Article Text

Abstract
Objective: To assess the effect of rituximab on the efficacy and safety of influenza virus vaccine in patients with rheumatoid arthritis (RA).
Methods: The study group comprised patients with RA treated with conventional disease-modifying drugs with or without rituximab. Split-virion inactivated vaccine containing 15 μg haemagglutinin/dose of B/Shanghai/361/02 (SHAN), A/New Caledonian/20/99 (NC) (H1N1) and A/California/7/04 (CAL) (H3N2) was used. Disease activity was assessed by the number of tender and swollen joints, duration of morning stiffness and evaluation of pain on the day of vaccination and 4 weeks later. CD19-positive cell levels were assessed in rituximab-treated patients. Haemagglutination inhibition (HI) antibodies were tested and response was defined as a greater than fourfold rise 4 weeks after vaccination or seroconversion in patients with a non-protective baseline level of antibodies (<1/40). Geometric mean titres (GMT) were calculated in all subjects.
Results: The participants were divided into three groups: RA (n = 29, aged 64 (12) years), rituximab-treated RA (n = 14, aged 53 (15) years) and healthy controls (n = 21, aged 58 (15) years). All baseline protective levels of HI antibodies and GMT were similar. Four weeks after vaccination, there was a significant increase in GMT for NC and CAL antigens in all subjects, but not for the SHAN antigen in the rituximab group. In rituximab-treated patients, the percentage of responders was low for all three antigens tested, achieving statistical significance for the CAL antigen. Measures of disease activity remained unchanged.
Conclusion: Influenza virus vaccine generated a humoral response in all study patients with RA and controls. Although the response was significantly lower among rituximab-treated patients, treatment with rituximab does not preclude administration of vaccination against influenza.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/
Statistics from Altmetric.com
Infection is one of the leading causes of morbidity and mortality in patients with rheumatoid arthritis (RA),1 ,2 who have nearly twice the rate of infection compared with matched non-RA controls.3 This might be related to the disease itself through either altered immunological function or due to other factors, such as immobility, skin defects, Felty’s syndrome and more. Alternatively, treatment with corticosteroids and other immunosuppressive drugs may also predispose patients with RA to the development of severe infections.4
Vaccination against influenza is currently recommended to patients who have chronic diseases, including RA.5 We and others6 ,7 have shown that vaccination against influenza is safe and that it induces a satisfactory humoral response, although one that is lower than in healthy controls. The humoral response of patients with RA to vaccination against influenza does not seem to be affected by the use of prednisone, disease modifying antirheumatic drugs (DMARDs) or tumour necrosis factor α blockers.6 ,7
Results of recent clinical studies8 using the B-cell-depleting monoclonal antibody rituximab indicate that B-cell-targeted treatment promises to be a major advance in the treatment of RA. B-lymphocyte depletion with rituximab, either alone or in combination with cyclophosphamide or methotrexate (MTX), has been shown to have efficacy in patients with RA who experience incomplete response to MTX.8
Rituximab is a genetically engineered chimeric anti-CD20 monoclonal antibody that selectively targets CD20+ B cells and induces a transient depletion of the CD20+ mature B-cell subpopulation. Although the levels of pre-existing antibody levels against tetanus and pneumococcal polysaccharide were shown to be unaffected by a single course of rituximab,9 its effect on the immune response to active immunisation in patients with RA has not yet been investigated. The purpose of our study was to evaluate the effect of rituximab on the immunogenicity of vaccination against influenza in patients with RA and to assess safety in these patients.
PATIENTS AND METHODS
Subjects
Forty-three consecutive outpatients routinely treated at two departments of rheumatology who fulfilled the American College of Rheumatology criteria for RA10 and 21 healthy hospital personnel matched for age and gender participated in the study. Fourteen of the 43 patients with RA had been treated with rituximab (rituximab group) during the previous 18 months (seven of them during the past 6 months) according to the standard protocol used in RA—that is, two infusions of 1000 mg each along with 100 mg methylprednisolone intravenously with background weekly MTX. The remaining 29 patients with RA (non-rituximab) were receiving different DMARDs excluding tumour necrosis factor α blockers or other biological agents. Patients were required to be on stable drug treatment for the 3 months preceding the vaccination. The vaccinations consisted of 0.5 ml split virion inactivated vaccine (Vaxigrip, Promedico) containing a 15 μg haemagglutinin (HA) dose of A/California /7/04 (CAL) (H3N2), B/Shanghai /361/02 (SHAN) and A/New Caledonian/20/99 (NC) (H1N1), administered intramuscularly. Exclusion criteria were pregnancy, a history of past vaccination allergy, a known allergy to egg products, hyposplenism, and active RA necessitating a recent change in the drug regimen.
Clinical assessment
Each subject gave a complete history including drug use and underwent a physical examination before vaccination. Clinical assessment on the day of vaccination and 4 weeks later included the following: duration of morning stiffness (in minutes); evaluation of daytime and nocturnal pain using a visual analogue scale of 10 cm, and count of the number of tender and swollen joints (28 joint counts).
Laboratory assessment of disease activity included erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) on the day of the vaccination and 4 weeks later. A complete blood count was performed for all treated patients, with assessment of total lymphocyte count and the subpopulations, including CD5, CD19 and CD20, assessed as frequency and absolute numbers.
Haemagglutination inhibition test
The immunogenicity of the vaccine was tested by the haemagglutination inhibition (HI) test. Influenza virus has two important surface glycoproteins, HA and neuraminidase. Antigenic classification and subtyping of influenza viruses are based on these two glycoproteins. HA has a key role in virus cell entry by binding to cell surface receptors, which are also found on red blood cells of certain species. Binding to red cells results in haemagglutination, which can be observed as a carpet of agglutinated red cells at the bottom of a tube or microtitre well. In the HI test, antibodies directed against the viral HAs block the virus from binding to the blood cells and thus inhibit the haemagglutination reaction.
The pre- and postimmunisation HI antibodies were tested at the Central Virology Laboratory of the Israeli Ministry of Health using the HI test according to a standard WHO procedure.11 Serum samples were separated, code labelled, and stored at −20°C until tested. They were treated with receptor-destroying enzyme cholera filtrate to remove non-specific inhibitors, and with Turkey red blood cells to remove non-specific agglutinins. The treated serum samples were tested by an HI test against the three antigens included in the vaccine, CAL, SHAN and NC. The working dilution (test dose) of each antigen contained four HA units in 25 μl of antigen. Test doses were diluted in phosphate-buffered saline and added to serial dilution of antiserum. The HA inhibition titre was determined as the highest dilution of serum that completely inhibited haemagglutination of red blood cells.
The titre of an antiserum not showing any inhibition was recorded as <10. Humoral response was defined as either a fourfold or more rise in titre, or a rise from a non-protective baseline level of <1/40 to ⩾1/40 in HI antibodies 4 weeks after vaccination.12 ,13 Geometric mean titres of antibodies were calculated to assess the immunity of the whole group.
Outcomes of the study
The primary outcome was the percentage of patients from the three groups (RA treated with rituximab, RA treated with DMARDs alone and controls) showing a humoral response to each of the three serotypes. Secondary outcomes included predictors of immunogenicity in patients with RA and the safety of the vaccine in these patients.
Appropriate informed consent was obtained from all patients, and the clinical research was conducted in accordance with guidelines for human experimentation specified by the Tel Aviv Sourasky Medical Centre and the Rambam Health Care Centre. The study was approved by the ethics committee of both medical centres.
Statistical methods
Non-parametric tests were used for the analysis since most variables were not normally distributed (based on the Shapiro–Wilk test). In addition, parametric tests were performed for the log transformation of the variables.
Associations between the response to vaccination and patient group and the drug use were examined using the χ2 and the Fisher exact tests.
Patients with positive reactions to vaccination were compared with those who did not react with respect to clinical measures—use of drugs at baseline, change in disease indices (number of tender and swollen joints, morning stiffness, pain intensity), ESR, CRP, etc—using the Mann–Whitney U test and the t test for independent samples.
Change in drug use was evaluated by the McNemar test, change in the number of drugs by the Wilcoxon non-parametric test, and change in drug dosage by paired t tests. A binomial logistic regression model was constructed to assess the importance of the different variables relative to the immunogenicity response.
Statistical analysis was carried out using the SPSS system for Windows, release 14.0.
RESULTS
Characteristics of patients and control subjects
The three groups were statistically similar in age and gender and comprised mostly women (table 1). The mean disease duration was 15.5 years for the patients with RA and 16.5 years in the rituximab group. At the time of vaccination, all patients with RA were being treated with at least one DMARD (table 2). Most (76%) of the non-rituximab RA subjects and 86% of the rituximab RA subjects were being treated with MTX at a mean dose of 12.7 and 14.6 mg/week, respectively. A significantly higher proportion of patients in the rituximab group was treated with prednisone (50% vs 28% non-rituximab, p = 0.003) At the time of vaccination, patients in the rituximab group were profoundly B-cell depleted, with a mean (SD) level of 14.2 (22.8) CD19+ B cells, 0.98% of total lymphocytes (range 0–80 μl). Four weeks after vaccination, the mean level of CD19+ B cells was 22, 1.6% of total lymphocytes (range 0–50 μl).
Effect of vaccination against influenza on disease activity
Vaccination against influenza was not associated with a significant worsening of any clinical or laboratory indices of disease activity in both groups of rheumatoid patients (table 3). A few subjects reported mild adverse events after vaccination: two rheumatoid patients in the rituximab group and none of the controls developed symptoms of mild upper respiratory tract infection within 4 weeks following vaccination.
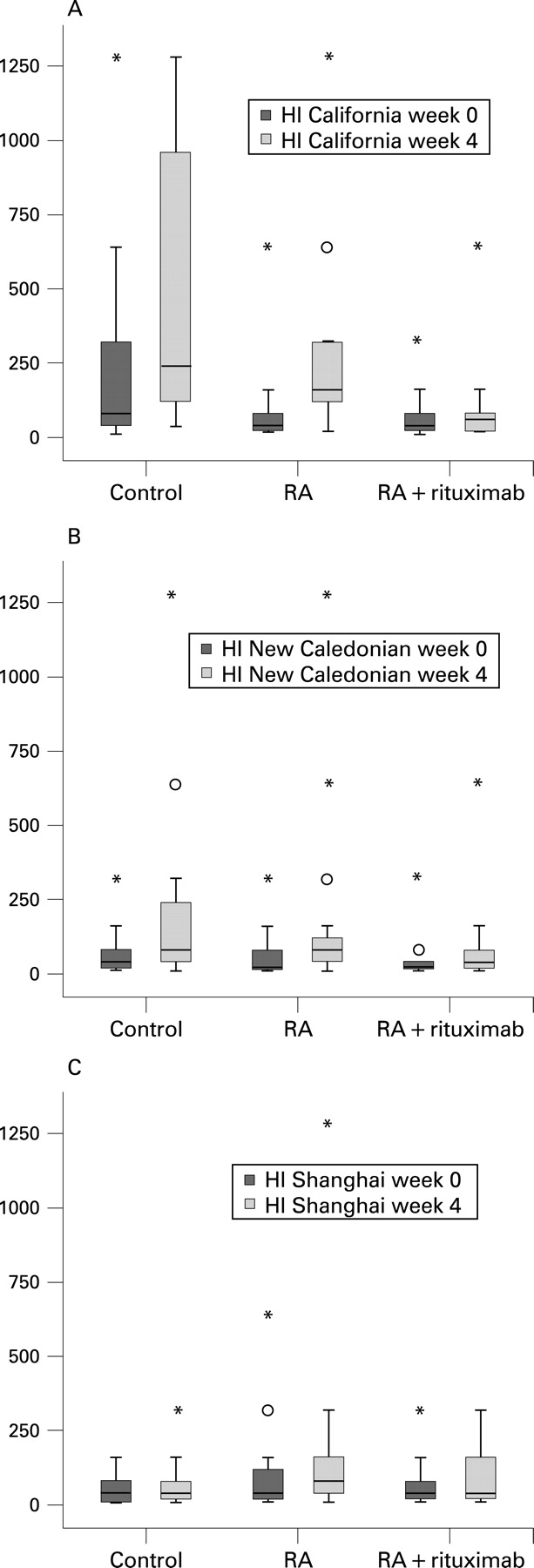
Immunogenicity of influenza vaccine
Pre-vaccination HI antibody levels—that is, as a result of previous infection or vaccination, did not differ significantly between patients with RA and controls. Four weeks after vaccination, all study participants in the control groups had significant increases in their geometric mean titres of HI antibody against each of the antigens tested, suggesting a satisfactory humoral response on the part of the whole group. The rituximab group showed a significant rise for NC and CAL antigens but not for SHAN (fig 1).

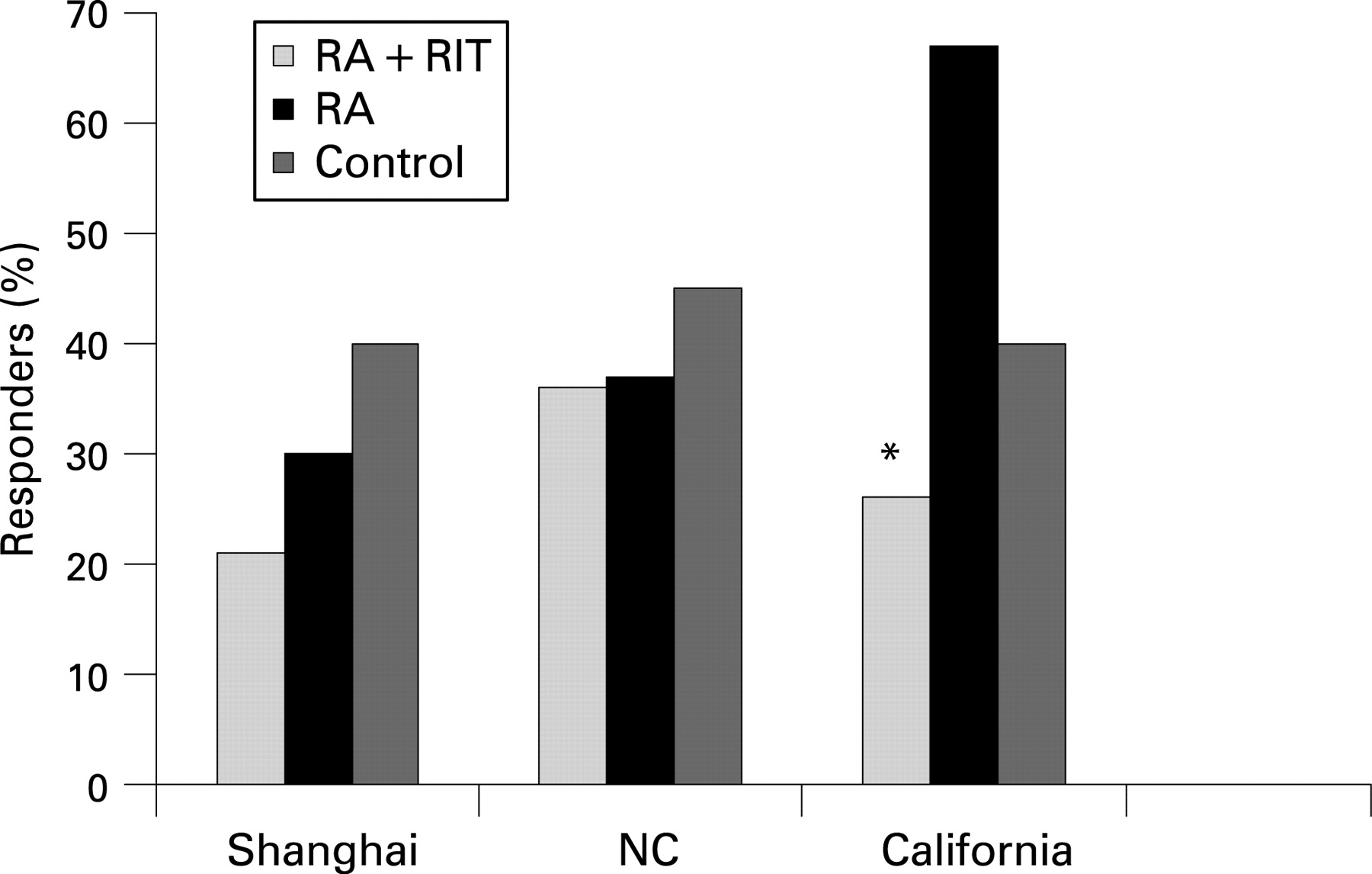
Individual responses of rheumatoid patients and controls to vaccination against influenza
Although patients with RA and controls responded to most of the antigens, the vaccine did not appear to be uniformly immunogenic among all the patients. Levels of HI antibodies <1/40 are considered to be non-protective. A satisfactory humoral response was defined as a fourfold or more rise in HI antibodies 4 weeks after vaccination in patients with baseline HI antibody levels >1/40, or a rise of HI levels to ⩾1/40 in patients with non-protective baseline levels of <1/40. When this definition was used, the proportion of responders to the CAL antigen was significantly lower in the rituximab group than in the non-rituximab group (21% vs 67%, respectively; p = 0.006). The proportion of responders to the SHAN and NC antigens was similar in the three groups (fig 2). Response to more than one antigen was obtained in 14% of the rituximab patients, 48% of the non-rituximab patients and 40% of the healthy controls (p = 0.53). No difference was noted between the three groups in the proportion of responders to all three antigens or to none of them.
{kind=link}
{kind=link}
Predictors of immunogenicity
We attempted to identify clinical and/or laboratory indices which might predict a poor response to the influenza virus vaccine. We could not find any association between the humoral response and age, sex, disease duration, swollen and tender joint counts, duration of morning stiffness, level of pain, ESR and CRP levels, the use or dose of prednisone or MTX. The proportion of responders to the CAL antigen was significantly higher in patients treated with a smaller number of DMARDs (3.95 vs 7, p = 0.02) while no difference was noted for the two other antigens. Multivariate regression analysis did not identify any predictor of immunogenicity. We also could not find any correlation between immunogenicity and the level of CD19+ B cells, CD+19 frequency or the time interval since receiving rituximab in the rituximab-treated patients with RA (table 4), although the very low levels of CD+19 may not allow evaluation of its influence on immunogenicity.
DISCUSSION
The findings of the current study demonstrated that vaccination against influenza generated a humoral response for two of three antigens tested (NC and CAL but not SHAN) in rheumatoid patients treated with rituximab. The proportion of responders to one of the antigens only (CAL) was significantly lower in the patients treated with rituximab, while the response rate for the other two antigens was similar among all participants. The humoral response was not affected by different clinical and demographic characteristics of RA, or by the level of B cells or the length of time that had passed since receiving rituximab.
The immune responsiveness of patients treated with rituximab has been examined by several studies, most of them performed in patients with lymphoma. Horwitz et al evaluated the ability of 35 patients with lymphoma who were being treated with rituximab and cyclophosphamide to respond to vaccination against tetanus, haemophilus influenza and pneumococcus administered at 6 and 9 months after their last rituximab infusion.14 Most of the patients produced protective antibody levels against haemophilus and tetanus but not against pneumococcus.14 Others have reported significantly decreased responses to recall antigen, tetanus and polio immunisation and no responses to primary antigen, keyhole limpet haemocyanin and hepatitis A immunisation after rituximab monotherapy in 11 patients with lymphoma.15 Another study assessed immunisation with neoantigen phiX174—an established method of assessing in vivo antibody response—in patients with chronic renal failure who were treated with rituximab before transplantation.16 Rituximab significantly inhibited the antibody response to phiX174 at all time points after both primary and secondary immunisations compared with subjects with chronic renal failure not treated with rituximab (p<0.001) and normal controls (p<0.001).16
Data on the effect of rituximab on immune responsiveness of patients with autoimmune diseases are scarce. Edwards et al 8 demonstrated that despite complete depletion of B cells in patients with RA treated with rituximab, levels of immunoglobulins as well as anti-tetanus antibody titres remained stable, reflecting the presence of long-living plasma cells.17 Although serum levels of rheumatoid factor decreased during treatment with rituximab, no changes in anti-tetanus toxoid or anti-pneumococcal polysaccharide antibody levels were seen.18 In another study,9 serum levels of IgG anti-tetanus toxoid antibodies and antibodies to pneumococcal capsular polysaccharide did not change significantly in 16 patients with active systemic lupus erythematosus who received rituximab. On the other hand, Vallerskog et al recently investigated how rituximab-induced B-cell depletion affected antibody titres in patients with systemic lupus erythematosus.19 Serum levels of IgG and antibodies against measles and tetanus remained unchanged, while decreases in IgM, IgE, anti-dsDNA and anti-C1q antibodies were seen.
As far as we know, the immune response to active immunisation of patients with RA treated with rituximab has not been studied before. We now provide evidence of a humoral response to influenza virus vaccine by some of our rituximab-treated patients. The observed significantly decreased response might be attributed to a decrease in the amount of B cells after rituximab treatment or to an increase of regulatory T cells. Indeed, previous studies showed a slow and delayed repopulation of CD27+ memory B cells with a significant reduction of their level (to <50%) for more than 2 years.20 On the other hand, a substantial proportion of the patients treated with rituximab did respond to the vaccine despite total B-cell depletion. This might be explained by the presence of plasma cells, which originate from marginal zone B cells less sensitive to rituximab treatment, that continue to secrete antibodies for extended periods of time.21 Another possible explanation is that early differentiating B cells with low-level expression of CD20 “survived” and became the source for the antibodies that had been produced.
In conclusion, this study has confirmed that vaccination against influenza is safe and the findings showed that it generated an appreciable humoral response in patients with RA treated with rituximab, although this response was lower than that seen in non-rituximab-treated patients with RA or in healthy controls. We are aware of the limitations of this study, which include a relatively small number of treated patients and controls. Based on our present data, however, we feel that vaccination against influenza, which is strongly indicated in RA, can also be safely recommended for patients who are being treated with rituximab.
REFERENCES
Footnotes
-
Competing interests: None declared.
-
Ethics approval: Approved by the ethics committees of Tel Aviv Sourasky Medical Centre and the Rambam Health Care Centre.