Article Text

Abstract
OBJECTIVE To investigate the incidence of retinopathy in systemic lupus erythematosus (SLE) and to clarify its significance in relation to other clinical manifestations.
METHODS A cross sectional study on lupus retinopathy was made in 69 patients with SLE. One expert ophthalmologist examined the ocular fundi of the lupus patients without any information of their disease state. Clinical and laboratory findings in the patients with retinopathy and those without were compared.
RESULTS Retinopathy was found in 7/69 (10%) patients. The findings included haemorrhages, vasculitis, cotton wool spots, and hard exudates, all of which were considered to reflect vascular damage. Retinopathy was found to be associated with the presence of anticardiolipin antibody (p<0.05) and with central nervous system lupus (p<0.01). The patients with retinopathy had higher levels of serum creatinine than the patients without retinopathy (p<0.01). The disease activity of lupus, as assessed by the maximum SLE disease activity index (SLEDAI) score of the patients, was also significantly higher in the patients with retinopathy (p<0.03).
CONCLUSION Incidence of retinopathy in SLE was similar to that in previous reports and it may reflect tissue microangiopathy, particularly associated with vasculitis or anticardiolipin antibodies, or both.
- systemic lupus erythematosus
- retinopathy
- antiphospholipid antibody
- ocular disease
Statistics from Altmetric.com
It is known that patients with systemic lupus erythematosus (SLE) sometimes have ocular manifestations. It is generally understood that the causes of ocular manifestations of SLE include active lupus, antiphospholipid antibody syndrome (APS), and drugs used to treat SLE.1 The most common pattern of retinopathy is thought to be microangiopathy.2 However, it is not well understood whether retinopathy correlates with antiphospholipid antibodies (aPL) or central nervous system (CNS) disease.
aPL represent a heterogeneous group of antibodies against phospholipid binding proteins or their complexes with anionic phospholipids.3 As the presence of aPL often provokes arterial and venous thrombosis, intrauterine fetal loss, and thrombocytopenia,4 many organs may be affected by these antibodies.5 ,6 On the other hand, CNS disease is known as a severe manifestation of SLE. CNS lupus is thought to be mainly associated with vasculopathy7 and it is characterised by a wide variety of clinical features, from mild psychotic symptoms to severe convulsion or disturbance of consciousness. An association of aPL with CNS lupus has also been described.8 ,9 This prompted us to make a cross sectional study of lupus retinopathy with special reference to aPL and CNS disease in patients with SLE.
Patients and methods
PATIENTS
Sixty nine consecutive patients with SLE (four male, 65 female) who fulfilled the American College of Rheumatology criteria for SLE10 were enrolled; three were inpatients and 66 outpatients. The mean ages at the onset of SLE and at the ophthalmological examinations were 32.1 and 40.7 years, respectively. Fifty three patients were receiving corticosteroids and 16 patients had never received them; no patients had discontinued corticosteroid treatment. The mean duration of steroid treatment was 5.8 years. The average daily dose of steroids at the ophthalmological examination was 7.8 mg (as prednisolone). Seven patients had taken immunosuppressant drugs, including cyclophosphamide and azathioprine.
METHODS
One expert ophthalmologist (KU) carried out all the ophthalmological examinations without knowledge of the general condition of each patient or of laboratory findings. Retinopathy was defined as the presence of any of the following lesions: haemorrhages, vasculitis (sheathing of retinal arterioles and/or venules or vascular tortuosity), cotton wool spots, papilloedema, optic atrophy, or retinal detachment according to the report of Stafford-Bradyet al.2 In addition to these findings, we also included hard exudates unless the patients had essential hypertension or diabetes mellitus, because they were considered to be the result of deposition of exudated lipids or proteins from the degenerated ocular nerves or from vessels with hyperpermeability. Retinal lesions considered to be caused by hypertension (that is, not caused by SLE), arteriosclerosis, or diabetes mellitus, were excluded. We divided the patients into two groups according to the presence or absence of retinopathy, and clinical and laboratory findings were compared between the groups. The maximum disease activity through the entire history of SLE in each patient was scored according to SLE disease activity index (SLEDAI).11 Renal disease was defined according to 1982 ACR criteria10: persistent proteinuria (>0.5 g/day or >3+) or cellular casts, or both. In addition, a raised serum creatinine level (normal >84 μmol/l) was also included in the index. Measurement of anticardiolipin antibodies was performed with a commercially available anticardiolipin enzyme linked immunosorbent assay (ELISA) kit (Yamasa Shoyu Co, Ltd, Chiba, Japan). If the titre was over 3.2 U/ml, the result was defined as positive.
STATISTICS
The data were analysed with Student'st test, χ2 test, and Fisher's 2×2 test.
Results
INCIDENCE AND FEATURE OF RETINOPATHY
Retinopathy was found in 7/69 (10%) patients—all female. The mean age at onset of SLE in the patients with and without retinopathy was 34.2. and 31.9 years, respectively. The mean age at the ophthalmological examination of each group was 42.3 and 40.4 years, respectively. The dose of steroids and the incidence of immunosuppressant treatment in both groups were similar (table1).
Backgrounds of the patients with systemic lupus erythematosus (SLE)
Table 2 summarises the retinal findings of the patients with lupus retinopathy. Five of the seven patients had microhaemorrhages; this was the most common finding. Vasculitic lesions, cotton wool spots, and hard exudates were each found in two patients. As none of the patients had essential hypertension or diabetes mellitus, these findings were attributed to lupus retinopathy.
Retinal findings in patients with lupus retinopathy
CLINICAL FEATURES OF THE PATIENTS WITH LUPUS RETINOPATHY
Table 3 shows clinical features of the seven patients with retinopathy. Patient 1 was a new case of SLE. She had severe chorea and mild proteinuria. Other patients were all outpatients and their disease was inactive when examined. CNS disease was found in 5/7 (71%) patients, being significantly higher than in those without retinopathy (8/62 (13%), p<0.01). As shown, the CNS manifestations varied, including chorea, convulsion, manic state, epilepsy, and visual hallucination. Four of seven patients with retinopathy had proteinuria or a raised serum creatinine level, or both. Figure 1 shows that the serum creatinine concentration was higher in the patients with retinopathy than in those without (84.0 μmol/lv 56.6 μmol/l, p<0.01). Moreover, proteinuria was more commonly found in the patients with retinopathy than in those without (4/7 (57%) v 8/62 (13%), p<0.02) (data not shown). These results indicate that retinopathy may have a tendency to develop in patients with CNS or renal disease, or both.
Clinical features of the patients with lupus retinopathy
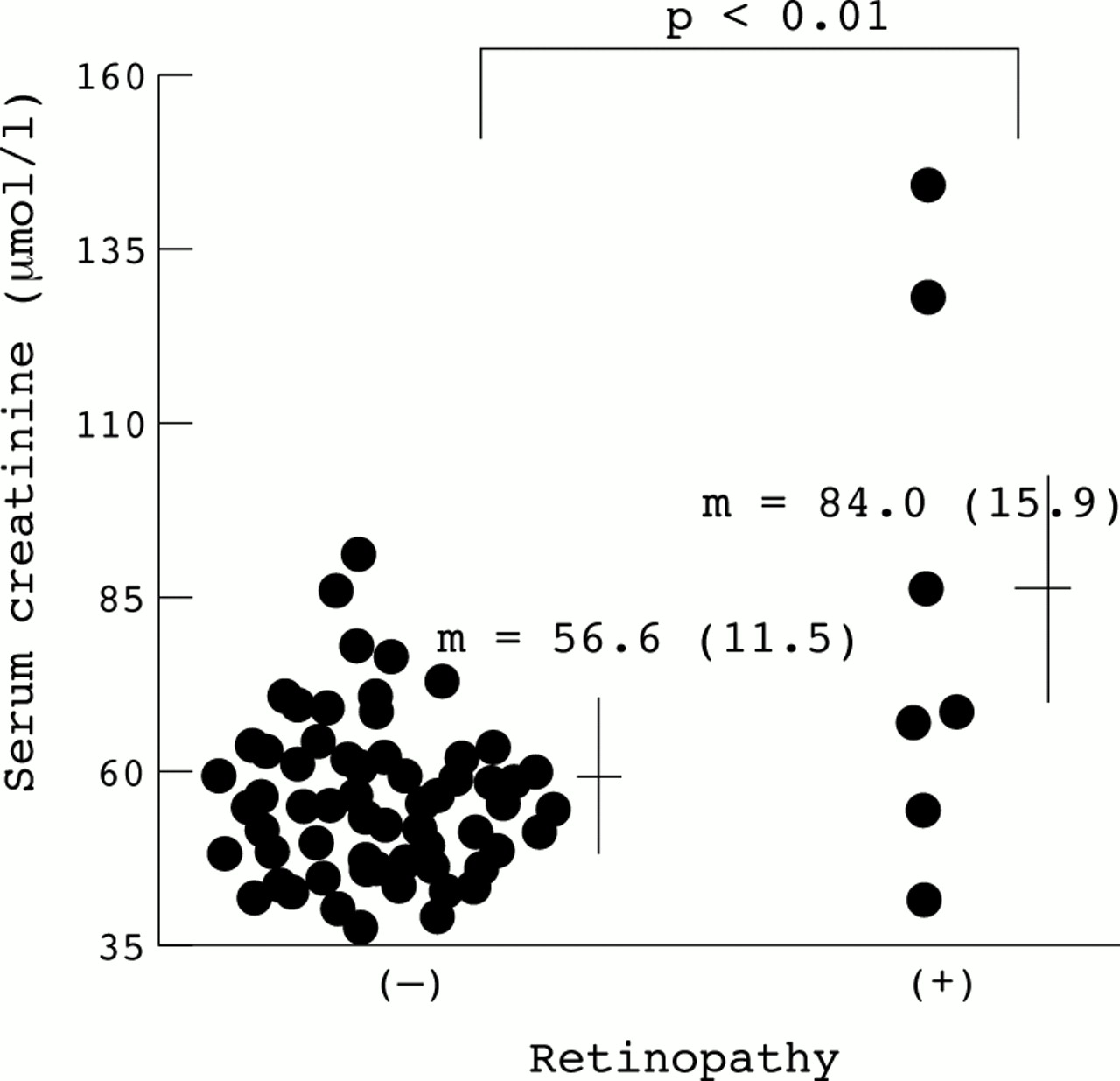
Serum creatinine concentrations in the patients with or without retinopathy.
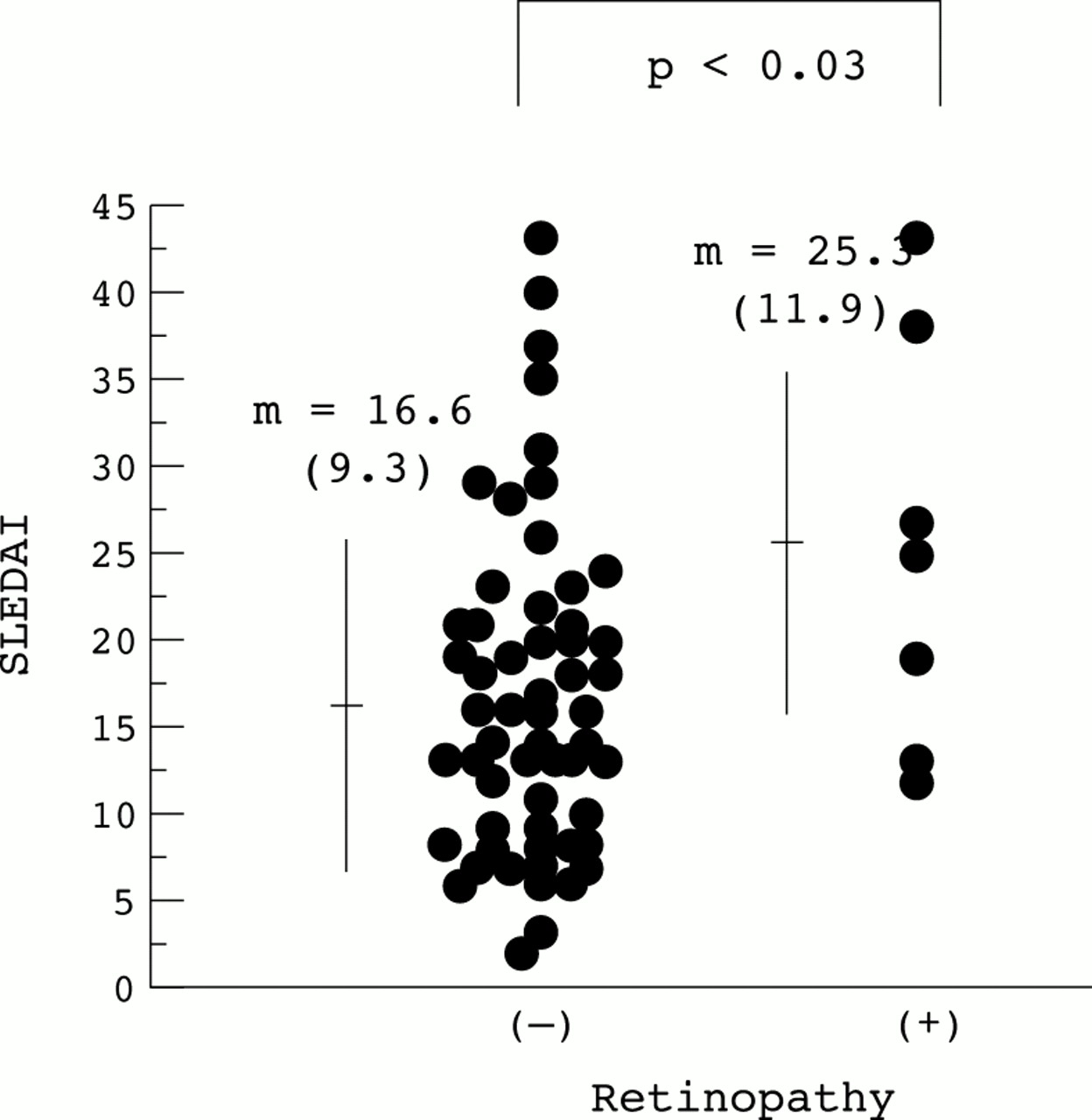
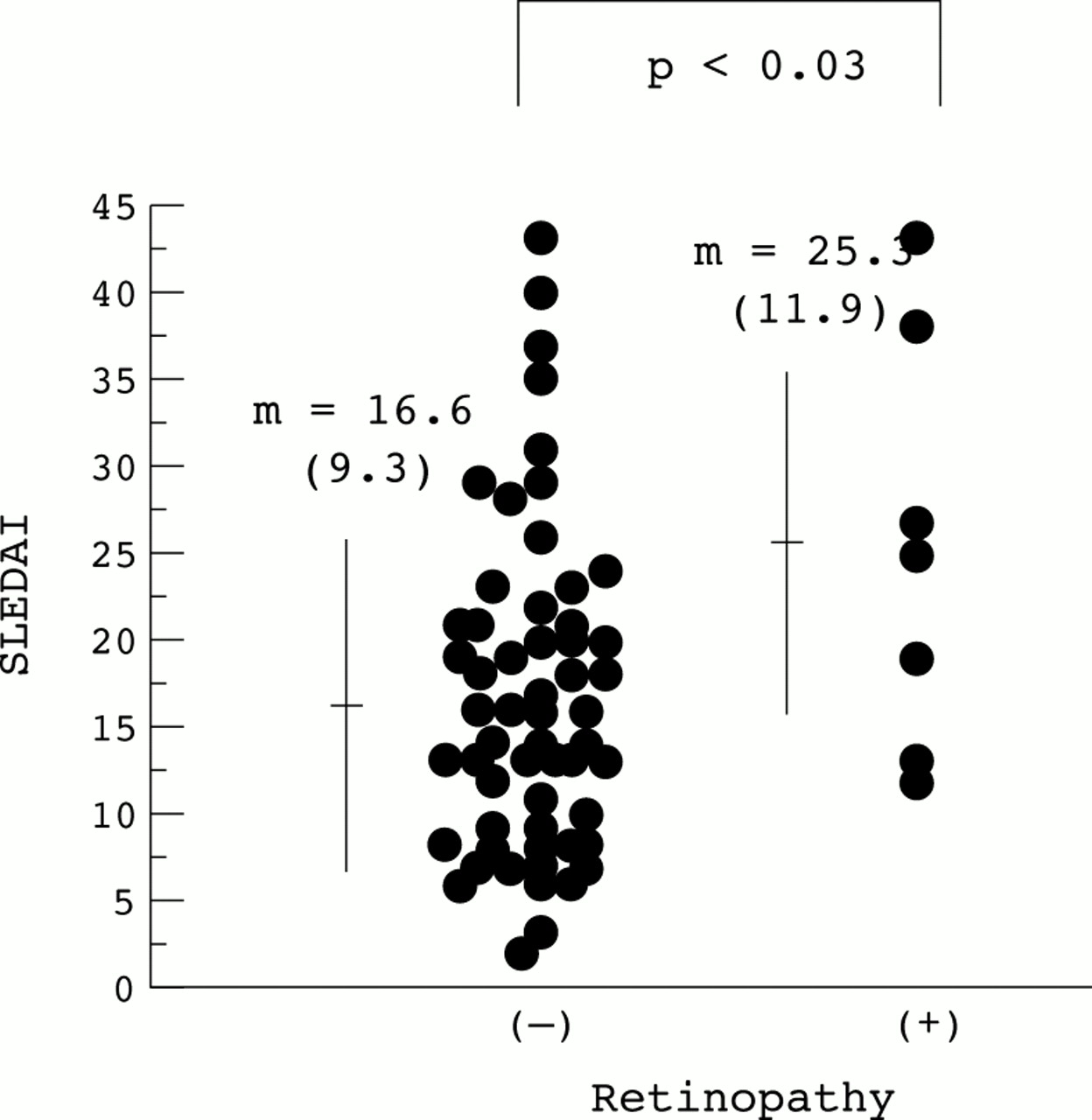
In an attempt to investigate whether the development of lupus retinopathy was associated with the disease activity of SLE, the maximum score of the SLE disease activity index (SLEDAI) in each patient was measured. Figure 2 shows that the patients with retinopathy had a higher score than those without it (25.3 (SD 11.9)v 16.6 (9.3), p<0.03), suggesting that development of retinopathy may be associated with the disease activity of SLE.
{kind=link}
{kind=link}
Systemic lupus erythematosus disease activity index (SLEDAI) scores in the patients with or without retinopathy. The maximum SLEDAI score for each patient is shown.
ASSOCIATION WITH ANTICARDIOLIPIN ANTIBODIES
IgG anticardiolipin antibodies (IgG aCL) were detected in 26 of 61 patients tested (43%). A significant difference in the prevalence of aCL between the two groups was found (table 4). Although IgG aCL were found in only 20/54 (37%) patients without retinopathy, 6/7 (86%) with retinopathy had IgG aCL (p<0.05). Two of the seven patients had evidence of aCL related events (infarctions and recurrent abortions) (table 3).
Correlation between retinopathy and anticardiolipin antibody (aCL)
Discussion
Retinopathy is one of the important, if not major, manifestation of SLE, which develops with an incidence of 72–26%.12 In our study retinopathy was found in 10% of the patients with SLE, comparable with previous studies. All the findings of retinopathy were considered to reflect vascular damage, such as vasculitis and thromboembolism. For instance, haemorrhages, which were seen in five patients, might have been caused by vasculitis, thromboembolism, or hypertension. In this study we included hard exudates in lupus retinopathy unless the patient had uncontrolled essential hypertension or diabetes mellitus. The hard exudates consist of proteinaceous and lipid material derived from exudation of serum components from vessels, or from an accumulation of lipid products from degenerating neural elements within the retina.13 Pathological examination of cotton wool spots discloses disciform thickening of the retinal nerve fibre layer.14 Vasculitis or microembolism of the retinal arterioles which supply blood to the retinal neurones may cause destruction of the vessel walls or neural fibres, or both, resulting in the formation of cotton wool spots and hard exudates.
An important finding characteristic of lupus retinopathy is thought to be vasculitis of the retinal capillaries associated with local microinfarction.1 Charles describes the diagnosis of retinal vasculitis with perivascular exudates and patches of fluorescein leakage along vessels.15 Histological evidence of immune mediated vasculitis has also been reported in lupus retinopathy.16 ,17 On the other hand, ocular fundus is the only part of the human body where we can directly observe small vessels without injuring the tissue. This suggests that lupus retinopathy reflects systemic vascular damage and that ocular fundus examination should be carried out more often. In fact, as shown in table 3, the six patients with lupus retinopathy had systemic organ findings associated with vascular disease. We found that the retinopathy in patients with SLE was associated with renal dysfunction, CNS lupus, and aCL, all of which were more or less related to vascular disorders. Although it is unclear whether lupus retinopathy is directly associated with renal disease, retinopathy may develop in severe SLE which involves the kidney or CNS, or both. This is supported by the fact that the patients with SLE with retinopathy had a higher SLEDAI score than those without it.
aPL are known to be associated with arterial and venous thrombosis.18 ,19 Our results showed that 43% of the patients with SLE had IgG aCL, comparable with the incidence found in previous studies.20 More importantly, an association of the presence of aCL with lupus retinopathy was found. It is considered that some of the findings of lupus retinopathy in this study, such as haemorrhage and cotton wool spots, might be caused by aPL. This indicates that aPL should be added to the list of candidates causing lupus retinopathy.
Previous studies have described the involvement of aPL in the pathogenesis of CNS lupus.19 Lie et al reported a patient with SLE and APS, examined post mortem, in whom systemic vasculitis and occlusive intimal proliferation of arterioles in the CNS were prominently seen.21 It is considered, therefore, that occlusive lesions or vasculitis, or both, might cause similar damage in the CNS and retinal tissue. In this study we have also shown that five of seven patients with lupus retinopathy had histories of CNS lupus with IgG aCL.
In conclusion, lupus retinopathy may reflect systemic, particularly CNS, vascular damage, which may develop in association with vasculitis or aCL, or both. In addition, the presence of retinopathy is suggestive of high disease activity during the history of SLE.
Acknowledgments
We thank Motoko Fujisaki for her assistance in the preparation of this manuscript.