (DMARDs), 20% were treated with DMARDs other than methotrexate (MTX), 26.6% received MTX in monotherapy and 40% in combination therapy.
All patients were recruited from the Department of Rheumatology, Copenhagen University Hospital at Hvidovre, Denmark, and underwent two MRI examinations and CR of the wrist joints and second to fifth MCP joints of the dominant hand. Local ethics (Copenhagen and Frederiksberg) committee approval was obtained before starting the studies, and informed consent was obtained from all participants.
MRI
The two low-field MRI-units being tested were: (a) 0.2 T Artoscan MRI unit (Esaote Biomedica, Genoa, Italy) and (b) 0.2 T portable MV1000 MRI system (MagneVu Carlsbad, California, USA).
The slice thickness, repetition time (TR) and echo time (TE) were chosen in order to test and compare the best performances of both units rather than testing the same parameters on two different units. Both MRI scans were performed on the same day.
Image acquisition using the Artoscan E-MRI unit
The patients were seated in an adjustable chair with the dominant hand positioned in the centre of a dual phased array wrist coil in a neutral position (fig 1B).
A T1-weighted three dimensional gradient echo sequence (3-D T1-GE), with subsequent multiplanar reconstruction (slice thickness 1 mm, TR 30 ms, TE 12 ms, number of excitations (NEX) 1, matrix 192×160×80, field of view (FOV) 140×140 mm, scan time 6 min), covering the second to fifth MCP joint and metacarpal bases, all carpal bones and the distal radius and ulna was performed (fig 2). In cases of very large hands, wrist and MCP joint images were obtained separately.
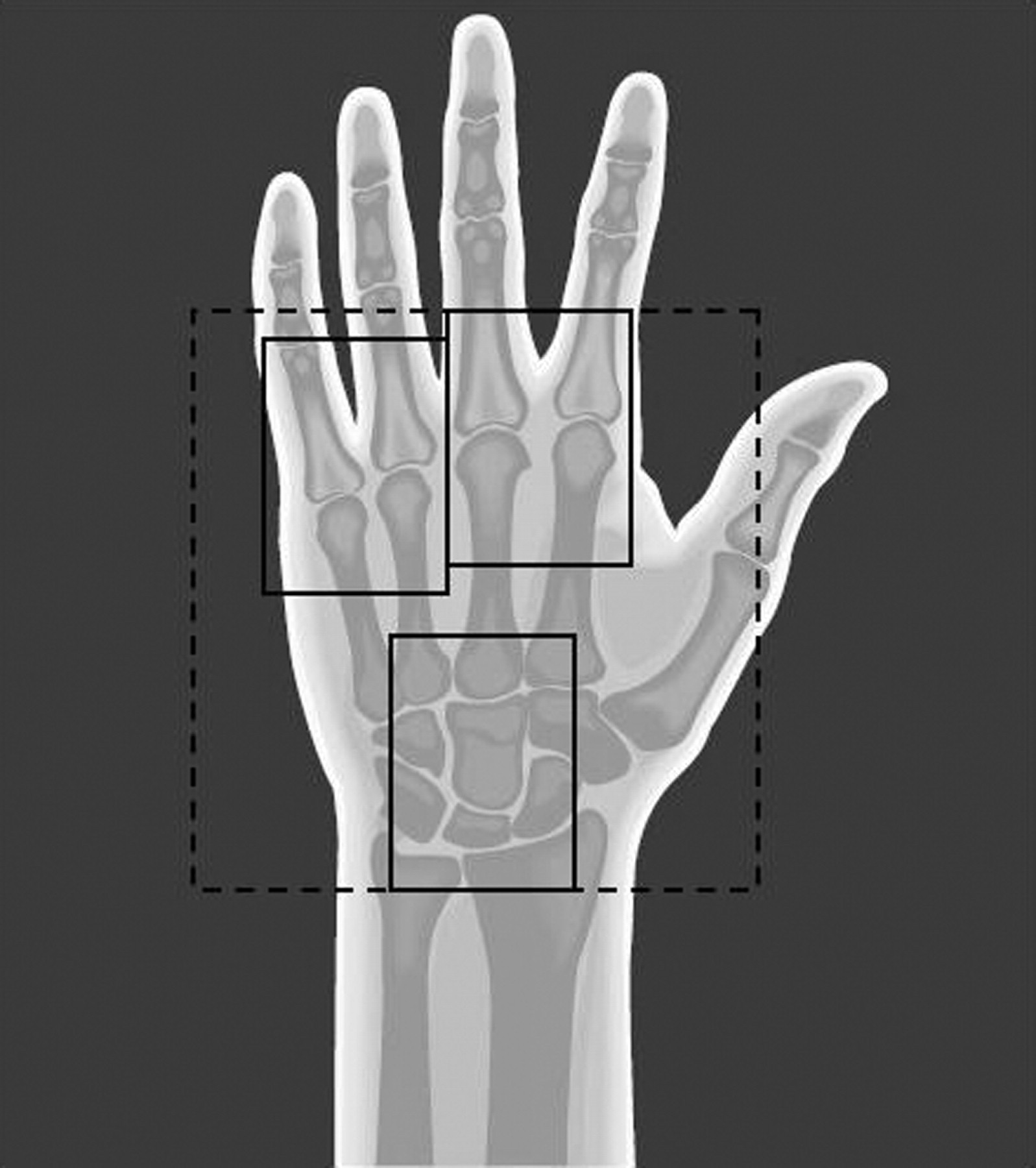
Image acquisition using the MagneVu MV1000 E-MRI unit
To cool the magnet the antenna was filled with liquid nitrogen followed by calibration before each examination. The patients were seated in an armchair with the dominant hand in the coil, palmar side facing up (fig 1A). Pads of variable thicknesses were used to place the region of interest in the FOV. Finally, the hand was fixed in position by a pillow designed specifically for this purpose (fig 1A). The unit allowed imaging of a box-shaped volume of a fixed size of 50×75×10 mm (FOV 50×75 mm; slab thickness 10 mm). This box was invariably located from 10 mm to 20 mm above the surface of the coil, ie, the FOV could not be moved at all, and the only option to visualise a different area was to move the hand.
A 3-D T1-GE sequence (16 slices of a thickness of 0.62 mm, 1 mm coronal in-plane resolution, TR/TE: 100/27 ms, NEX 2, FOV 50×75 mm, acquisition time 15.11 min) was performed of the following regions: second and third MCP joints, fourth and fifth MCP joints and the wrist of the dominant hand (fig 2). For the MCP joints, the aim was to visualise the most dorsal part of the bone in the first coronal image. Furthermore, we aimed to visualise at least 1 cm of the shaft of the metacarpal bone and proximal phalanges respectively. In the wrist we particularly aimed to visualise the following bones: scaphoid, lunate, capitate, distal radius, trapezium and trapezoid.
The T1 weighted sequences of the MCP joints were followed by a short tau inversion recovery (STIR) sequence of the same area (TR 100, TE 29, NEX 4, matrix (1×1×0.6 mm, FOV 50×75 mm, scan time 13.20 min).
Conventional radiography
CR of dominant wrist and MCP joints were performed in posterior-anterior and Nørgaard projections within a month of the MRI examination.
Image evaluation
The images were separately and evaluated blindly; the radiographs by a musculoskeletal radiologist (AV) and the two sets of MRI images by a rheumatologist (MØ) experienced in reading RA MRI images (both were blinded to clinical results and other imaging findings, ie, when evaluating Artoscan images the reader was blinded to results from MagneVu and CR) for presence or absence of erosion in each bone at the wrist and each bone in the MCP joints. Furthermore, Artoscan MRI images were evaluated by the Outcome Measures in Rheumatoid Arthritis Clinical Trials (OMERACT) RA MRI scoring method (RAMRIS) for erosions9 and on the MagneVu images the percentage of each bone being visualised by MagneVu was estimated. Finally a possible relation between the OMERACT grade of bone erosion on the Artoscan images and the detection of erosions by MagneVu and CR was explored.
The STIR MagneVu images were planned to be assessed for the presence of synovitis and bone oedema.
Merge eFilm (Milwaukee, Wisconsin, USA) program, a commercially available software package, was used for reading of the MRI images. This software enables digital image viewing and provides the reader with advanced features of image viewing, for example, window/level settings, zooming and 3-D localising for accurate identification of specific lesions in perpendicular planes.
Statistical analysis
The sensitivity, specificity and accuracy of CR and MagneVu MRI were calculated using interpretations from the Artoscan MRIs as the reference method.
RESULTS
MCP joint coverage
The Artoscan unit allowed visualisation of the entire bones of the second to fifth MCP joints in two planes.
The MagneVu allowed only visualisation of 1 cm of the ventral–dorsal diameter (slab thickness = 1 cm) of the bone, resulting in an incomplete visualisation of the majority of the examined joint areas (fig 3): 18.5% of bones were visualised entirely and 71.1% of bones were 67–99% visualised (see table 1).

{kind=link}
{kind=link}
{kind=link}
MCP joint sensitivity
A total of 76 metacarpal heads and 76 phalangeal bases were examined. Artoscan, MagneVu and CR detected 22, 19 and 15 erosions, respectively. The number of erosions seen in the different bones and the sensitivity, specificity and accuracy of MagneVu and CR when interpretations from the Artoscan unit were used as the reference method, are shown in table 1.
The sensitivity of MagneVu (0.82) for detecting erosions was higher than CR (0.55), which was mainly due to a higher sensitivity for metacarpal heads (MH). CR and MagneVu were equal in finding erosions in phalangeal bases (PB).
The quality of the MagneVu STIR images was so poor in all patients that assessment of synovitis or bone oedema was considered unreliable.
Wrist bone coverage
The Artoscan visualised the entire area from the distal radio-ulnar joint to the carpo-metacarpal joints. The FOV of MagneVu did not allow visualisation of the entire wrist (table 2). Of the 266 bones examined, 1.5% were visualised entirely, 39.8% were 67–99% visualised and 19% were not visualised at all.
Wrist sensitivity
266 wrist bones were examined. Artoscan, MagneVu and CR detected 66, 40 and 13 erosions, respectively. The distribution of the registered erosions and the sensitivity, specificity and agreement of MagneVu and CR, when interpretations from the Artoscan unit were used as the reference are shown in table 2.
The sensitivities of MagneVu and CR for detecting wrist bone erosions were low, but with MagneVu presenting with higher values (0.41) than CR (0.14). MagneVu showed the highest sensitivities in the radius, hamate and trapezoid. MagneVu found no erosions in the pisiform and trapezium, as these bones were not visualised in any patient.
OMERACT bone erosion score versus detection of erosions by MagneVu and CR
The OMERACT-RAMRIS grading of the Artoscan images were related to the presence of erosions on the MagneVu images; 61.5% of the Artoscan grade 1 erosions were detected by MagneVu and all erosions graded 2 or more on the Artoscan were detected by the MagneVu. CR detected all erosions graded >2 on the Artoscan and found 89% of erosions graded >1.
In the wrist, MagneVu found 69% of erosions graded >1 on the Artoscan and 25% of grade 1 erosions. CR detected 15.8% of erosions graded >1 on the Artoscan and 10% of grade 1 erosions.
Erosions not detected by MagneVu
In the MCP joints, one of five erosions not seen on MagneVu was missed due to the MagneVu not covering the erosion site. In one case erosion was suspected on coronal MagneVu images, but was not confirmed in the axial plane. In three cases movement artefacts made the evaluation difficult. In the wrist, 16 out of 41 (39%) erosions not seen on MagneVu were missed due to the MagneVu not covering the erosion site. In three (7%) cases erosions were suspected on coronal MagneVu images, but were not confirmed in the axial plane, in 16 (39%) cases movement artefacts made the evaluation difficult and in 5 (12%) cases a low signal to noise ratio (SNR) producing suboptimal images was considered the main reason for missing the erosion.
Erosions detected by CR or MagneVu, but not by Artoscan
In the MCP and wrist joints, respectively, 2 and 10 erosions were reported by MagneVu, but not by Artoscan. In 9 of these 10 wrist cases the reader had noted that the MagneVu images were not optimal for evaluation due to low imaging quality or the eroded area was located in the periphery of the FOV, making evaluation less certain.
Two erosions in the fifth metacarpal head and one in the trapezium were seen on CR but not by Artoscan. In this latter case, the Artoscan images were reported to have suboptimal quality.
DISCUSSION
This is the first study to compare and validate the smallest available MRI unit, the MagneVu unit, and CR, using a validated, dedicated MRI unit as the reference method. We chose to use Artoscan as the reference method since studies have shown this unit to be equivalent to standard high-field MRI regarding sensitivity and specificity for detecting erosive changes in wrists and MCP joints in patients with RA.5 6 The potential limitations of this approach are described below.
We found a higher sensitivity for MagneVu compared to CR for detecting erosions in the metacarpal heads (0.81 vs 0.44). In the wrist bones, the sensitivity was markedly lower, but still higher for MagneVu than CR (0.41 vs 0.14). In the phalangeal bases the sensitivity was comparable and low for MagneVu and CR. Specificities for MagneVu and CR were similar.
While CR and the Artoscan allowed evaluation of the entire MCP and wrist joints, the MagneVu only allowed assessment of limited parts of the bone, particularly in the wrist (tables 1 and 2).
The low sensitivity of CR for detecting erosions in the wrist bones is in accordance with earlier comparisons of CR and MRI.1 3 10 The particular difficulties of CR in the wrist joints, compared to MCP joints, can be explained by projectional superimposition of bones in this complex joint.
The relatively low sensitivity of the MagneVu unit can be explained by the inability to cover the wrist bones in one examination (table 2), our choice of the wrist examination protocol as the last sequence, preceded by approximately 1 h of examination of MCP joints (inevitably leading to a risk of movement artefacts), and difficulties with positioning the wrist optimally. A poor position was generally not disclosed before the end of the examination. In the majority of the examinations experiencing this problem, the patient was not willing to have a new wrist examination.
Using the Artoscan as the comparator for the MagneVu has advantages and disadvantages. Disadvantages include that it, being another low-field dedicated extremity MRI unit, is not as thoroughly validated as high-field MRI and may thus be considered less reliable. However, previous studies have shown very high reliability for the Artoscan using the exact sequences used in the present study when compared to high-field MRI.5 Furthermore, MRI of unilateral wrist and MCP joints using this unit have been shown to be more sensitive to erosive progression than CR of hands, wrists and forefeet.11 12 Therefore, we considered that comparison with this unit would give important new information of the potential of the hitherto unvalidated MagneVu unit. Furthermore, the selected approach allows direct comparison between the two units that are currently the most likely MRI competitors to CR for widespread use in RA joint imaging.
Our results indicate that, overall, the sensitivity of the MagneVu for detection of bone erosions is lower than that of the Artoscan, probably mainly related to the lower coverage of the joints (smaller FOV) but also as a result of a lower mean image quality (due to image quality in general but also frequent artefacts caused by the significantly longer acquisition times (6 min for the second to fifth MCP on the Artoscan vs 30 min on the MagneVu). The lower sensitivity, longer imaging time and the inability to move the FOVs are other disadvantages of the MagneVu. Additionally, it is a fact that STIR sequences are unsuitable for examination of synovitis and bone oedema combined with the fact that additional post-contrast imaging is not feasible due to the long examination time and small FOV. However, it should be emphasised that the MagneVu was still markedly more sensitive for bone erosions than CR, and since CR is the standard method used, implementing MagneVu MRI may still be an improvement compared to the examination standards used today.
Further studies on the MagneVu unit are needed. It should be clarified which anatomic areas should be examined. The highest image quality was obtained for MCP joints, but erosive changes are often detected in the wrist.4 11 The MagneVu software has improved in the most recent version by adding 0.5 cm to the slab thickness. Therefore it is relevant to investigate to what degree this improves the bone coverage and detection of erosions. Also, a validation of erosion detection by E-MRI in general should be undertaken (eg, with CT as the standard reference).
In conclusion, the MagneVu MV1000 and Esaote Artoscan dedicated extremity MRI units detected more erosions than CR, based mainly on a higher sensitivity in the metacarpal heads. The Artoscan detected more erosions than the MagneVu unit due to a higher average image quality and a smaller proportion of bone being visualised by the MagneVu. The MagneVu images did not allow assessment of inflammatory changes as synovitis or bone marrow oedema.
Acknowledgments
We acknowledge The Danish Rheumatism Association, Elisabeth and Karl Ejnar Nis-Hanssens Memorial Award and Departments for Research, Quality and Education, Southern Region for financial support and MagneVu, Carlsbad, USA for donating the MagneVu MV1000 E-MRI unit for research purposes.
REFERENCES
Footnotes
Competing interests: None declared.
Funding: We acknowledge The Danish Rheumatism Association, Elisabeth and Karl Ejnar Nis-Hanssens Memorial Award and Departments for Research, Quality and Education, Southern Region for financial support.
Ethics approval: Local ethics (Copenhagen and Frederiksberg) committee approval was obtained before starting the studies, as was informed consent from all participants.
Patient consent: Informed consent was obtained for the publication of the details in this report.