Article Text

Abstract
Objective: The aim of this study was to determine whether a 3-year treatment with strontium ranelate could delay the progression of spinal osteoarthritis (OA).
Methods: This study was a post-hoc analysis of pooled data from the Spinal Osteoporosis Therapeutic Intervention (SOTI) and TReatment Of Peripheral OSteoporosis (TROPOS) trials performed on 1105 women with osteoporosis and concomitant radiological spinal OA at baseline, and for whom lumbar x-rays were available at baseline and over the 3-year treatment period. The presence and severity of osteophytes, disc space narrowing and sclerosis in the lumbar intervertebral spaces was graded according to a validated method, and an overall OA score was calculated for each intervertebral space. Back pain (measured on a five-point Likert scale only in SOTI) and health-related quality of life (SF-36 questionnaire) were assessed at baseline and after 3 years. Patients who suffered an incident or progressive vertebral fracture during the study were excluded from the analysis.
Results: The proportion of patients with worsening overall spinal OA score was reduced by 42% in the strontium ranelate group, compared with placebo (RR, 0.58; 95% CI, 0.42 to 0.79; p = 0.0005). Significantly more patients in the strontium ranelate group experienced an improvement in back pain after 3 years, compared with placebo (p = 0.03), while no significant difference was observed in terms of health-related quality of life between these patient groups.
Conclusions: The results of this post-hoc analysis suggest that strontium ranelate could reduce the progression of the radiographic features of spinal OA and back pain in women with osteoporosis and prevalent spinal OA.
Statistics from Altmetric.com
Osteoarthritis (OA) is a major cause of disability and is one of the most frequent musculoskeletal disorders.1 For decades, the traditional pharmacological management of OA has been mainly symptomatic, without the support of any well-documented findings on the influence of treatment on disease duration and progression. Drugs with a favourable action on joint structure, which are therefore able to delay the progression of the disease, are termed structure-modifying drugs.2 3 During the last few years, several randomised controlled trials have been performed to assess the structure-modifying effect of various compounds, such as diacerein,4 glucosamine sulphate,5 6 chondroitin sulphate,7 8 and doxycycline.9 However, all these trials specifically addressed lower limb OA (ie, OA of the knee and/or hip), whereas very few data are currently available concerning spinal OA.10 Moreover, the pathophysiology of hip or knee OA differs from that of spinal OA.11
Lumbar disc degeneration is characterised by the presence of osteophytes, endplate sclerosis and disc space narrowing. There is no consensus as to whether this is a variant of general OA or a separate phenomenon, but lumbar spine disc degeneration is often referred to as spinal OA.12 As the severity of radiographic features of spinal OA correlates with increased back pain and decreased health-related quality of life,13 14 any intervention able to delay the progression of spinal OA would be of great interest. Moreover, progression of OA in the spine correlates significantly with progression at other clinical sites such as hand and knee.15
Strontium ranelate is a new drug indicated for the treatment of postmenopausal osteoporosis, which has been proven to be effective in the reduction of vertebral and hip fractures.16 17 Previous studies have provided the preclinical basis for the in vivo testing of strontium ranelate in OA. In human normal and OA chondrocytes that are treated with or without interleukin 1β (IL-1β), strontium ranelate has been shown to stimulate the synthesis of type II collagen and proteoglycan.18 Moreover, 10−3 M strontium ranelate increased the stimulatory effect of insulin-like growth factor (IGF) on proteoglycan synthesis, but did not reverse the inhibitory effect of IL-1β.18 In a 3-year post-hoc analysis of the pool of Spinal Osteoporosis Therapeutic Intervention (SOTI) and TReatment Of Peripheral OSteoporosis (TROPOS) studies, strontium ranelate was also shown to significantly decrease, at all time points, the levels of urinary C-terminal telopeptides of type II collagen (u-CTX-II), a cartilage degradation biomarker with high tissue specificity, compared with placebo.19
The aim of the present study was to assess the efficacy of a 3-year treatment with strontium ranelate in delaying the clinical and structural progression of spinal OA.
METHODS
The present study is a post-hoc analysis of the SOTI and TROPOS trials.16 17 The design and methodology of these two studies have been described fully elsewhere. Briefly, ambulatory postmenopausal women were recruited in 11 European countries and in Australia into two prospective, randomised, double-blind, placebo controlled trials SOTI and TROPOS. Women were eligible for the SOTI trial if they were at least 50 years old, had been postmenopausal for at least 5 years, had at least one prevalent vertebral fracture confirmed by spinal radiography and had a lumbar spine bone mineral density of 0.840 g/cm2 or less. In the TROPOS trial, the eligibility criteria included a femoral neck bone mineral density of 0.600 g/cm2 (corresponding to a T-score <−2.5); age 74 years or older; or age between 70 and 74 years with at least one additional risk factor for fracture. In both studies, patients received either 2 g/day strontium ranelate or placebo, for 3 years. Calcium and vitamin D supplementation was prescribed throughout the course of both trials, the dosage having been determined during a run-in period. All participants gave written informed consent before enrolment and both studies were approved by the relevant institutional review boards.
Lumbar spine vertebral radiographs were evaluated at baseline (month 0 [M0]) and after 3 years (month 36 [M36]) (or M24 in 579 patients for whom M36 radiographs were unavailable or not assessable). In SOTI and TROPOS, only lateral spine radiographs were available. A total of 4224 patients had both a baseline and post-baseline x-ray (fig 1). Four intervertebral spaces (L1–L2, L2–L3, L3–L4 and L4–L5) were examined for the presence and severity of anterior osteophytes (score 0–3), posterior osteophytes (score 0–3), joint space narrowing (score 0–3) and sclerosis (score 0–1), and graded using an atlas according to the method of Lane et al.20 This enabled calculation of an overall OA score for each intervertebral space (graded from 0 to 2) as suggested in the original publication (table 1).20

Of the 4224 patients, 2395 have all lumbar intervertebral spaces assessable (fig 1). All radiographs were read by the same person, who was blinded both to the treatment (strontium ranelate or placebo) and to the time sequence of radiograph acquisition (M0 or M36). The reproducibility (test–retest of 40 radiographs over a 2-week interval) of these qualitative assessments was high, with a Kappa score between 0.85 and 0.92. The reproducibility of sclerosis assessment could not be evaluated because the number of patients with sclerosis was too small.
All patients were also asked to fill in the 36-item Short-Form health survey (SF-36). The SF-36 consists of 36 multiple-choice items comprising eight health domains that describe the overall health-related quality of life as reported by the subject.21 Four dimensions refer to physical health and four others to mental health. All subscales were scored using the Likert scale, with lower scores indicating a perception of poorer health, loss of function and presence of pain. The SF-36 has consistently shown high levels of reliability (test–retest and internal consistency reliability) and validity (content, concurrent, criterion-related, construct and predictive validity).21
As initially planned in the SOTI trial, patients were also asked to reply, at baseline and every 6 months, to one question related to back pain, using a five-point Likert scale: “During the past 4 weeks, have you had pain in the middle or upper part of your back?”. The possibility of response was “not at all, no pain”, “a little”, “moderately”, “quite a bit” and “a great deal”. This question was part of the Qualiost questionnaire.22
Statistical analysis
Our post-hoc analysis was carried out in patients with and without prevalent vertebral fractures, who had prevalent spinal radiographic OA (overall OA score ⩾1 for each intervertebral space). However, as initially planned, patients who had suffered a new vertebral fracture or the worsening of a prevalent fracture during the trial were excluded (in order to avoid interference with the evaluation of spinal interspace and osteophyte formation). The primary efficacy outcome was defined as the proportion of patients in the strontium ranelate and placebo groups in whom the overall OA score increased by at least one grade of severity (in one or more intervtertebral spaces) during the 3-year follow-up period. The statistical difference between the two groups was assessed by the χ2 test. The secondary end point in our study was the difference in the proportion of patients, in the strontium ranelate and placebo groups, with a progression in the score of any single one of the radiographic features (ie, osteophytes, narrowing of disc space, or sclerosis), during the 3-year follow-up. Secondary analyses also included the analysis in the whole study population (with or without prevalent spine OA) but also in patients with at least one intervertebral space with spinal OA. Changes in health-related quality of life scores after 3 years in both groups were assessed using the Mann–Whitney U test. The proportion of patients having experienced an improvement in back pain of at least one point on the Likert scale was calculated in the strontium ranelate and placebo groups, and the statistical difference between the two groups was assessed by the χ2 test. Assessment of health-related quality of life was only performed in patients without new non-vertebral fractures (n = 880) in order to avoid any influence of such fractures on the overall assessment of quality of life. Only the subgroup of patients form the SOTI trial replied to the question about back pain (n = 399). At least, we have looked at the proportion of patients, in each group, with new concomitant treatment taken for their OA.
RESULTS
Baseline characteristics of the study population are summarised in table 2. There were no statistical differences in the baseline characteristics between the strontium ranelate group and the placebo group.
At the end of the 3-year follow-up, 13.4% of patients experienced an increase in overall spinal OA score involving at least one intervertebral space. The proportion of patients with an overall OA score progression was 3.9%, 3.7%, 4.8% and 3.6% for the L1–L2, L2–L3, L3–L4 and L4–L5 intervertebral spaces, respectively.
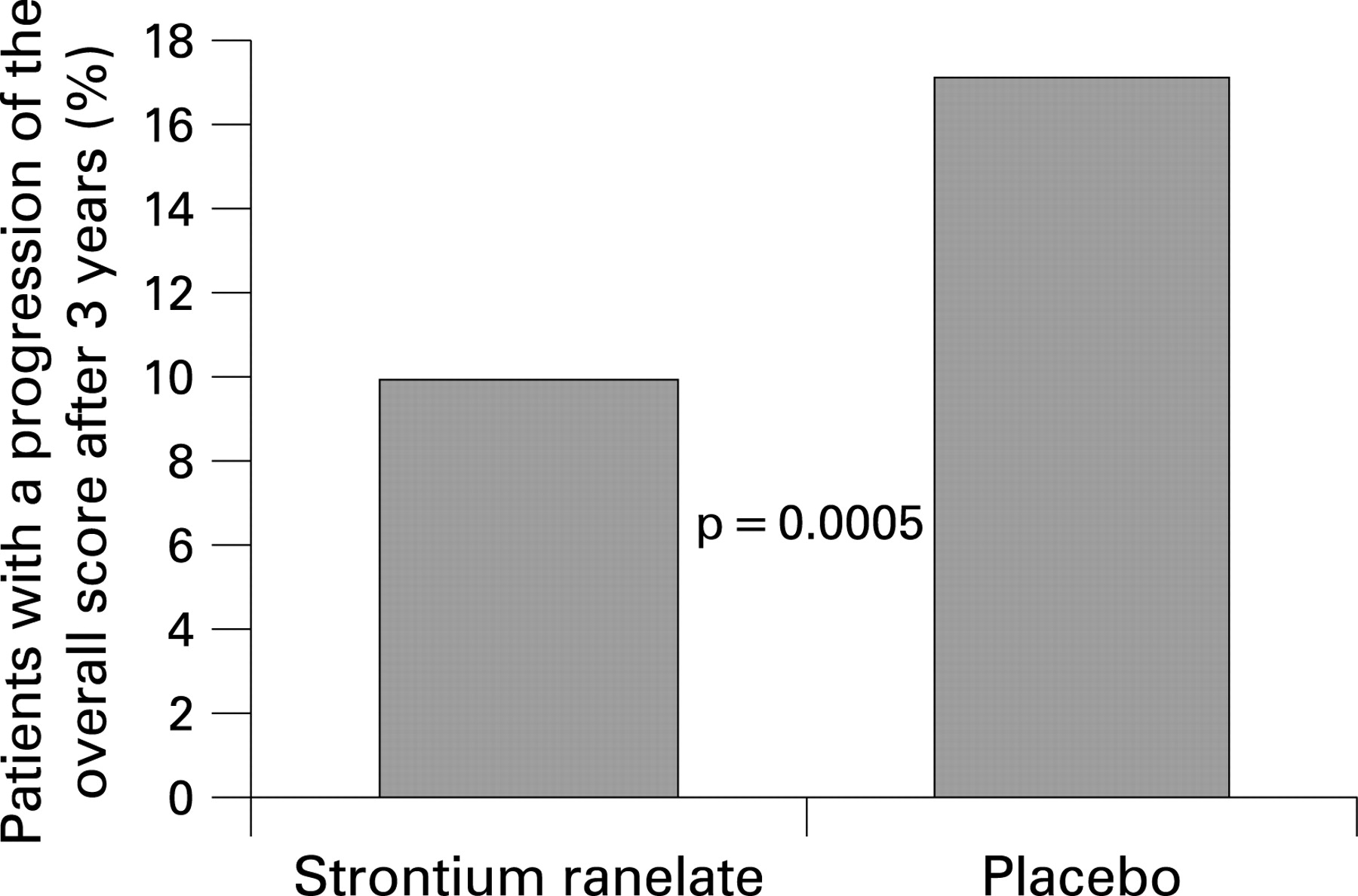
After 3 years of study, only 9.9% in the strontium ranelate group experienced an increase in the overall OA score, versus 17.1% in the placebo group. The proportion of patients with an increase in the overall OA score was reduced by 42% in the strontium ranelate group, compared with placebo (RR, 0.58; 95% CI, 0.42 to 0.79; p = 0.0005) (fig 2).

After 3 years of treatment the number of patients in whom the disc space narrowing score worsened was significantly reduced by 33% in the strontium ranelate group, compared with placebo (RR 0.67; 95% CI, 0.47 to 0.97; p = 0.03). There was also an absolute reduction in the proportion of patients with an increased severity of the osteophyte score in the strontium ranelate group, compared with placebo, but this finding did not reach statistical significance (table 3).
When our analysis is performed in the whole study population (ie, with or without prevalent spine OA; n = 2395), 29.5% in the strontium ranelate group experienced an increase in the overall spinal OA score after 3 years, versus 31.8% in the placebo group. As a matter of fact, strontium ranelate was not able to significantly reduce, compared with placebo, the proportion of patients with an increase in the overall OA score (p = 0.23), disc space narrowing (p = 0.93) or anterior osteophytes (p = 0.43) or posterior osteophytes (p = 0.42). In patients with at least one intervertebral space with OA, the proportion of patients with a progressive OA score was reduced by 9%, compared with placebo, but these results did not reach statistical significance (p = 0.14). The same trends have been shown for disc space narrowing, and anterior and posterior osteophytes (p = 0.78, 0.23 and 0.39, respectively).
After 3 years of treatment, more patients from the strontium ranelate group (84 of 201; 41.8%) experienced an improvement in back pain (decrease by at least one point on the Likert scale) compared with placebo (62 of 198; 31.3%; p = 0.03). Figure 3 show the change in the Likert scale in the placebo and the strontium ranelate group during the 3 years of follow-up. In the whole study population, no significant improvements were observed in any of the items of the SF-36 in the strontium ranelate group, compared with placebo (p-value between 0.18 and 0.93). In particular, there were no changes in the Physical and Mental component scores (p = 0.74 and p = 0.73, respectively).

{kind=link}
{kind=link}
{kind=link}
During the 3 years of follow-up, 10.5% of patients from the placebo group took a treatment related to their OA, compared with 8.3% of the patients from the strontium ranelate group (RR 0.78; 95% CI, 0.55 to 1.12; p = 0.18).
DISCUSSION
This post-hoc analysis suggests that strontium ranelate reduces radiographic spine OA progression in women with osteoporosis and prevalent spinal OA, with or without prevalent vertebral fractures. Concomitantly, a reduction in back pain was observed during the course of the 3-year treatment with strontium ranelate. These findings suggest that strontium ranelate may have symptom- and structure-modifying effects in women with osteoporosis and OA. New, prospective randomised controlled trials in patients with knee OA are currently ongoing to further confirm the potential structure-modifying effect of strontium ranelate.
Various methods have been proposed for assessing the severity of lumbar disc degeneration. Kellgren and Lawrence developed a grading scale.23 Lane et al sought to improve the moderate test–retest agreement and interrater agreement by defining radiographic indices of lumbar disc degeneration to evaluate the individual radiographic features of disc degeneration (ie, anterior osteophytes, posterior osteophytes, joint space narrowing and sclerosis). They were thus able to assign a summary grade derived directly from the evaluation of the selected radiographic features.20 The authors of the original study that validated this method also evaluated the two most frequently affected dorsal intervertebral spaces.20 In the present study, we used this method to assess lumbar spine OA. It should also be pointed out that the method of Lane et al and the views available did not allow assessment of intervertebral posterior articular or facet joints.20
Whether the occurrence of osteophytes and joint space narrowing are separate phenomena or not in the context of lumbar spine disc degeneration, remains unclear.12 In this study, we report a reduction in the progression of joint space narrowing with strontium ranelate, compared with placebo. Data are scarce with regard to therapies modifying the course of OA,4–10 especially in the spine,10 To the best of our knowledge, only one post-hoc analysis has shown that alendronate reduced spinal osteophyte formation in women with osteoporosis (n = 200), but no data on disc space narrowing were provided.10
Strontium ranelate is a drug registered for the treatment of osteoporosis. Other osteoporotic drugs have been tested for their structure-modifying properties in OA, but with conflicting results.10 24 25 Alendronate has been reported to reduce spinal osteophyte formation,10 but two prospective placebo controlled studies found that risedronate failed to significantly reduce the radiographic progression of knee OA (ie, joint space narrowing).24 25
We hypothesise that the effect on joint space narrowing and osteophytes may be due to a direct effect of strontium ranelate on cartilage and bone resulting in endochondral ossification. Although the effects of strontium ranelate on bone have been well described,26 few data are currently available on its effect on cartilage.18 19 In normal chondrocytes and chondrocytes with OA, cultured for 24–72 hours in the presence or absence of strontium ranelate at concentrations ranging from 10–4 to 10–3 M, 1 mM strontium ranelate stimulated human cartilage matrix formation (type II collagen and proteoglycan synthesis), via a direct ionic effect, without stimulating chondroresorption processes.18 Measurement of u-CTX-II was carried out in a subset of 2617 postmenopausal women with osteoporosis from the phase III clinical trial TROPOS.19 A total of 1310 patients was assigned to active treatment for 3 years with strontium ranelate 2 g/day, while 1307 patients received placebo. During the 3-year trial period, at all time points, there was a significant decrease in u-CTX-II of about 15–20% in the strontium ranelate-treated group, compared with placebo (p<0.001).19
It should be pointed out that strontium ranelate seems to be less effective in patients without prevalent OA at each intervertebral space suggesting that this drug could not be considered as a preventive treatment of incident spinal OA.
Our study did not show any significant improvement in health-related quality of life in patients taking strontium ranelate compared with placebo. However, it should be emphasised that the SF-36 questionnaire used in this study was a general questionnaire not OA-specific. The SOTI and TROPOS trials were initially designed to assess the effect of strontium ranelate on fracture incidence. As a consequence, no specific OA questionnaires were used. The only question relating, at least in part, to OA symptoms was the “back pain” question. However, this question was not specifically restricted to the lumbar spine. Moreover, this question was only used in the SOTI trial and not addressed to the whole study population. Nevertheless, more patients in the strontium ranelate group experienced an improvement in back pain than in the placebo group even after excluding patients with incident fractures.
The study we report here has strengths as well as limitations. It was a post-hoc analysis of two prospective placebo controlled 3-year trials, in which the patients included were rigorously followed and radiograph acquisition was fully standardised.16 17 The radiographs were read by a single trained person blinded to the treatment group and the time sequence of radiograph acquisition. However, no data on peripheral OA were available, nor did we assess thoracic spine OA. Moreover, the method of assessment of lumbar spine degeneration did not allow assessment of intervertebral posterior articular joints and lateral osteophytes or direct changes in the disc, which may also contribute to symptoms. At least, our results could not be extrapolated to all patients with lumbar OA as our study population consists of postmenopausal women with osteoporosis.
In conclusion, our findings suggest that strontium ranelate reduces the progression of radiographic spinal OA and back pain in women with osteoporosis and spinal OA. This study has implications not only in the potential treatment of chronic back pain, but also for progression of OA at other sites.
REFERENCES
Footnotes
Funding: The study was supported by a research grant from Servier
Competing interests: None