Article Text

Abstract
Objective: To investigate antibodies to complement 1q (anti-C1q) and investigate the correlation between anti-C1q titres and renal disease in systemic lupus erythematosus (SLE).
Methods: 151 SLE patients were studied. In patients with biopsy proven lupus nephritis (n = 77), activity of renal disease was categorised according to the BILAG renal score. Sera were tested for anti-C1q by enzyme immunoassay. Serum samples were randomly selected from 83 SLE patients who had no history of renal disease, and the positive and negative predictive value of the antibodies was studied.
Results: Patients with active lupus nephritis (BILAG A or B) had a higher prevalence of anti-C1q than those with no renal disease (74% v 32%; relative risk (RR) = 2.3 (95% confidence interval, 1.6 to 3.3)) (p<0.0001). There was no significant difference in anti-C1q prevalence between SLE without nephritis and SLE with non-active nephritis (BILAG C or D) (32% v 53%, p = 0.06) or between active and non-active nephritis (74% v 53%, p = 0.06). Patients with nephritis had higher anti-C1q levels than those without nephritis (36.0 U/ml (range 4.9 to 401.0) v 7.3 U/ml (4.9 to 401.0)) (p<0.001). Anti-C1q were found in 33 of 83 patients (39%) without history of renal disease. Nine of the 33 patients with anti-C1q developed lupus nephritis. The median renal disease-free interval was nine months. One patient with positive anti-C1q was diagnosed as having hypocomplementaemic urticarial vasculitis syndrome during follow up.
Conclusions: Anti-C1q in SLE are associated with renal involvement. Monitoring anti-C1q and their titres in SLE patients could be important for predicting renal flares.
- anti-dsDNA, antibodies against double stranded DNA
- APS, antiphospholipid syndrome
- BILAG, British Isles Lupus Assessment Group
- SLE, systemic lupus erythematosus
- BILAG score
- autoantibodies
- systemic lupus erythematosus
- nephritis
Statistics from Altmetric.com
- anti-dsDNA, antibodies against double stranded DNA
- APS, antiphospholipid syndrome
- BILAG, British Isles Lupus Assessment Group
- SLE, systemic lupus erythematosus
Glomerulonephritis is a major determinant of the course and prognosis of systemic lupus erythematosus (SLE) and is clinically evident in 40–85% of patients. Several autoantibodies, especially those against double stranded DNA (anti-dsDNA), are believed to play a major role in the induction of glomerular inflammation.1–3 Raised titres of anti-dsDNA and hypocomplementaemia are reported to be associated with the activity of the disease.4–6 However, the lack of specificity of these biological markers for renal exacerbations has led to the search for other autoantibodies that might contribute to nephritis and help diagnose a renal flare. Recently, it has been suggested that antinucleosome antibodies are a more sensitive marker of SLE than anti-dsDNA,7,8 particularly the IgG3 isotype which might constitute a selective biological marker of active SLE and lupus nephritis.9
C1q is the first component of the classical pathway of complement activation and its main function is to clear immune complexes from tissues and self antigens generated during apoptosis.10,11 Hereditary deficiency of this component is a known risk factor for the development of SLE.12 In 1984, antibodies directed to C1q (anti-C1q) were reported in the serum of patients with SLE, with a prevalence ranging from 34% to 47%,13–19 and in patients with hypocomplementaemic urticarial vasculitis syndrome (HUVS) with a prevalence of 100%.17
Recently, it has been suggested that the presence of anti-C1q is a required condition for the development of lupus nephritis.20,21 Some investigators have also proposed that monitoring anti-C1q might be valuable for the clinical management of SLE patients as a non-invasive biological marker of renal disease.22 However, to date, testing for these antibodies still does not have a definite place in daily clinical practice.
We designed this study to investigate further the clinical value of anti-C1q in a large cohort of SLE patients.
METHODS
Patients
The first part of this study comprised 151 patients with SLE, all fulfilling the 1982 criteria for the classification of the disease23 (141 female, 10 male; median age 39 years (range 15 to 74); median disease duration 8 years (0.1 to 52)). Seventy seven patients had biopsy proven lupus nephritis and 74 had no evidence of renal disease at the time of the study.
For the second part of the study, we included 83 consecutive patients fulfilling at least four of the 1982 criteria for the classification of SLE23 (78 female, 5 male; median age 44 years (18 to 74); median disease duration 9 years (1 to 52), median follow up 24 months (1 to 60)) with no previous history of renal involvement at the time of serum collection. All medical records were carefully reviewed retrospectively.
Procedures
Evaluation of renal involvement
The World Health Organisation (WHO) classification of lupus nephritis24 was used to define the histological lesions, and mixed forms were classified in keeping with the identified proliferative lesion. The individual components of the renal pathology were classified and scored according to previously published activity and chronicity scores.25
Data on renal disease activity corresponding to the patients’ samples were abstracted from medical records and categorised according to the British Isles Lupus Assessment Group (BILAG) renal score.26 The BILAG index assesses eight organs or systems separately, and each system is allocated an alphabetic score (A–E) defined by the presence or absence of specific clinical features (table 1).
BILAG renal score
In the majority of patients with nephritis, serum samples were taken before starting immunosuppressive treatment. However, as some patients were treated locally, their blood was tested in the first four months after the beginning of the immunosuppressive treatment.
Anti-C1q determination
Anti-C1q were tested in serum using a commercially available enzyme immunoassay (EIA) kit (Diagenics, Milton Keynes, UK), under 1 M NaCl conditions as described previously.27 Briefly, standards, controls, and patient sera were incubated with human C1q adsorbed into the microtitre plate. After washing, an IgG horseradish peroxidase labelled conjugate was added in the appropriate dilution. Colour was developed by adding an enzyme substrate (tetramethylbenzidine in citrate buffer with hydrogen peroxidase). The reaction was stopped by adding 0.25 M sulphuric acid and optical densities at 450 nm were measured by a Titertek Multiskan MC apparatus (Flow Laboratories, Herts, UK). Optical densities were then converted to units (U) by being plotted against the autoantibody titre of the standards given by the manufacturer.
Other laboratory measurements
Levels of serum complement C3 and C4 were measured by nephelometry, and anti-dsDNA by radioimmunoassay.
Statistical analysis
All statistical analysis was carried out using the SPSS 11.0 program (Microsoft software). Comparisons between patients groups were expressed as relative risk with 95% confidence interval (RR (95% CI)), where only a lower limit >1 was considered significant. Differences between means were analysed by the Spearman correlation coefficient. Comparisons between subject groups were made using Mann–Whitney test. A probability (p) value of <0.05 was considered significant.
RESULTS
Demographic data and clinical characteristics
The nephritis group (n = 77) comprised six male and 71 female patients, with a median age of 35 years (range 15 to 65) and a median disease duration of eight years (0.1 to 36).
Fifty five patients had proliferative nephritis (26 in class III and 29 in class IV), 10 had membranous nephritis (class V), 11 had mesangial nephritis (class II), and one had glomerulosclerosis according to the WHO classification. At the time of the sera collection, 43 patients were categorised as having active nephritis (39 in BILAG category A and four in category B). Thirty four patients had quiescent renal disease (26 in BILAG category C and eight in category D). Twenty one of these patients fulfilled criteria for the antiphospholipid syndrome (APS).28
The non-nephritis group (n = 74) comprised four male and 70 female patients, with a median age of 44 years (18 to 74) and a median disease duration of nine years (1 to 52). Fifteen of these patients fulfilled criteria for the APS.28
There were no differences in male/female distribution or disease duration between groups. However, patients with nephritis were younger than the non-nephritis group (p = 0.0001).
Prevalence and clinical associations of anti-C1q
Anti-C1q were found in 74 of the 151 SLE patients (49%). Patients with nephritis more often had anti-C1q than those without a history of renal disease (65% v 32%, RR = 2.0 (95% CI, 1.4 to 2.9); p<0.001). Patients with active lupus nephritis (BILAG A or B) had a higher prevalence of anti-C1q than those without renal disease (74% v 32%, RR = 2.3 (1.6 to 3.3); p<0.0001). However, there was no significant difference between patients without nephritis and those with non-active nephritis (BILAG C or D) (32% v 53%; p = 0.06) or between patients with active and non-active nephritis (74% v 53%; p = 0.06).
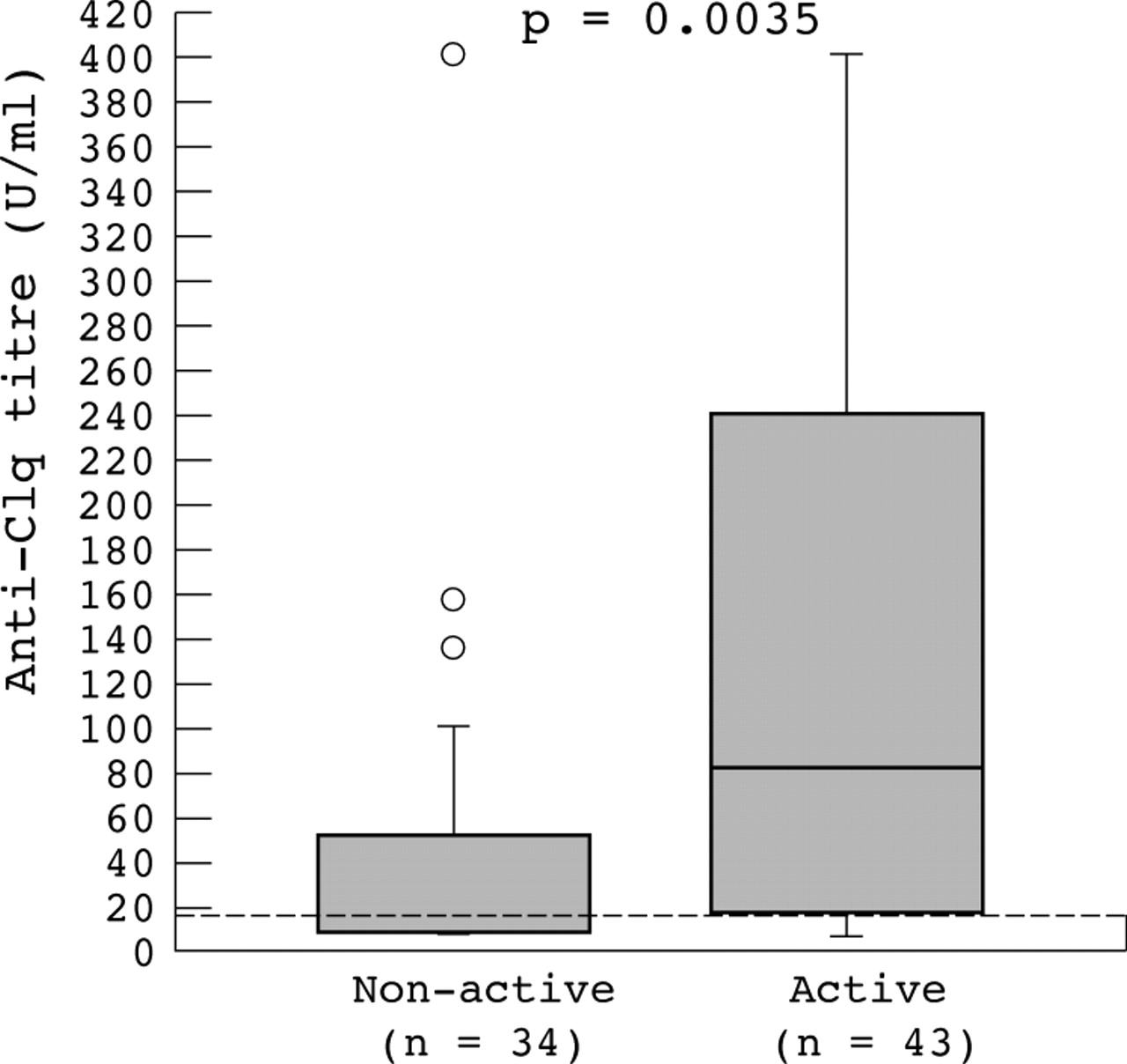
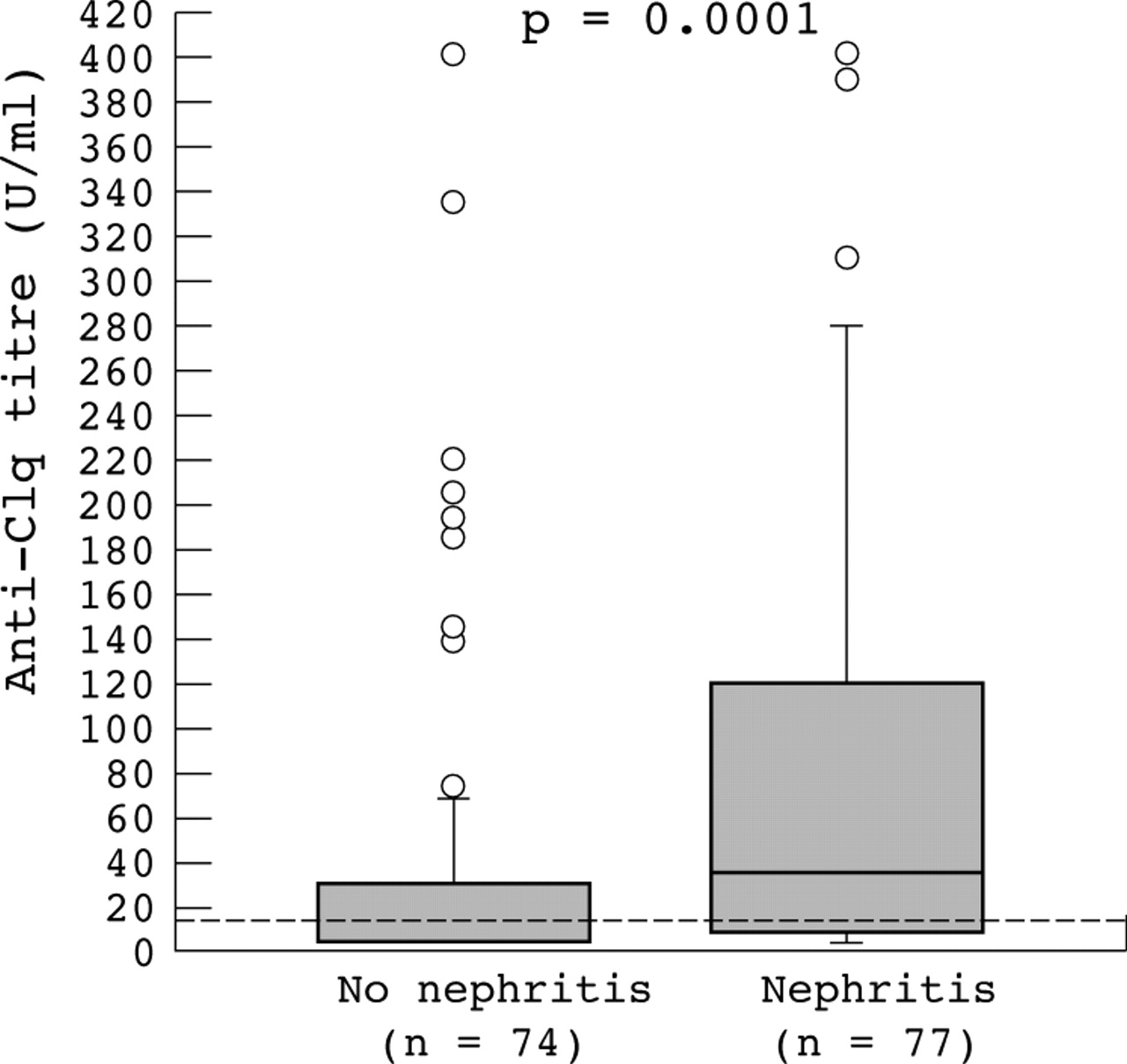
Higher titres of anti-C1q were found in patients with renal involvement than in those with no renal involvement (36.0 U/ml (4.9 to 401.0) v 7.3 U/ml (4.9 to 401.0)) (p<0.001) (fig 1). In particular, those with active nephritis had significantly higher anti-C1q titres than those with quiescent renal involvement (80.0 U/ml (4.9 to 401.0) v 17.5 U/ml (4.9 to 401.0)) (p = 0.0035) (fig 2).

Anti-C1q antibody titres in 151 patients with systemic lupus erythematosus. Dashed lines indicate cut off for positivity. This graph shows the median, first to third quartiles (box), interquartile range (whiskers), and outliers (circles). Higher titres of anti-C1q were found in patients with v without renal involvement; the difference was significant.
{kind=link}
{kind=link}
Anti-C1q titres and activity of renal disease in 77 patients with systemic lupus erythematosus and renal involvement. This graph shows the median, first and third quartiles (box), interquartile range (whiskers), and outliers (circles). Higher titres of anti-C1q were found in patients with v without renal involvement; the difference was significant.
There were no differences in anti-C1q prevalence or titres between patients with proliferative and non-proliferative glomerulopathy (69% v 57%, or 34.5 U/ml (4.9 to 401.0) v 40.9 U/ml (4.9 to 401.0), respectively.
Anti-C1q and other serological markers of disease activity
When comparing anti-C1q titres with known serological markers of disease activity, we found a negative correlation with levels of C3 and C4 and a positive correlation with anti-dsDNA. No significant correlation was found with serum creatinine, glomerular filtration rate, proteinuria, or histological activity index (table 2).
Correlation of anti-C1q with laboratory indices of renal disease
Anti-C1q in patients with no renal disease
As some patients without nephritis had positive anti-C1q, we studied a cohort of 83 SLE patients with no previous history of renal involvement at the time of serum collection.
Anti-C1q were detected in 33 of the 83 patients (39.8%). Nine of these 33 patients (27.3%) developed lupus nephritis. All nine patients underwent renal biopsy which showed a proliferative form of glomerulopathy (WHO classes III or IV). The renal disease-free interval from the time of serum collection ranged from two to 48 months (median nine months). One patient with positive anti-C1q was later diagnosed as having hypocomplementaemic urticarial vasculitis syndrome (HUVS).
The remaining 23 patients with positive anti-C1q are being closely followed up for the development of kidney disease.
None of the 50 patients with negative anti-C1q developed any sign of renal involvement.
DISCUSSION
Our studies were designed to clarify the role of anti-C1q testing in the diagnosis and monitoring of SLE. In a cross sectional study of a cohort of 151 SLE outpatients, 77 with and 74 without lupus nephritis, we showed a strong association between high titres of anti-C1q and renal disease, especially active glomerulonephritis. In addition, in a retrospective analysis of 83 SLE patients, anti-C1q were found to have very high sensitivity and negative predictive value for the occurrence of renal disease.
Anti-C1q were detected in 65% of patients with nephritis, compared with 32% of those with no renal disease—a prevalence within the range reported in previous studies.15,18,19,29,30 Specifically, higher titres were associated with the presence of nephritis, as previously described.15,19,31 Our data confirm a strong association between anti-C1q and lupus nephritis in a large series of patients, including a significant number with nephritis.
Earlier investigations suggested that development or recurrence of nephritis was associated with rising titres of anti-C1q in the preceding six months19,31 and that these were more specific for active renal involvement than anti-dsDNA.32 This prompted us to explore the potential role of anti-C1q in the early diagnosis of renal relapses. Comparing patients with active and inactive nephritis, defined according to strict criteria, we showed that although there was no significant difference in the prevalence of anti-C1q, active nephritis was associated with higher titres.
Like others,15,19,29,31 we found a good correlation between anti-C1q and other recognised markers of disease activity in SLE. Curiously, although higher anti-dsDNA values were associated with activity of nephritis, there was no difference in prevalence of anti-dsDNA in patients with and without nephritis, supporting previous evidence of the superior specificity of anti-C1q over anti-dsDNA for renal flares.31,32 It is clear that these findings could have been influenced by the fact that some of the serum samples were taken in the first four months after beginning immunosuppressive treatment, as anti-dsDNA values fall very rapidly after treatment.33
In our retrospective study, 33 of 83 patients had anti-C1q at the time of serum sampling. Increased levels of anti-C1q were found in all the nine patients who developed renal disease during follow up. The positive predictive value of anti-C1q for nephritis was 9/33 (27.3%), which is lower than in other reports,19,20 probably because our follow up period was shorter. More significantly, none of the 50 patients negative for anti-C1q had or developed lupus nephritis, corresponding to a negative predictive value of 100%. Again, our results corroborate findings from smaller studies and strengthen the hypothesis that there is no lupus nephritis in the absence of anti-C1q.21
However, we must bear in mind that in our cross sectional study only 65% of patients with renal disease had anti-C1q, implying that 35% of patients with nephritis, and in particular 26% with active nephritis, tested negative for antibodies to C1q. We could not single out a different characteristic in these patients, even in the histological type of lesion on renal biopsy. However, three of these patients were tested for anti-C1q while on treatment for nephritis. In addition, patients with nephritis and negative anti-C1q titres tended to have more longstanding disease, particularly renal disease (data not shown), so we might speculate that they were heavily immunosuppressed in the past. This could be a reason for false negative testing, as earlier reports show a decline in anti-C1q following initiation of immunotherapy.30,34 Other possible explanations for the absence of anti-C1q in some patients with active lupus nephritis are raised by studies by Gunnarsson et al.18 In a longitudinal study of 21 SLE patients with active disease, they found that all patients with proliferative nephritis had high ongoing production of anti-C1q in peripheral cells, although not every one had positive serum levels of anti-C1q.18 The same investigators reported that only 11 of 18 patients with biopsy confirmed lupus nephritis had anti-C1q but C1q was low in most of these patients and correlated negatively with anti-C1q. A question is raised as to whether the antibodies bind to C1q, forming immune complexes, or are particularly readily sequestered in the kidney.35
One of the important physiological functions of the classical pathway of complement is the disposal of immune complexes and the products of inflammatory injury, and recent data suggest a role for C1q in the clearance of apoptotic cells.10,11 There is at present much interest in the hypothesis that a major source of the autoantigens driving the immune response in SLE is the apoptotic cell. Binding of autoantibodies to the collagen-like region of C1q could interfere with activation of C1 and functionally resemble a C1q deficient state. This may provide a unifying explanation for the paradoxical finding that homozygous C1q deficiency causes SLE while many patients with SLE have anti-C1q. In both situations the interference with the putative physiological role of C1q mediated clearance of apoptotic cells would result in autoimmunity.36
The strong correlation between anti-C1q and lupus nephritis appears to be a general finding in our own and many other studies. Anti-C1q show a significant inverse correlation with levels of C1q, C3, and C415,19,29,35,37 and decreases in these components of the complement classical pathway are associated with active renal disease.35,38,39 In addition, anti-C1q have been recovered at necropsy from the glomeruli of patients with proliferative lupus nephritis.40 A recent experimental report in rodents showed that infusion of anti-C1q resulted in reduced levels of circulating C1q and deposition of anti-C1q and complement components in the glomerulus.41 The available data suggest that autoantibodies against C1q have a definite role in the pathogenesis of lupus glomerular injury but so far we can only speculate how these antibodies exert their nephritogenic effect. Anti-C1q may either contribute to the formation of circulating immune complexes that are deposited in the kidneys or contribute to local formation of immune complexes on the glomerular basement membrane. By interfering with activation of the complement system through the classical pathway, anti-C1q may hamper immune complex solubilisation, further contributing to immune complex deposition in the kidney.
Prevailing knowledge associates anti-C1q specifically with proliferative forms of lupus nephritis.14,15,18,19,31 However, we did not find differences in the prevalence or levels of anti-C1q when comparing proliferative and non-proliferative forms of nephritis. We suggest that previous results, drawn from a small number of patients—particularly those with non-proliferative nephritis—do not hold true in a large patient cohort. This implies that, contrary to the accepted wisdom, anti-C1q have a potential pathogenic effect in all types of lupus nephritis, including mesangial and membranous nephritis.
Conclusions
In a representative sample of the population in a lupus clinic, we have shown that anti-C1q are useful to identify a subgroup of SLE patients at risk for renal disease, and that monitoring anti-C1q titres is potentially more helpful in the early diagnosis of nephritis or the prediction of renal flares than the currently employed indices of disease activity.