Article Text

Abstract
Objective: To investigate changes in the levels of circulating cytokines with a focus on the Th1/Th2 balance during and after pregnancy in patients with rheumatoid arthritis (RA), juvenile idiopathic arthritis (JIA), and ankylosing spondylitis (AS).
Methods: Plasma and serum samples of 34 pregnant patients, 19 with RA, 6 with JIA, and 9 with AS, and of 30 healthy pregnant women, 20 non-pregnant patients, and 10 non-pregnant healthy women were analysed for levels of interferon γ (IFNγ), interleukin (IL) 1β, IL10, IL1 receptor antagonist (IL1Ra), soluble tumour necrosis factor receptor (sTNFR), and soluble CD30 (sCD30) by ELISA. Clinical assessment and blood sampling in pregnant women was done once in each trimester and 6, 12, and 24 weeks post partum. Disease activity in the patients was evaluated by validated clinical instruments and correlated with circulating levels of cytokines.
Results: Low levels of IL10 were found sporadically, whereas IFNγ and IL1β were below detection level in the samples tested. Significantly higher concentrations of sTNFR and IL1Ra were measured in pregnant than in non-pregnant subjects. An increase of IL1Ra from the second to the third trimester correlated with improvement of disease activity in patients with RA and AS. Compared with non-pregnant patients and the other pregnant women, patients with RA showed markedly raised levels of sCD30 during pregnancy.
Conclusions: IFNγ and IL10, markers of a Th1 and Th2 response, respectively, were either low or undetectable in the cohorts analysed. The increase of cytokine inhibitors IL1Ra and sTNFR was related to pregnancy and was independent of an underlying disease. These anti-inflammatory mediators seem to affect disease activity.
- AS, ankylosing spondylitis
- BASDAI, Bath Ankylosing Spondylitis Activity Index
- CRP, C reactive protein
- ELISA, enzyme linked immunosorbent assay
- IFNγ, interferon γ
- IL, interleukin
- IL1Ra, interleukin 1 receptor antagonist
- JIA, juvenile idiopathic arthritis
- NSAIDs, non-steroidal anti-inflammatory drugs
- PGA, physician’s global assessment
- RA, rheumatoid arthritis
- RADAI, RA Disease Activity Index
- sCD30, soluble CD30
- sTNFR, soluble tumour necrosis factor receptor
- TNF, tumour necrosis factor
- cytokines
- immune response
- pregnancy
- rheumatic disease
Statistics from Altmetric.com
- AS, ankylosing spondylitis
- BASDAI, Bath Ankylosing Spondylitis Activity Index
- CRP, C reactive protein
- ELISA, enzyme linked immunosorbent assay
- IFNγ, interferon γ
- IL, interleukin
- IL1Ra, interleukin 1 receptor antagonist
- JIA, juvenile idiopathic arthritis
- NSAIDs, non-steroidal anti-inflammatory drugs
- PGA, physician’s global assessment
- RA, rheumatoid arthritis
- RADAI, RA Disease Activity Index
- sCD30, soluble CD30
- sTNFR, soluble tumour necrosis factor receptor
- TNF, tumour necrosis factor
Several autoimmune, rheumatic diseases modulate disease activity during and after pregnancy. Rheumatoid arthritis (RA) improves in the majority of patients,1 whereas ankylosing spondylitis (AS) remains active and is mitigated only in late pregnancy.2 Aggravation of disease symptoms after delivery is commonly seen in both diseases and occurs, in general, within the first 6 months post partum. Pregnancy induces changes in the maternal immune system in order to protect the fetus from immunological attack by the mother. Research over the past decade has indicated that no general immunosuppression takes place in the maternal system, rather a shift from a prevailing Th1 response to a type Th2 response.3 CD4+ T cells can be divided into two subsets: one is the T helper 1 type characterised by production of interferon γ (IFNγ), interleukin (IL) 12, tumour necrosis factor β (TNFβ), and IL2 and involved in cell mediated immunity. The other T cell subset consists of Th2 committed cells, which mainly produce IL4, IL10, and IL13, thereby enhancing humoral immunity. The immunological changes taking place during and after pregnancy may modulate disease symptoms according to the underlying pathophysiology of the disease in question. In RA, a Th1-type immune response is predominant, whereas a Th0 or Th2 type prevails in AS.4
IFNγ is a major contributor to a Th1 immune response, up regulating Th1 cell differentiation and inhibiting Th2 cell development. IL1β and TNFα are proinflammatory cytokines that contribute to synovitis and joint destruction in both RA and AS.5–7 IL10 down regulates production of proinflammatory cytokines by Th1 cells and macrophages. In pregnancy, IL10 counteracts pregnancy related disorders, such as fetal growth restriction as well as fetal death and pre-eclampsia.3,8 The immune modulating activities of cytokines are also regulated by soluble cytokine receptors like TNF receptor (TNFR) which can buffer the biological effects of TNFα.9 Another natural inhibitory mechanism involves the blocking of receptor binding by cytokine receptor antagonists like IL1Ra.10
The CD30 receptor belongs to the TNF/nerve growth factor receptor superfamily. CD30 is normally expressed on a subset of activated T cells producing Th2-type cytokines.11 The soluble form of CD30 (sCD30) released upon T cell activation by proteolytic cleavage is regarded as a measure of CD30 turnover. Raised levels of sCD30 have been detected in Th2 dominated diseases like systemic lupus erythematosus,12 systemic sclerosis,13 ulcerative colitis,14 and allergic disorders.15
The objective of this study was to investigate changes of circulating cytokines and regulatory molecules with a focus on the Th1/Th2 balance during and after pregnancy in patients and healthy controls. By analysing the type of cytokine pattern we sought to determine if the different clinical responses to pregnancy were related to a particular immune response.
PATIENTS AND METHODS
Patients and samples
The longitudinal prospective study was performed at the Department of Rheumatology and Clinical Immunology/Allergology of the University Hospital of Bern after approval by the institutional review board of Bern. Additional sequential serum samples (collected after centrifugation of venous blood) from 10 pregnant patients with RA and 6 patients with juvenile idiopathic arthritis (JIA), and from 8 healthy pregnant women were provided by Professor JL Nelson, Seattle, USA and by Dr G Hebisch, Department of Gynaecology at the University Hospital of Zürich, respectively.
A total of 34 pregnant patients, 19 with RA, 6 with JIA, 9 with AS (10 pregnancies), and 30 healthy pregnant women matched for age were included in the study. Ten non-pregnant, age matched healthy women were included to get the background measurements for the age group, and 9 non-pregnant patients with RA and 11 patients with AS provided background data of a chronic, inflammatory disease. Patients with RA fulfilled the American College of Rheumatology criteria,16 and patients with AS the criteria of the European Spondylarthropathy Study Group (ESSG).17 The mean age of pregnant patients was 31 (range 21–38), of pregnant healthy women 33 (21–40), of non-pregnant patients 30 (24–37), and of non-pregnant controls 29 years (range 24–35). At the time of blood sampling, none of the participating women had any known infections or was close to labour.
All pregnant women recruited at the University Hospital of Bern were assessed by clinical examination and measurement of C reactive protein (CRP) at each trimester of pregnancy: gestational week 9–12, gestational week 20–23, gestational week 32–34, and 6, 12, and 24 weeks post partum. Four patients with RA, four with AS, and three healthy women also had blood sampling 8–12 weeks before the index pregnancy. Clinical evaluation was carried out by the RA Disease Activity Index (RADAI) and the tender and swollen joint count18 in patients with RA and by the Bath Ankylosing Spondylitis Activity Index (BASDAI)19 in patients with AS. Overall disease activity was measured by the physician’s global assessment (PGA, a visual analogue scale from 0 to 100).20 A remission of the disease during pregnancy was defined as a PGA score of 0, improvement as a decrease of PGA of 20, and active disease as a PGA score >20. In all pregnant patients recruited by Dr JL Nelson, disease activity was expressed in three ways: remitted, improved, or active. The six patients with JIA had polyarticular disease and five were positive for rheumatoid factor. Their serum samples were analysed together with those of patients with RA.
Drug treatment during pregnancy
At study entry six patients were receiving intramuscular gold or sulfasalazine, seven low dose prednisone, and eight non-steroidal anti-inflammatory drugs (NSAIDs). At the third trimester, two were receiving sulfasalazine, three prednisone, and five NSAIDs. At the post partum aggravation, 28 patients received one of the mentioned drugs or anti-TNF therapy.
Enzyme linked immunosorbent assay (ELISA)
Venous blood samples obtained from patients and controls were drawn into tubes containing 3.8% trisodium citrate as an anticoagulant. Plasma was prepared by centrifugation for 15 minutes and aliquots were stored at −80C. Samples were thawed and assayed for levels of sTNFR (p75), IL1Ra, and sCD30 by solid phase sandwich ELISA. The minimal detectable concentrations for the sTNFR ELISA (R&D Systems, Minneapolis, USA) and the IL1Ra ELISA (R&D Systems, Minneapolis, USA) were <1.0 pg/ml and 14 pg/ml, respectively. The instant ELISA for sCD30 (Bender MedSystems, Vienna, Austria) had a detection limit of 0.5 U/ml. ELISA kits were also used to detect levels of IFNγ (Biosource International, Europe, Nivelle, Belgium), IL1β (R&D Systems, Minneapolis, USA), and IL10 (Immunotech, Marseille, France) in the plasma. For these last assays the detection limits were as follows: <4 pg/ml, <1 pg/ml, and 5 pg/ml. Intra-assay precision and interassay precision of all ELISAs applied were <10%. All cytokine assays were performed according to the manufacturer’s instructions.
Statistics
Data were analysed using the SPSS 11.0 software package. The associations between clinical measurements of disease activity and the TNFR, IL1Ra, and sCD30, respectively, were analysed using Spearman’s rank correlation. Correlation was considered strong if the correlation coefficient was ⩾0.70, moderate to substantial between 0.30 and 0.70, and weak if ⩽0.30. We applied the Mann-Whitney U test to compare the median levels of the cytokines measured in pregnant subjects with those of the non-pregnant controls. To analyse the longitudinal change of cytokines we used the Wilcoxon test for paired data. Graphical presentation of the summary scores are given in box plots displaying the median and 25th–75th centiles and the range of values. Values of p<0.05 were considered significant.
RESULTS
Patients’ characteristics and clinical outcome during pregnancy
All patients and healthy women had uncomplicated pregnancies with delivery of healthy children between 36 and 40 weeks of gestation. During pregnancy, 17 patients with RA and five with JIA improved, but the disease remained active in the remaining three patients. Except for two patients with AS with minimal disease activity at study entry, a varying disease course with active disease in the first and second trimester was observed in eight pregnancies. Four patients with AS improved in the third trimester. Aggravation of disease symptoms occurred in 22 patients with RA/JIA and in eight patients with AS between 6 and 12 weeks after delivery.
Cytokines and cytokine receptors
Low levels of IL10 were sporadically found in five samples, whereas IFNγ and IL1β were below detection levels in the samples tested. The sTNFR values of two patients with RA measured in the postpartum period were excluded because they had started anti-TNF treatment.
Circulating levels of sTNFR, IL1Ra, and sCD30 in pregnant women compared with non-pregnant women
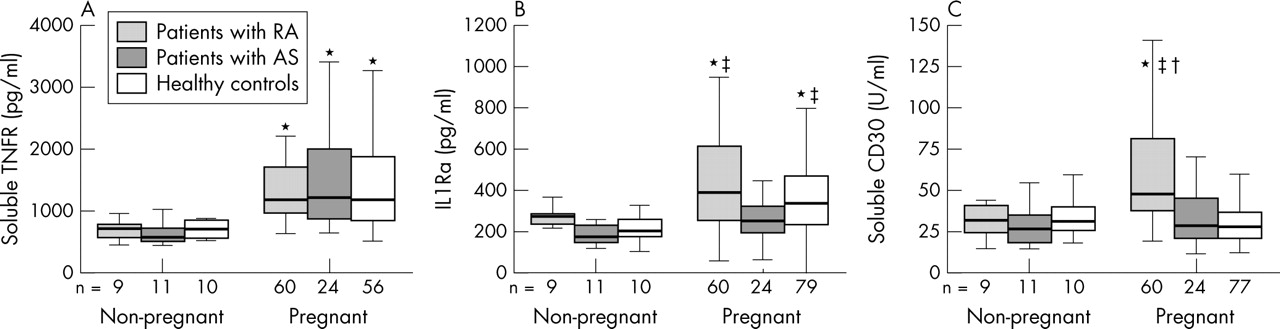
Significantly higher circulating levels of sTNFR (fig 1A; RA: p<0.001, AS p<0.001, healthy: p = 0.001) were measured in the cohorts of pregnant women compared with non-pregnant women matched for age. Levels of IL1Ra were significantly raised in pregnant healthy women and pregnant patients with RA compared with non-pregnant controls (fig 1B; healthy: p = 0.001, RA: p = 0.034), and they exceeded levels measured in pregnant patients with AS (RA: p = 0.002; healthy: p = 0.013). Only patients with RA showed significantly higher levels of sCD30 (fig 1C) in pregnant compared with non-pregnant subjects (p = 0.001), and compared with pregnancy levels of patients with AS (p<0.001) and healthy women (p<0.001). Among the groups of non-pregnant women, no significant differences were seen for sTNFR, IL1Ra, and sCD30.

Levels of (A) sTNFR, (B) IL1Ra, and (C) sCD30 in patients with RA, patients with AS, and healthy women. Values presented in the group of non-pregnant (no pre-pregnancy or postpartum data included) and pregnant (pooled data of first, second, and third trimester) subjects. Horizontal bar within the box marks the median, the boxes represent the range of ±25% around the median (interquartile range). Vertical bars indicate 95% confidence interval. *Significant difference compared with the non-pregnant control group (p<0.05 by Mann-Whitney U test); †significant difference compared with healthy pregnant women (p<0.05 by Mann-Whitney U test); ‡significant difference compared with pregnant patients with AS (p<0.05 by Mann-Whitney U test).
Changes of sTNFR-75, IL1Ra, and sCD30 during and after pregnancy
A gradual, albeit not significant, increase of sTNFR occurred both in healthy women and patients during pregnancy, followed by a significant decrease of sTNFR post partum (figs 2 A, B, C). A moderate negative correlation (rs = −0.448, p = 0.05) was observed between sTNFR and RADAI. None of the other clinical assessments correlated with levels of sTNFR.

Levels of sTNFR before, during (first, second, and third trimester), and after pregnancy (6, 12, and 24 weeks post partum) in patients with (A) RA or (B) AS, and (C) in healthy controls. Horizontal bar within the box marks the median, the boxes represent a range of ±25% around the median (interquartile range). Vertical bars indicate 95% confidence interval. Significant changes indicated by p values (Wilcoxon test for paired data).
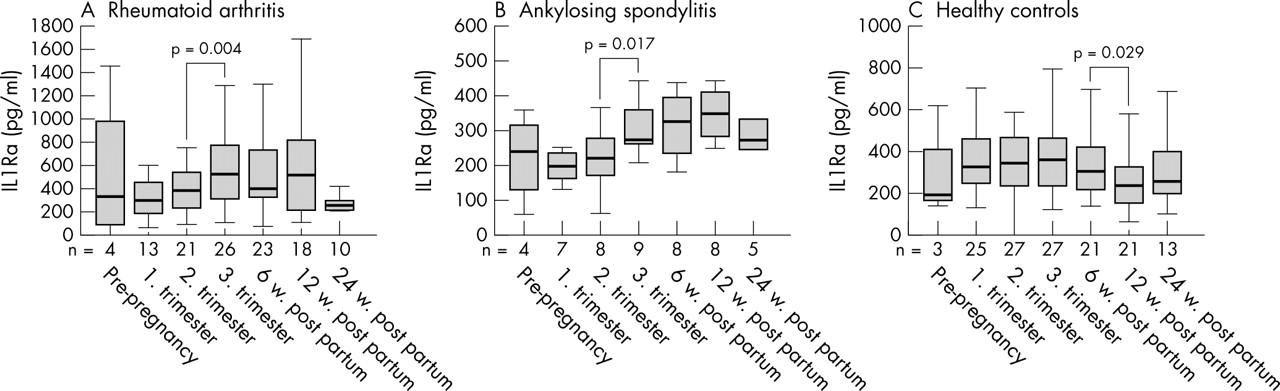
In patients with RA and AS, a significant rise of IL1Ra appeared from the second to the third trimester of pregnancy (figs 3A and B). In parallel, disease activity as measured by the PGA was at its lowest in the second and third trimester. In healthy women no significant increase of IL1Ra was found during pregnancy, but a significant decrease of IL1Ra occurred from 6 to 12 weeks post partum (fig 3C). Levels of IL1Ra in patients with RA and AS correlated weakly to moderately with disease activity measured by the PGA (rs = −0.269, p = 0.01), the tender joint count (rs = −0.349, p = 0.01), and the swollen joint count (rs = −0.263, p = 0.01), but not with the RADAI or BASDAI.
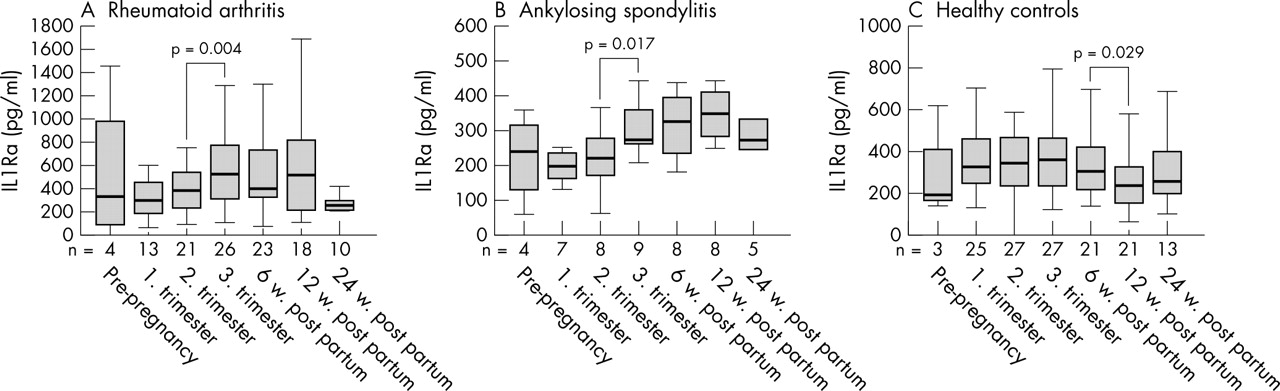
Levels of IL1Ra before, during (first, second, and third trimester), and after pregnancy (6, 12, and 24 weeks post partum) in patients with (A) RA or (B) AS, and (C) in healthy controls. Horizontal bar within the box marks the median, the boxes represent a range of ±25% around the median (interquartile range). Vertical bars indicate 95% confidence interval. Significant changes indicated by p values (Wilcoxon test for paired data).
sCD30 decreased gradually during pregnancy and showed an increase at 6 weeks post partum in the three groups of pregnant women (figs 4A, B, and C). In patients with RA and AS, levels of sCD30 did not correlate with any of the clinical assessment instruments.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Levels of sCD30 before, during (first, second, and third trimester), and after pregnancy (6, 12, and 24 weeks post partum) in patients with (A) RA or (B) AS, and (C) in healthy controls. Horizontal bar within the box marks the median, the boxes represent a range of ±25% around the median (interquartile range). Vertical bars indicate 95% confidence interval. Significant changes indicated by p values (Wilcoxon test for paired data).
DISCUSSION
Our longitudinal study comparing pregnant patients with rheumatic disease and healthy pregnant women found similar cytokine profiles in both groups, with few quantitative differences. This can be expected in patients who enter pregnancy in a state of low disease activity and with little or no organ involvement as did our patients. Thus the physiological alterations induced by pregnancy are not profoundly affected by a chronic inflammatory state, but provide a cytokine milieu that supports pregnancy. In agreement with other studies comparing healthy pregnant women with non-pregnant controls,21,22 we found raised levels of IL1Ra and sTNFR in pregnant patients and controls, whereas IL1β, IFNγ, and IL10 were undetectable. Results are conflicting for the circulating levels of IFNγ and IL1β, which have been found either absent or in low levels during pregnancy.23–25 The inability to detect circulating IL10 in pregnancy corresponds with another longitudinal study investigating IL10 in plasma of healthy pregnant women at each trimester.22 By contrast, low levels of IL10 were found in a cross sectional study of women in their second and third trimester.26
Inflammatory rheumatic diseases are associated with a proinflammatory cytokine profile systemically and locally not only at times of active symptoms but also during quiescent disease.8,9,27,28 Up regulation of the inflammatory cytokine IL1β has been reported in RA and AS, sometimes accompanied by an IL1Ra deficiency.29–31 Treatment with the recombinant TNFR:Fc fusion protein and with recombinant IL1Ra is efficacious in RA and AS.32–35 Thus, increased levels of IL1Ra in the third trimester might overcome a deficiency in pregnant patients with RA and AS and lead to improvement of the disease. The negative correlation between IL1Ra and disease activity supports this notion. Likewise, raised sTNFR levels in pregnant patients with RA and AS might contribute to an improvement of the disease in late pregnancy.
It has been suggested that the remission so often seen in RA during pregnancy may relate to the increased gestational secretion of IL10, resulting in the induction of tolerance.36 In our study IL10 was either below detection levels or present in few patients with active RA post partum. Even in the absence of raised circulating levels of IL10, T cells of peripheral blood could still increase their IL10 secretion as shown recently in four pregnant patients with RA.37 However, the role of IL10 in joint inflammation is ambiguous. Experiments on joint tissues have shown that inflammation is suppressed by IL10.38 Furthermore, Th2 committed T cells and regulatory T cells, which counteract inflammation and autoimmunity, produce high levels of IL10.14,39 On the other hand, a study of IL10 polymorphism in RA found an association between high production of IL10 and joint destruction.40 This may, in part, be due to the effect of IL10 on monocyte maturation, rendering them into tissue infiltrating cells,41 or to the stimulation of autoantibody production and enhancement of Fc gamma receptor expression on monocytes.42 Also in patients with active spondyloarthropathy raised levels of circulating IL10 have been found.29
sCD30 is an indirect marker for a Th2 immune response and can be induced by progesterone together with IL4 production.43 A rise of sCD30 during pregnancy would therefore be expected. Interestingly, this was observed exclusively in our pregnant patients with RA, who had markedly higher gestational levels of sCD30 than the other groups of pregnant women and than non-pregnant patient cohorts. Owing to the few pre-pregnancy samples available, no statement can be made about whether sCD30 levels increased during the first trimester in patients with RA and then decreased again. A counterregulatory role for CD30+ T cells, providing an attempt to control inflammation in a Th1 driven disease like RA, has been discussed,44 and higher circulating levels of sCD30 have been found in non-pregnant patients with RA than in healthy controls.45 The latter finding was not confirmed by our results. In our longitudinal study, concentrations of sCD30 in patients and healthy controls decreased progressively during pregnancy, possibly as a result of the increasing plasma volume. The same dynamics were previously shown by others investigating sCD30 in healthy pregnant women.46 However, when the ratio of sCD26, a Th1 related molecule, and sCD30 was analysed, a predominance of the Th2 marker was demonstrated throughout pregnancy. Circulating sCD30 levels in our cohort of pregnant patients with RA did not correlate with disease activity measurements. This is at variance with another study showing an inverse correlation between sCD30 and CRP.47 Lack of correlation in our study was probably due to the low range of disease activity, with mostly normal CRP levels among our patients with RA.
Our study has several limitations—for example, the limited number of patients included and the small number of women with pre-pregnancy measurements. The gestational rise of a marker is sometimes only reflected by a significant drop after delivery and the significant difference of circulating levels in pregnant and non-pregnant subjects. Taking into account the dilution effect of the increasing plasma volume during pregnancy, emphasises that indeed an increase of the measured protein has taken place. A cytokine increase might also be hidden in the large interindividual variation that arises from different levels of disease activity at study entry, from treatment, and from genetic variation. However, the limited number of patients does not allow a separate analysis for subgroups.
To summarise, among the cytokines and regulatory molecules for which tests were carried out, an increase of the anti-inflammatory cytokines IL1Ra and sTNFR was found during pregnancy. IFNγ and IL10, markers of a Th1 and Th2 response, respectively, were either low or undetectable. The possibility cannot be excluded that at a local level a more pronounced change in the Th1/Th2 balance during and after pregnancy might have been measured. In addition, up regulation of IL1Ra and sTNFR as well as sCD30 in patients with RA during pregnancy may be indirect signs of a Th2 immune response because Th2 cytokines have been shown to induce the production of both sTNFR and IL1Ra.48,49 On the other hand, evidence accumulates that pregnancy promotes not only a Th2 response, but rather an immunomodulation that is complex and dependent on the stage of pregnancy.50 Because most of the disease activity markers did not correlate with the changes of circulating cytokines, the extent to which they contribute to pregnancy related improvement of disease activity in the third trimester remains open.
Acknowledgments
The study was supported by grant 31-59979 from the Swiss National Research Fund, and by grants from the Kurt and Senta Hermann-Stiftung and from the Swiss League against Rheumatism.