Article Text

Abstract
Background: The Combinatietherapie Bij Reumatoide Artritis (COBRA) trial has proved that combination therapy with prednisolone, methotrexate and sulphasalazine is superior to sulphasalazine monotherapy in suppressing disease activity and radiological progression of early rheumatoid arthritis (RA). In addition, 5 years of follow-up proved that COBRA therapy results in sustained reduction of the rate of radiological progression. Despite this evidence, Dutch rheumatologists seem reluctant to prescribe COBRA therapy.
Objective: To explore the reasons for the reluctance in Dutch rheumatologists to prescribe COBRA therapy.
Methods: A short structured questionnaire based on social–psychological theories of behaviour was sent to all Dutch rheumatologists (n = 230).
Results: The response rate was 50%. COBRA therapy was perceived as both effective and safe, but complex to administer. Furthermore, rheumatologists expressed their concern about the large number of pills that had to be taken, the side effects of high-dose prednisolone and the low dose of methotrexate. Although the average attitude towards the COBRA therapy was slightly positive (above the neutral point), the majority of responding rheumatologists had a negative intention (below the neutral point) to prescribe COBRA therapy in the near future.
Conclusion: The reluctance of Dutch rheumatologists to prescribe effective COBRA therapy may be due to perceptions of complexity of the treatment schedule and negative patient-related consequences of the therapy.
- COBRA, Combinatietherapie Bij Reumatoide Artritis
- MTX, methotrexate
- RA, rheumatoid arthritis
- SSZ, sulphasalazine
Statistics from Altmetric.com
- COBRA, Combinatietherapie Bij Reumatoide Artritis
- MTX, methotrexate
- RA, rheumatoid arthritis
- SSZ, sulphasalazine
In the randomised, double-blind, multicentre Combinatietherapie Bij Reumatoide Artritis (COBRA) trial, published in 1997, 155 patients with early rheumatoid arthritis (RA) were treated with either sulphasalazine (SSZ) monotherapy or COBRA combination therapy, comprising SSZ (2 g/day), methotrexate (MTX; 7.5 mg/week) and prednisolone (initially 60 mg/day, tapered in 6-weekly steps to 7.5 mg/day; fig 1).

Combinatietherapie Bij Reumatoide Artritis (COBRA) treatment schedule.
The COBRA combination was found to be superior to SSZ monotherapy in suppressing disease activity and radiological progression of early RA.1 After a 5-year follow-up, the COBRA therapy resulted in a sustained reduction in the rate of radiological progression, despite similar treatment and activity of the disease in the follow-up period,2 and was proven cost-effective because of enhanced efficacy at lower or equal direct costs compared with SSZ monotherapy.3,4
In addition, the Behandel Strategieen trial, comparing clinical and radiographic outcomes of four treatment strategies, showed equal effectiveness of the COBRA strategy in the initial combination therapy with infliximab. This resulted in earlier functional improvement and less radiographic damage after 1 year, compared with sequential monotherapy or step-up combination therapy.5
Despite the evidence on short- and long-term effectiveness and safety of the COBRA combination therapy and its cost effectiveness, it appears that this therapy is seldom prescribed in clinical practice.
This study was designed to explore the use of COBRA therapy in Dutch clinical practice and to explain the reservation of Dutch rheumatologists towards its prescription.
METHODS
A short structured questionnaire was designed with questions partially based on the social–psychological theory of planned behaviour. This theory predicts behaviour (in our case, prescribing COBRA therapy) through behavioural intention, which in turn is explained through attitude towards the behaviour, the influence of the social environment and the self-perceived control over the behaviour.6,7
The first question probed familiarity with COBRA therapy by asking respondents whether they had heard of COBRA therapy, and whether or not they had ever used this therapy in their clinical practice or in trials.
The attitude towards prescribing the COBRA therapy was measured through seven word pairs (ineffective vs effective; unsafe vs safe; complex vs simple; patient-unfriendly vs patient-friendly; unsympathetic vs sympathetic; unnecessary vs necessary; bad vs good) on a 7-point “Likert scale”. Negatively worded items were recoded for analysis. Thus, a score of 1 indicates a negative attitude towards prescription of COBRA therapy and a score of 7 indicates a positive attitude towards prescribing COBRA therapy. Overall attitude was calculated as the grand mean of all the individual items.
Intention was measured through a single item querying the likelihood of the respondent prescribing COBRA therapy to a newly diagnosed patient with RA within the next 6 months (1 “not at all likely” to 7 “very likely”). Questionnaires were sent by surface and by electronic mail to all Dutch rheumatologists and rheumatologists-in-training, and to members of the Dutch Society of Rheumatology (n = 230).
Analyses
Results were statistically analysed by parametrical (Student’s t) and non-parametrical (Mann–Whitney U) tests wherever applicable, and linear stepwise regression analysis was used to explore relationships between variables. Remarks written on the questionnaire were categorised by one investigator and judged by two other investigators.
RESULTS
The response to the questionnaire was 50% (n = 116). All respondents were familiar with COBRA therapy: two-thirds had used it in clinical practice, and the remainder had participated in a trial. Thirteen respondents were trainees. Overall, the attitude towards prescribing COBRA therapy was slightly positive (table 1).
Dutch rheumatologists’ attitude towards prescribing COBRA therapy
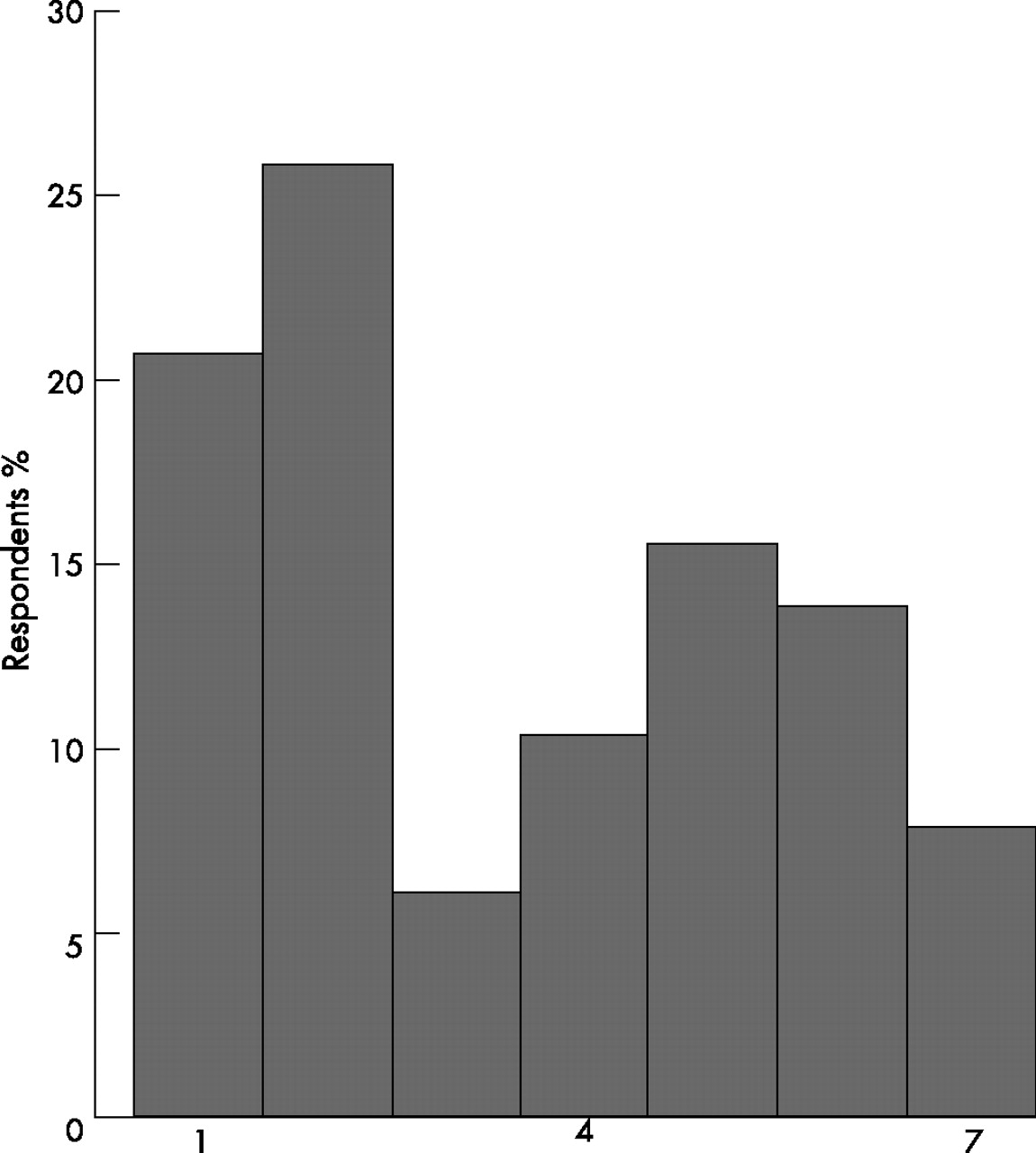
The high score of 6 shows that respondents were convinced of the effectiveness of COBRA therapy. All other items scored a slight plus, except for a slight minus on simplicity and a neutral on patient friendliness. All items except patient friendliness scored significantly differently from the neutral point 4. In contrast to these findings, the mean score on intention to prescribe the COBRA therapy to patients with early RA in the near future remained slightly negative. Distribution of items was reasonably normal, except for items complexity, which showed some skewness towards lower values (data not shown), and intention, which showed a bimodal distribution (fig 2).

{kind=link}
{kind=link}
How likely is it that you will prescribe Combinatietherapie Bij Reumatoide (COBRA) therapy to a patient in the coming 6 months? (1 “not at all likely” to 7 “very likely”).
Respondents experienced with COBRA therapy scored significantly higher on both attitude and intention compared with “unexperienced” respondents: 4.7 vs 4.3 and 4.7 vs 4.1 (p<0.001). Stepwise regression analysis showed that the variance in intention to prescribe COBRA was significantly explained by attitude towards prescribing COBRA therapy (R2change = 0.15; p = 0.002) and by prior experience with COBRA therapy (R2change = 0.15; p = 0.001). There were no significant differences between trainees and rheumatologists, but the number of trainees responding was very small.
Table 2 shows that the remarks written on the questionnaires could be divided into six categories.
Remarks of respondents written on the questionnaire
The most prevalent remark was the preference of respondents for using a “mild” or “revised” COBRA therapy. The suggestions and adjustments that respondents made to the therapy were the exclusion of SSZ from the medication strategy (n = 5), the use of higher doses of MTX (n = 5) or continuation of the therapy after 40 weeks with MTX instead of SSZ (n = 4). Remarks about high-dose prednisolone were mainly focused on the unpleasant side effects for patients, the suggestion that a lower dose might also suffice, and the preference for injections instead of oral steroids.
DISCUSSION
This study explored the reluctance of Dutch rheumatologists to prescribe COBRA therapy. Although most scores (except effectiveness) were on average near neutral, we found a discrepancy between a positive attitude and a negative intention, with a cluster of respondents who emphatically did not want to prescribe COBRA therapy.
Some clues to explain this come from the other items and, especially, the added remarks. The schedule is perceived as somewhat complex, and several rheumatologists appear to prefer their own mild/revised COBRA therapy in daily practice. In addition, respondents criticise the inclusion of SSZ in the COBRA treatment schedule and the dosage of MTX, which, at 7.5 mg weekly, is low by current standards. Finally, several remarks are aimed at prednisolone: a preference for injections, and the perception that patients object to high-dose prednisolone and a large amount of pills. The more positive attitude and intention of rheumatologists who had experience with COBRA therapy (compared with “unexposed” rheumatologists) suggests that encouraging such practical experience is a feasible way to increase implementation of COBRA in daily practice.
However, this study did not measure social norm and perceived behavioural control, important factors in explaining behaviour. Because of the finding that the COBRA therapy was perceived as slightly complex, rheumatologists might find it difficult to prescribe this therapy (perceived behavioural control). Furthermore, the perception of the behaviour of colleagues may also influence the decision on whether or not to prescribe a therapy that not many others do (social influence).
Another limitation of this study is the selection of rheumatologists. Although all Dutch rheumatologists and trainees were invited to respond, only 50% did so. This could introduce bias in terms of the “population” mean opinion of Dutch rheumatologists. However, more than enough material was obtained in this exploratory first step. The next step is in-depth exploration of physicians’ and patients’ opinions via focus groups and interviews (currently ongoing, to be reported separately). This information will be crucial in designing an implementation project addressing the problems that respondents have with prescribing the COBRA therapy in their daily practice.
Acknowledgments
This study was supported by the Dutch Arthritis Association.
Footnotes
-
Competing interests: None declared.
-
Published Online First 28 March 2007