Article Text

Abstract
OBJECTIVES Rheumatoid arthritis (RA) is a chronic disease characterised by irreversible destruction of the affected joints. As aggressive transformed-appearing synovial fibroblasts are commonly found at the site of invasion of the rheumatoid synovium into the adjacent cartilage and bone, the presence of microsatellite instability (MSI) and expression of mismatch repair enzymes as a possible mechanism in the alteration of these cells was examined.
METHODS DNA was extracted from the synovial fibroblasts and blood of 20 patients with long term RA undergoing joint replacement, and the presence of MSI was studied at 10 microsatellite loci. In addition, immunohistochemistry was performed to evaluate the expression of the two major mismatch repair enzymes (hMLH1 andhMSH2) in rheumatoid synovium.
RESULTS MSI could not be detected in any of the fibroblast cell populations derived from the 20 different rheumatoid synovial samples. In addition, strong expression of mismatch repair enzymes could be seen in numerous cells, including fibroblasts, throughout the synovium.
CONCLUSIONS Applying the currently used and established markers for MSI, the data show for the first time that MSI does not appear to have an important role in alteration of rheumatoid synovial fibroblasts into an aggressive phenotype. On the other hand, strong mismatch repair enzyme synthesis in rheumatoid synovium supports the hypothesis of continuing DNA repair, presumably due to long term, inflammation induced DNA damage.
- rheumatoid arthritis
- synovial fibroblasts
- microsatellites
- mismatch repair enzymes
Statistics from Altmetric.com
Rheumatoid arthritis (RA) is a chronic disease characterised by altered immune responses, inflammation, and synovial hyperplasia, resulting in irreversible destruction of the affected joints. In the past, numerous data showed that synovial fibroblasts, which are found at the site of invasion of rheumatoid synovium into the adjacent cartilage and bone, are important players in the pathophysiology of RA.1
After initial stimulation, cellular activation of the rheumatoid synovial fibroblast is reflected by an enhanced gene transcription, and the upregulation of proto-oncogenes. Subsequently, increase in cellular activity results in longlasting alterations of the cell cycle, followed by prolonged production of matrix degrading enzymes.1 A potential mechanism that may be operative in rheumatoid synovium and lead to these alterations is the accumulation of somatic mutations during the course of the disease owing to persistent inflammation. Little is known about genomic mutations in rheumatoid synovium and in rheumatoid synovial fibroblasts, and it was shown recently that one of the candidates for cellular transformation, the p53 tumour suppressor gene, is overexpressed in rheumatoid synovium,2 but that most mutations are not located in the rheumatoid synovial fibroblasts.3 Therefore, we searched for other known cell transforming mechanisms that might be operative in rheumatoid synovium.
One of the most exciting areas of cancer research in the past years has been the discovery that instability of DNA sequences is a pathophysiological mechanism underlying the development of a wide variety of inherited and sporadic malignant diseases.4 ,5A new pathway in the production of tumours was found by the detection of DNA mismatch repair genes and their ability to correct DNA replication derived somatic mutations.6 ,7 Until now, seven DNA mismatch repair genes have been identified in humans (hMSH2, hMSH3,hMSH5, hMSH6,hMLH1, hPMS1, andhPMS2), which, in the case of biochemical inactivation induced by biallelic mutation, cause a distinct genomic phenotype termed microsatellite instability (MSI). MSI is defined as alteration of the length of simple repetitive genomic sequences (microsatellites), which can be visualised by comparing tumour with matched DNA of the same person.
Various tumours have been investigated for the presence of MSI. It has been found in gastric, endometrial, lung, bladder, and oropharyngeal cancer,8 and is most commonly localised in colorectal cancers of patients with hereditary non-polyposis colorectal cancer syndrome.9 In addition to inherited non-polyposis colorectal cancer, we found MSI in up to 15% of patients with sporadic colorectal cancer.10 ,11 Of interest, MSI appears not to be limited to malignant and premalignant diseases. For example, it has been detected in inflammatory diseases such as pancreatitis.12 As MSI has not been evaluated in rheumatoid synovial fibroblasts, the histomorphological feature of aggressive invasion of these fibroblasts into the adjacent cartilage and bone motivated us to search for MSI as a possible pathophysiological pathway in the metabolic alteration of these cells.
Recently, a panel of 10 reference loci was established for determination of the presence of MSI.13 In addition, expression of the MMR genes hMLH1 andhMSH2 are of particular interest, as their biochemical inactivation contributes to most cases of hereditary non-polyposis colorectal cancer showing MSI.14 Therefore, we examined the DNA of rheumatoid synovial fibroblasts for MSI, and rheumatoid synovium for the presence of the mismatch repair geneshMLH1 and hMSH2.
Methods
PATIENTS
Peripheral blood samples and synovial tissues were obtained from 20 patients with long term RA undergoing joint replacement at the department of orthopaedics at the University of Regensburg. Before the operation informed consent was obtained from each patient, and the project was approved by the local ethics committee.
MICROSATELLITE INSTABILITY ANALYSIS
DNA was extracted from cultured synovial fibroblasts after four to six passages and from matching germline controls (peripheral blood samples) by standard procedures,3 and MSI analysis was performed as described recently.12 ,15 In brief, DNA was examined for genetic alterations at microsatellite loci BAT25, BAT26, BAT40, D5S346, D17S250, D2S123, D10S197, D18S58, D18S69, and MYCL1. Polymerase chain reaction (PCR) amplifications were performed with 100 ng of purified genomic DNA in a final volume of 20 μl in an MJ Research Thermocycler (PTC100; MJ Research, Watertown, MA). Subsequently, PCR products were analysed by 6.7% polyacrylamide/50% urea gel elctrophoresis (one hour, 1500 V, 50°C) in a SequiGen sequencing gel chamber (Bio-Rad, Hercules, CA) and by silver nitrate staining as described previously.16
AUTOMATED PCR FLUORESECENCE ANALYSIS
In addition to conventional PCR-polyacrylamide gel analysis, five microsatellite loci were also analysed by automated, fluorescence based PCR. In brief, five fluorescein labelled primer sets for microsatellite loci BAT25, BAT26, D17S250, and APC were used for amplification of the same synovial fibroblast and corresponding whole blood DNA as mentioned above. For PCR amplification and analysis an ABI PRISM fluorescence cycler (Perkin Elmer Cetus, Norwalk, CT) in combination with GeneScan 2.1 software was used according to the protocol of the producer.
DETERMINATION OF MICROSATELLITE INSTABILITY
MSI was determined, after PCR amplification of fibroblast DNA, by the presence of new bands or band shifts which were not present in PCR products of the corresponding normal DNA.13 To decide on those markers, in which band shifts were difficult to interpret, all gels were evaluated independently by three different observers. According to established classification criteria, microsatellites were defined as highly unstable if at least 40% of the analysed loci showed instability, whereas <40% instability was classified as “low microsatellite instability” and 0% was classified as stable.13
IMMUNOHISTOCHEMISTRY
To determine mismatch repair enzyme expression, all synovial specimens were examined by immunohistochemical analysis with the streptavidin-biotin-peroxidase complex method using 3,3′-diaminobenzidine as chromogen. After deparaffinisation, 4 μm synovial sections were pretreated by microwave (quadruplicate application of four minutes at 900 W in 0.1 M citrate buffer).13 ,15 ,16 After a blocking step, sections of paraffin embedded tissue samples were incubated with a polyclonal rabbit antibody against hMSH2 (Clone FE11, 0.5 μg/ml; Oncogene, Cambridge, MA), and a serial section was incubated with a mouse monoclonal antibody againsthMLH1 (Clone G168–728, 1 μg/ml; Pharmingen, San Diego, CA), overnight at 4°C. Colour development was performed according to established protocols,13 ,15 ,16and serum samples from normal mouse were used as negative controls.
Results
Microsatellite gene loci of all patients could be amplified by the complete primer set. MSI, which would have been characterised by allele shift, allele deletion, or additional alleles in the fibroblast DNA, was found in none of the 20 patients examined. In comparison with the matching blood DNA, the cultivated synovial fibroblasts showed identical patterns of bands on the gel electrophoresis at all 10 MSI loci, indicating a general lack of MSI. Figure 1A illustrates a representative microsatellite analysis of an MSI locus (D2S123) of 10 different patients with RA. In addition, using fluorescence PCR, amplification of gene segments of five microsatellite loci was achieved. As with conventional PCR analysis, alterations in the allele pattern were not found in any of the five loci examined, thus confirming the lack of MSI within the rheumatoid fibroblast genome. Figure 1B illustrates an analysis of one patient (fibroblastv whole blood DNA) showing an identical allele pattern in two of the five loci investigated.

Polymerase chain reaction (PCR) based microsatellite instability (MSI) analysis using primers for the microsatellite locus D2S123 (fig 1A) showing patients RA01– RA10. Lane pairs 1–10 show an identical allele pattern for DNA derived from peripheral blood (1B–10B) and from synovial fibroblasts (1F–10F) of the same patients. Arrows indicate DNA markers for 100 bp (arrow) and 200 bp (arrowhead). Figure 1B shows a cumulative analysis of patient RA04 performed with fluorescence based PCR using two different primer sets (BAT25 and BAT26). No difference in allele pattern can be seen in the two loci, indicating a lack of MSI.
IMMUNOHISTOCHEMISTRY
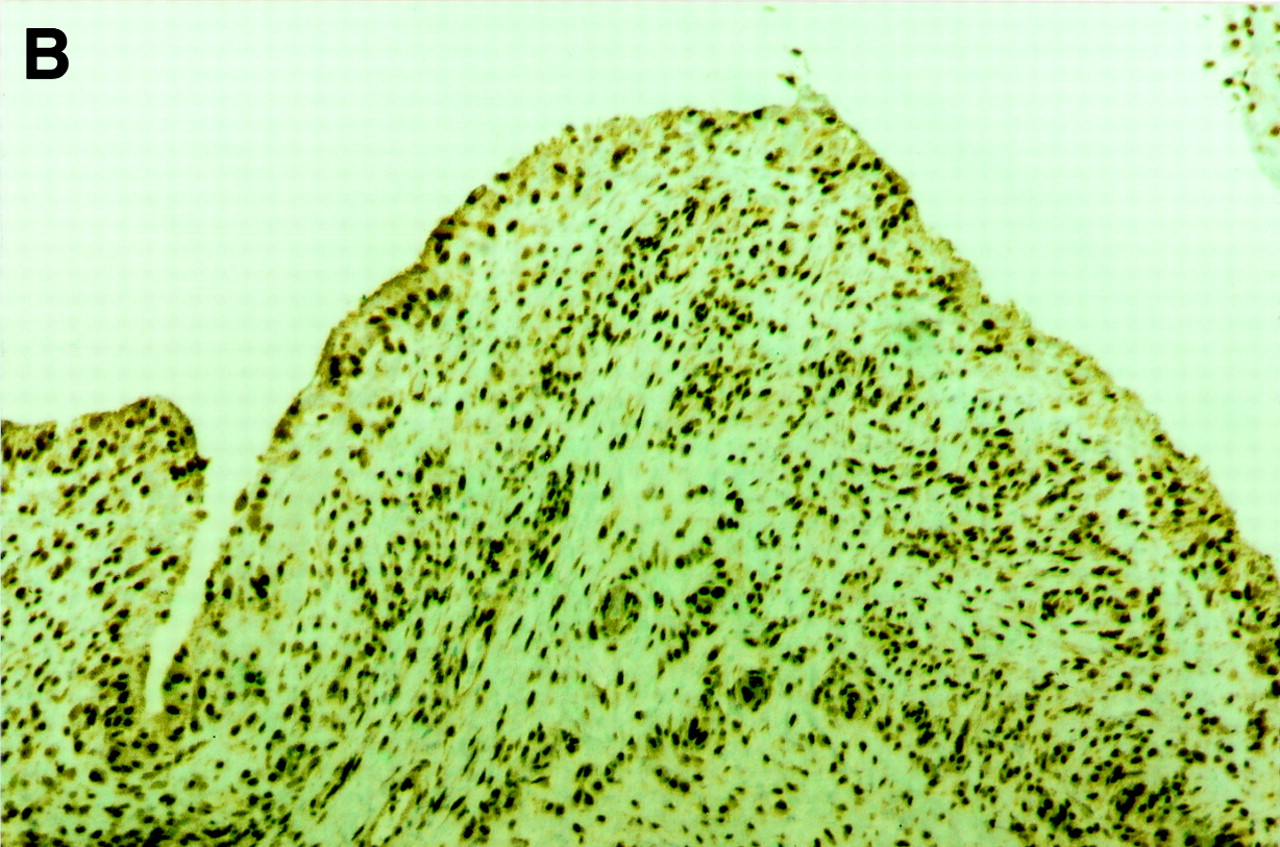
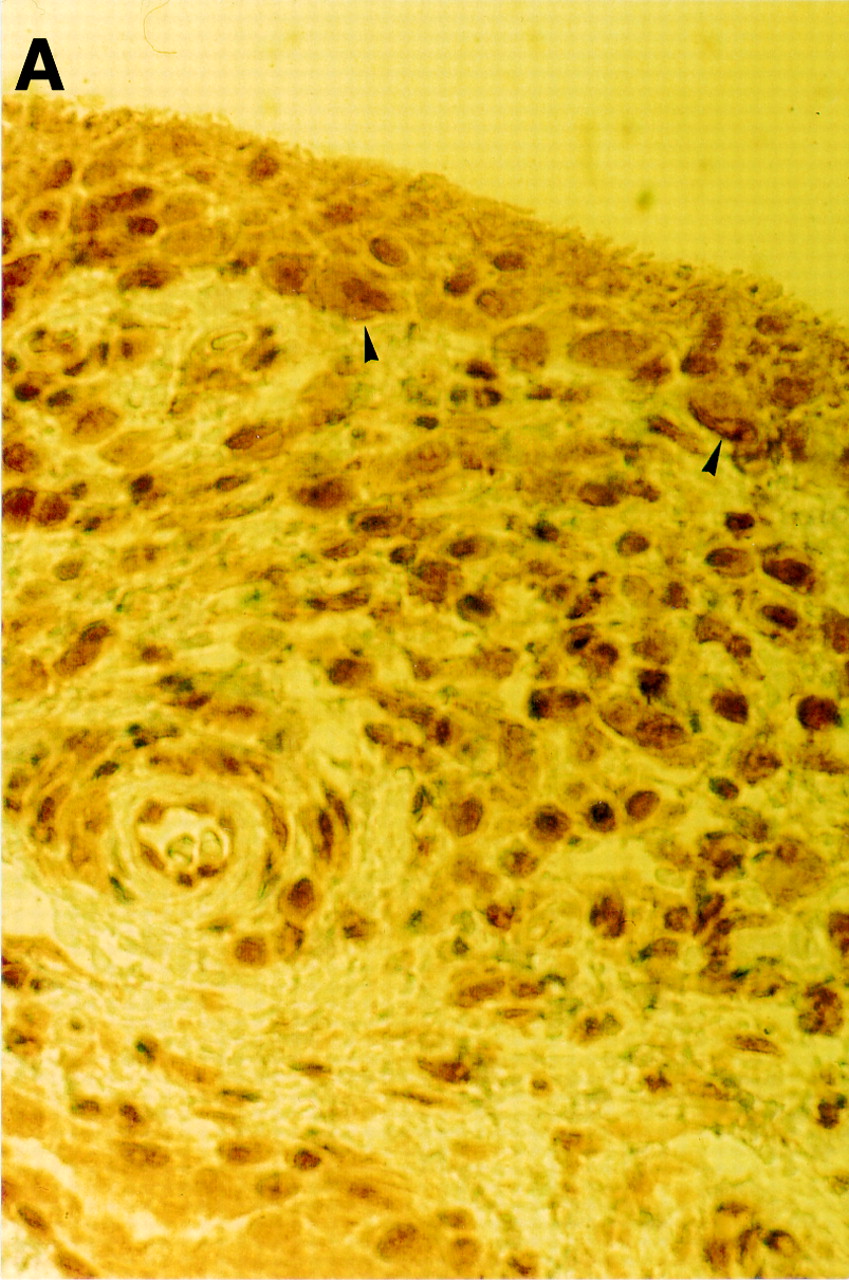
Strong expression of mismatch repair enzymes could be seen in all synovial tissue samples. Cells expressing eitherhMLH1 or hMSH2could be found throughout the synovium, including fibroblast-like cells, macrophage-like cells, and mononuclear cells, indicating intensive DNA repair within the rheumatoid synovium, and—in combination with the lack of MSI—no deficiency in DNA mismatch repair activity. Figure 2 shows serial sections for demonstration of thehMLH1 and hMSH2protein in a synovial sample of a patient with RA analysed by peroxidase based immunohistochemistry, and table 1 shows a semiquantitative analysis of hMLH1 andhMSH2 expression as compared with osteoarthritis synovial and different colon tissue samples also examined.

{kind=link}
{kind=link}
{kind=link}
Paraffin embedded rheumatoid synovium section. Peroxidase based immunohistochemistry showing an intensive brown cellular staining for the hMLH1 protein (fig 2A) in numerous cells throughout the synovium including transformed appearing synovial fibroblasts (arrowheads). Original magnification ×640. An identical distribution pattern is seen for the hMSH2 protein (fig 2B). Original magnification ×80.
Expression of hMLH1 and hMSH2 in different tissue specimens. The semiquantitative analysis shows the number of cells positive for hMLH1 or hMSH2
Discussion
Here, we present the first study to evaluate MSI in synovial fibroblasts from patients with RA. Taken together, synovial fibroblasts of patients with RA did not show MSI in any of the gene loci validated and currently used to determine MSI in malignant disease, especially in colon carcinoma.13 However, the possibility cannot be excluded that this panel of 10 microsatellite loci might lack sensitivity for analysis of potentially important MSI in rheumatoid synovial fibroblasts in loci hitherto unknown. The latter argument is supported by the presence of 50–10 000 microsatellites located throughout the human genome.17
There is a body of evidence that chronic inflammation seen in rheumatoid synovium may cause somatic mutations, resulting in transformation of synovial cells forming the aggressive synovium that invades and degrades the adjacent cartilage and bone.1 As immunohistochemistry showed an intensive expression of both major DNA mismatch repair enzymes, hMLH1and hMSH2, especially when compared with the expression in colonic tumour tissue positive for the investigated mismatch repair gene (table 1), it is most likely that this strong expression may reflect a continuing, but functionally intact, repair process of inflammation induced DNA damage.
In summary, our data show for the first time that applying the currently used loci and criteria for MSI, there is no evidence that MSI does have a considerable role in phenotype alteration of rheumatoid synovial fibroblasts. In addition, as the rheumatoid synovium showed an intensive expression of the mismatch repair enzymes,hMLH1 and hMSH2,the hypothesis can be proposed that an increased instability of tracts of nucleotide repeats in the genome of various synovial cells is induced by persistent synovial inflammation, which requires constant DNA repair by functionally intact mismatch repair enzymes.
Acknowledgments
This study was supported by grants from the German Research Society (DFG), Nos 1383/1–1 and Ku 792/6–1.