Article Text

Abstract
Objective: The chemokine CCL2 has been consistently found to be up-regulated in systemic sclerosis. To explore the potential value of serum CCL2 measurement in disease assessment, we have compared CCL2 levels with clinical phenotype and investigated effect of therapy on circulating CCL2.
Methods: Serum samples from a well characterised cohort of 94 systemic sclerosis (SSc) patients, 16 patients with primary Raynaud phenomenon and 11 healthy controls were examined by ELISA. Our cohort of patients included 50 patients with limited cutaneous (lc)SSc (20 with lcSSc alone and 30 with pulmonary arterial hypertension-lcSSc), and 44 with diffuse cutaneous (dc)SSc, 30 of which had early-onset dcSSc.
Results: Serum levels of CCL2 were increased in both major SSc subsets. In early stage dcSSc 18/30 (60%) cases demonstrated markedly elevated CCL2, and this was associated with anti-topoisomerase or anti-RNA polymerase I/III antibody reactivity, and with greater frequency of major organ-based complications. Elevation of CCL2 serum levels in the lcSSc subset was not associated with pulmonary arterial hypertension, although there was a trend for reduction following treatment with prostacyclin analogues or bosentan.
Conclusion: These findings suggest that the CCL2/CCR2 axis is a potential therapeutic target in SSc, particularly in the early dcSSc subset. CCL2 measurement may be useful for risk stratification in early stage disease, but its value in disease monitoring is questionable.
Statistics from Altmetric.com
It is now widely accepted that CCL2 (previously known as monocyte chemoattractant protein-1 or MCP-1) is a potentially important mediator in pathogenesis of systemic sclerosis (scleroderma; SSc). CCL2 belongs to the family of the CC chemokines in which the two cysteines residues are adjacent, whilst the CXC chemokines are characterised by interposition of a single amino acid between the two cysteines residues. CCL2 is a well studied chemokine, known to be produced by a variety of cells and to be a potent chemoattractant for monocytes but also CD4 and CD8 memory T lymphocytes, and NK cells.1 MCP-1 exerts its action mostly trough interaction with CCR2 chemokine receptor. Initial evidence of a role for CCL2 in SSc came from an in vitro study: SSc fibroblasts, but not normal fibroblasts, selectively promoted leucocyte migration across endothelial cell monolayers in vitro and this was blocked by neutralising antibodies against CCL2,2 suggesting a key role in promotion of skin perivascular inflammatory infiltrates. Further work has shown that CCL2 also has a profibrotic effect in SSc. In a recent study we demonstrated that SSc fibroblasts up-regulate CCL2/CCR2 chemokine axis and that CCL2 is involved in the differentiation of fibroblast into myofibroblasts via its receptor CCR2.3 Other recent work suggests that CCL2 profibrotic effects is mediated via the release of interleukin-4 from T cells.4 A number of in vivo studies have also shown up-regulation of CCL2 protein and mRNA in serum, skin and BAL from SSc patients.5–10 However the utility of measuring CCL2 serum levels to evaluate patients with in SSc remains unclear.
Here, we report a cross sectional investigation of circulatory levels in a well characterised cohort of SSc patients to assess whether serum CCL2 could have potential as a surrogate marker of disease severity or be used to monitor treatment response.
PATIENTS AND METHODS
Patients
We studied 94 patients with SSc, 16 patients with primary Raynaud phenomenon and 11 matched healthy controls who entered the study following informed consent. The study was approved by the institutional local ethics committee. All patients fulfilled the American College of Rheumatology (ACR) preliminary criteria for the classification of SSc.11 This SSc cohort included 50 patients limited cutaneous SSc (lcSSc) (including 30 with pulmonary arterial hypertension; PAH), 44 diffuse cutaneous SSc (dcSSc) including 30 patients with early diffuse cutaneous SSc (dcSSc), defined as disease within 2 years from first non-Raynaud manifestation.12 To evaluate organ involvement we adopted the recently published consensus core set variables for SSc studies.13 Therefore, skin involvement was assessed using the modified Rodnan skin score, gastrointestinal involvement was defined symptomatically. Restrictive pattern of pulmonary function abnormalities with reduction in FVC and DLCO below 80% of predicted value (based on age, sex, height and ethnic origin) was used as main indication of lung involvement, although this was generally confirmed by high-resolution computed tomography of the chest. A diagnosis of pulmonary arterial hypertension was suspected when estimated RVSP was above 35 mmHg by Doppler echocardiography, and was confirmed by right heart catheterisation. Cardiac involvement was considered present if any significant conduction defects were found on electrocardiogram, or impaired left ventricular function or haemodynamically significant pericardial effusion were detected by echocardiography. Above fourfold elevation of creatinine kinase accompanied by the clinical finding of proximal weakness defined muscular involvement, whilst renal involvement was determined by history of definite scleroderma renal crisis or significant impairment in creatinine clearance (less than 65 ml/min).
Demographic, clinical and serological characteristics of the patients studied are summarised in table 1. The differences in pattern of internal organ involvement and serological profile between groups are attributable to different stages and subsets of the disease. Patients with later stage dcSSc had generally been previously treated with immunomodulatory therapy including anti-thymocyte globulin, mycophenolate mofetil or cyclophosphamide, but no cases were receiving corticosteroids at doses greater than 10 mg prednisolone daily. Patients with lcSSc were not on immunomodulatory agents or corticosteroids. All SSc cases received treatment for Raynaud phenomenon with one or more vasodilator agent including calcium channel blockers, angiotensin-converting enzyme (ACE) inhibitors or angiotensin receptor blocking drugs.
Measurements of CCL2 serum levels by ELISA
Serum samples were taken from all patients with SSc, following consent, when they attended the Rheumatology department for clinical review, and were then stored at −20°C over a short period of time. Serum CCL2 was measured using specific ELISA kit (Quantikine, R&D, Oxford, UK). All samples were tested in duplicate, the minimum detectable dose of CCL2 was less than 5 pg/ml. A standard curve was used as reference, this was obtained by increasing dilutions of a stock solution provided by manufacturer to obtain eight different concentrations, each of which was also tested in duplicate. Briefly, serum samples were diluted in calibrator diluent provided by manufacturer to achieve a twofold dilution, 200 μl of each sample was added to 50 μl of assay diluent into each well of a 96-well microplate that was pre-coated with monoclonal antibody specific for CCL2. After 2 h incubation at room temperature, each well was thoroughly washed three times using an automated ELISA plate washer. 200 μl of CCL2 conjugate were then added to each well and again incubated for 2 h. After washing, 200 μl of substrate solution were added and incubated for 30 min. 50 μl of Stop solution were then added and the optical density of each well was determined using a microplate reader set to 450 nm according to the manufacturer’s instructions.
Statistical analysis
For quantitative variables, the mean (SEM) results from replicate samples were compared by Student t test. A χ2 test was used for categorical data. Statistical significance was inferred by a p value less than 0.05.
RESULTS
Clinical and serological features associated with elevated CCL2 in SSc
Overall CCL2 serum levels were greatly and significantly elevated in SSc patients (359 (27) pg/ml, mean (SEM)) compared to controls (132 (26) pg/ml) (p<0.05) and patients with isolated Raynaud phenomenon (154 (17) pg/ml) (p<0.05). Although CCL2 serum levels were higher in the dcSSc subset (478 (47) pg/ml) than in the lcSSc subset (260.97 (20) pg/ml) there was no statistically significant difference between the two groups. In addition, we found no difference between isolated Raynaud phenomenon patient’s levels (154 (17) pg/ml) and healthy controls (132 (26) pg/ml), suggesting that elevated CCL2 serum levels do not occur in isolated Raynaud phenomenon (fig 1).
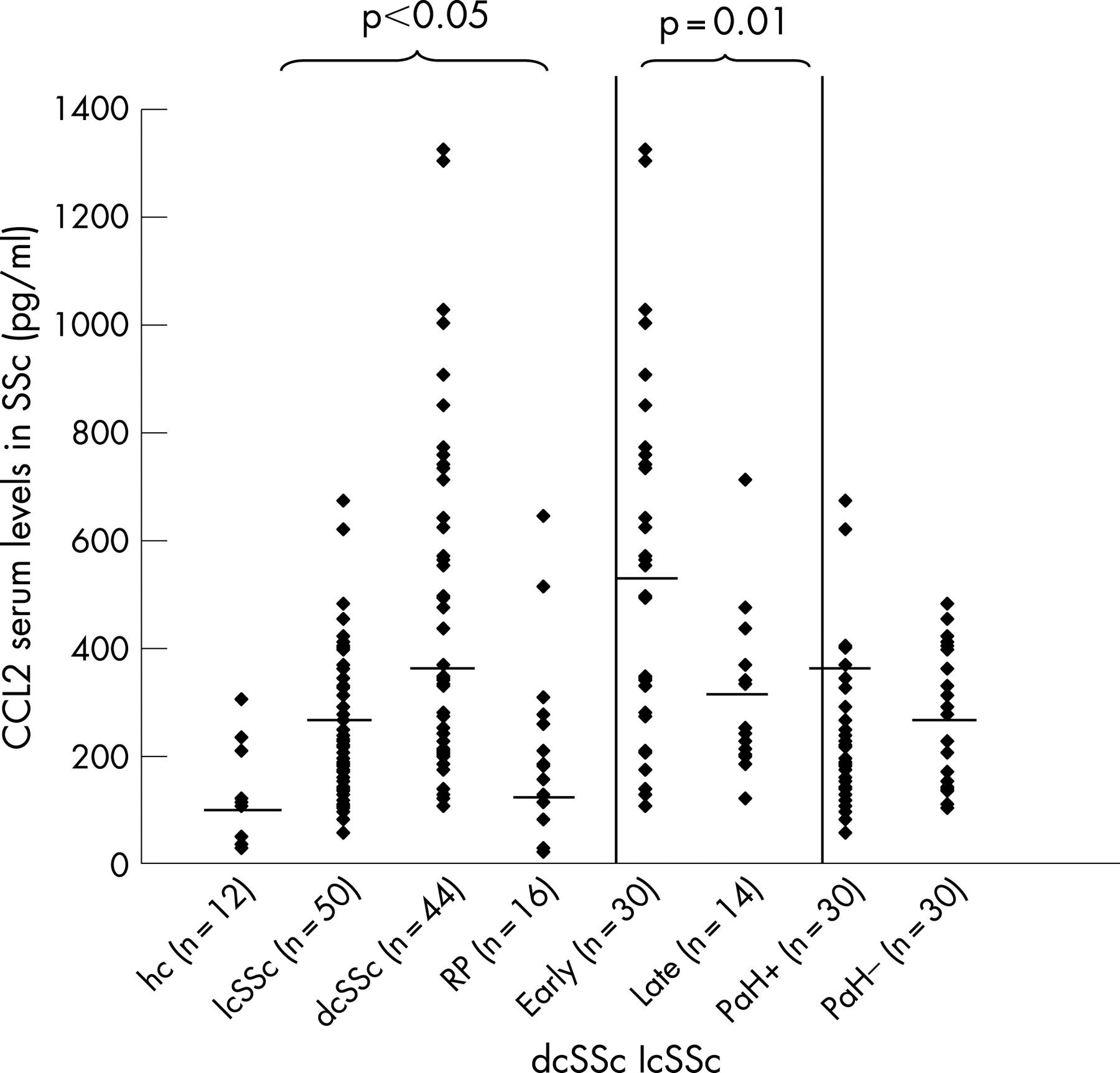
To better understand the relationship between CCL2 serum levels and stage and severity we focused on patients with dcSSc. We divided this cohort in patients who had early diffuse cutaneous SSc, defined as disease within 2 years from first non-Raynaud manifestations (6) (n = 30) and patients with late dcSSc (n = 14). CCL2 serum levels in the early disease group were nearly twofold higher (557 (61) pg/ml) than late stage dcSSc (307 (41) pg/ml) (p = 0.01) (fig 1). These data are in keeping with our observation of up-regulation of CCL2 and CCR2 in the skin from early dcSSc patients3 and together support a potential role for CCL2 in the pathogenesis at an early stage.
However, we noted substantial variability in CCL2 levels in the early dcSSc cohort. To explain the significance of this we segregated the early dcSSc cohort on the basis of their serum levels. Levels higher than three standard deviations above the mean for healthy controls were considered markedly elevated. Using this definition, 18 patients (60%) with significantly elevated CCL2 in serum were compared to those with lower serum levels of CCL2 (n = 12). Many clinical and demographic variables were similar between these two groups, including duration of Raynaud phenomenon and time in months from SSc onset. Internal organs involvement, in particular pulmonary fibrosis, pulmonary arterial hypertension and cardiac involvement, were at least twice as more frequent in the high CCL2 group, although, and probably due to the unavoidably small numbers in this subset analysis, this difference was not statistically significant (table 2). This observation was supported by higher frequency of the hallmark dcSSc associated autoantibodies anti-topoisomerase-1 and anti-RNA polymerase I/III in the high CCL2 group (p<0.05). When patients with anti- topoisomerase-1 and anti RNA polymerase I and III, (both independently associated with poor outcome14 but also mutually exclusive, were combined the association with CCL2 serum levels was even stronger (p<0.025). This suggests that the association of CCL2 is likely to be with outcome rather than with either of these two hallmark reactivities.14
Elevated CCL2 levels do not associate with PAH in lcSSc but may fall with treatment
Elevated CCL2 serum levels have been reported in patients with idiopathic pulmonary hypertension.15 In order to assess whether the elevation of CCL2 serum levels in the lcSSc subset was attributable to pulmonary arterial hypertension we analysed this subset. In this subgroup, 20 patients had lcSSc alone and 30 lcSSc with associated pulmonary arterial hypertension (PAH), proven on Right heart catheter (table 3). CCL2 serum levels were higher in patients with lcSSc and PAH (317 (26) pg/ml) when compared with patients with lcSSc alone (267 (28) pg/m) but this difference did not reach statistical significance (fig 1). We then analysed CCL2 serum levels in the subset with lcSSc associated- PAH (n = 10) following administration of licensed therapy for advanced PAH including prostacylin analogue or endothelin-1 receptor antagonists. Following initiation of treatment there was a fall in serum levels in 12/17 patients with mean serum of 205 (25) pg/ml at the baseline and 162 (61) pg/ml post treatment but this change did not reach statistical significance (fig 2). However, we found a clear inverse correlation between serial CCL2 serum levels and 6 min walk time in two patients undergoing treatment suggesting that in a well defined subset of patients it could be used as marker of pulmonary vascular disease activity (data not shown). Similarly, we observed a fall in CCL2 serum levels following iloprost therapy in 5/7 patients with SSc but no pulmonary hypertension, although there was no statistically significant difference overall (fig 2).

{kind=link}
{kind=link}
DISCUSSION
It is likely that clinical heterogeneity within and between major subsets of SSc arises through different patterns of altered intercellular cross-talk involving the vasculature, the immune system and connective tissue fibroblasts. Mediators that are produced by or act upon these cell types are key factors in pathogenesis. Our study suggests a role for CCL2 in the pathogenesis of SSc, moreover it suggests that patients expressing high serum levels at an early stage in the disease may be more likely to develop cardiovascular and respiratory involvement. In the present study we assess the utility of CCL2 serum levels in patients risk stratification. High levels of CCL2 expression overall in SSc, including late dcSSc and lcSSc imply that its overexpression may be determined by a common event in pathogenesis that occurs in all SSc cases. However, CCL2 serum levels were highest in early dcSSc suggesting that CCL2 overexpression may have a specific role in this subset. We defined elevated CCL2 by levels more than three standard deviations above the mean level for healthy individuals of similar age and gender. This is a more rigorous definition than was applied in one previous study in SSc,10 and so our results confirm the previously reported association of high CCL2 serum levels and pulmonary fibrosis. In another study high serum CCL2 levels were associated with renal involvement in keeping with our findings.16 Drawing analogy with other inflammatory diseases it is likely that genetically determined qualitative or quantitative differences in cytokine ligand or receptor expression influence the disease phenotype. Single nucleotide polymorphisms in the promoter region of CCL2 gene have been described that associate with higher protein expression levels.17 This appears to be clinically relevant in context of several inflammatory diseases.18–20 Recently a study on a small cohort of SSc patients has also shown an association of CCL2 single nucleotide polymorphisms (-2518G/A) with SSc.20 Support for a genetic basis comes from studies of hallmark autoantibodies in SSc, which are strongly linked to HLA haplotypes but which also have characteristic clinical associations. For example, both anti-topoisomerase 1 and anti-RNA polymerase I/III antibodies are associated with the diffuse cutaneous subset of SSc in addition anti-topoisomerase 1 strongest association is with interstitial lung disease while anti-RNA polymerase I/III is associated with renal involvement independent of subset.14 It seems unlikely that CCL2 reflects renal disease, based upon our cohort, but lung fibrosis does occur more frequently in the high CCL2 group. It remains possible that the higher levels reflect a more progressive form of scleroderma, and that complications will develop later in the low CCL2 expressing group. In our study CCL2 overexpression is associated with patients expressing these mutually exclusive hallmark reactivities combined and this implies an association of CCL2 with poor outcome rather than with either of these antibodies. Clarification of this will depend upon future longitudinal assessment of cases.
We also explored the hypothesis that CCL2 elevation may reflect vascular disease or damage. CCL2 is in fact overexpressed in patients with idiopathic pulmonary hypertension and CCL2 antagonists have been found to ameliorate disease in animal models.22 23 Our study did not show a significant overexpression of CCL2 serum levels in patents with PAH and LcSSc vs patients with lcSSc alone, suggesting that elevation of this chemokine reflects disease at multiple sites and the fibrotic component of the disease. However, the decline in CCL2 serum levels following therapy for pulmonary arterial hypertension suggests a role for CCL2 in the pathogenesis of this complication, and the role of measuring serial serum levels to monitor response to treatment needs to be further evaluated. However, it is unlikely that CCL2 will prove to be a sensitive and specific marker as the N-terminal pro-brain natriuretic peptide, which has been shown to associate with clinical and haemodynamic features of PAH in SSc and also reflect outcome or treatment response.24 Elevation of CCL2 in the serum of a subgroup of cases of early dcSSc is an important finding in our study. There was association with autoantibodies that may predict poor outcome in SSc. A longitudinal study of early dcSSc patients with high levels of CCL2 will help to define if this marker has any prognostic value as a severity marker in this particular subset of the disease, and more comprehensive genetic studies should address whether these differences are associated with particular single nucleotide polymorphisms in the CCL2 gene, as has been suggested in other diseases
In conclusion, our data suggest that the CCL2/CCR2 axis remains a logical target for therapy in selected patients especially those cases of early dcSSc with high CCL2 levels and agents that attenuate CCL2 activity may be useful. Future work is needed to assess whether CCL2 serum or tissue levels may help to predict which patients are likely to benefit from such therapeutic intervention. However, it seems unlikely that CCL-2 levels will offer additional information for diagnosis and follow-up of SSc cases with suspected or proven PAH or lung fibrosis compared with other promising serological markers such as N-terminal pro-BNP or KL-6.
Acknowledgments
The authors thank the Arthritis Research Campaign for funding this work.
REFERENCES
Footnotes
-
Competing interests: None declared