Article Text

Abstract
OBJECTIVE The aim of this study was to evaluate left ventricular filling in patients with rheumatoid arthritis (RA), analysing transmitral flow and pulmonary venous flow, with special regard to age and disease duration.
METHODS 32 patients affected by RA according to ARA criteria were selected, without evidence of cardiac disease, and compared with matched control subjects. All patients and the control group were submitted to M-mode, two dimensional, Doppler and colour Doppler (continuous and pulsed wave) echocardiography. The following diastolic parameters were evaluated: transmitralic flow (E/A ratio), pulmonary venous flow (S/D ratio), a-Pw, IVRT and DT.
RESULTS In RA patients left ventricular filling abnormalities were found characterised by a reduced E/A ratio (mean (SD) 1.16 (0.31) vcontrols 1.37 (0.32); p =0.02) and an increased S/D ratio (1.43 (0.40)v controls 1.22 (0.29); p = 0.017). In the group of patients a relation was found between E/A ratio and disease duration (r= 0.40, p =0.01 Spearman rank correlation).
CONCLUSIONS At present, it is concluded that RA patients, in absence of clinical evidence of heart disease, show diastolic dysfunction characterised by impaired E/A and S/D ratio. The relation between transmitral flow alteration and disease duration suggests a sub-clinical myocardial involvement.
- diastolic function
- rheumatoid arthritis
- transmitralic flow
- pulmonary venous flow
Statistics from Altmetric.com
Long term survival of patients with rheumatoid arthritis (RA) is shorter compared with the general population or control subjects without RA.1 Among the different causes of death, increased mortality from heart disease with high prevalence of congestive heart failure was reported in many studies.1 ,2Necropsy studies showed a high incidence of pericardial, myocardial and endocardial involvement in RA patients.3 However, cardiac disease is often clinically silent and is rarely a severe life threatening complication in RA. Cardiac failure is the result of either systolic or diastolic dysfunction, or both. Left ventricular (LV) diastolic dysfunction is usually attributable to common structural abnormalities such as hypertrophy or interstitial fibrosis and impaired myocyte relaxation resulting from ischaemia.4 Doppler echocardiography is a sensitive, and non-invasive method of detecting cardiac abnormalities and systolic and/or diastolic function.
The aim of this study was to evaluate left ventricular filling abnormalities in RA patients, without apparent cardiovascular disease, with special regard to age and disease duration.
Methods
The study was carried out on 32 outpatients (four men and 28 women, mean (SD) age 50 (10), range 34–65 years) attending the Rheumatology Unit of the University of Rome “ La Sapienza”. All patients were affected by RA according to ARA criteria of 1987.5 Duration of disease ranged from 3 to 26 years (mean (SD) 9 (6)). Informed consent was obtained from subjects enrolled and the study was approved by the local ethics committee. Thirty three normal subjects, (eight men and 24 women, mean (SD) age 49 (7), range 38–65 years) were selected as controls. None of the subjects included in this study had evidence of cardiac disease, hypertension or diabetes mellitus as assessed by history, physical examination and standard 12-lead ECG. All patients were checked for number of tender and swollen joints and submitted to laboratory investigations including erythrocyte sedimentation rate (ESR), C reactive protein (CRP), complete blood count, serum protein electrophoresis, serum creatinine, serum transaminases, rheumatoid factor (latex agglutination test) and anti-nuclear antibody.
ECHOCARDIOGRAPHY
The study was performed using an Hewlett-Packard Sonos 2000 ultrasound imaging system with a 2.0–2.5 MHz transducer. All patients and control group were submitted to M-mode, two dimensional and Doppler and colour Doppler (continuous and pulsed wave) echocardiography. The cardiac chamber dimensions and wall thickness were obtained from M-mode echocardiography. Left ventricular mass was calculated by M-mode measurements at end-diastole by Penn convention.6Fractional shortening (FS) and ejection fraction (EF) according to Simpson's formula were calculated. Segmental LV function was evaluated using two dimensional long axis and short axis parasternal views and four chamber apical view. Doppler echocardiography was used to obtain transmitral flow and pulmonary venous flow determined from the apical four chamber view. To record transmitral flow the sample volume was carefully positioned at the tip of the leaflets of mitral valve. The following variables were evaluated as parameters of left ventricular filling: peak of early diastolic (E) and late diastolic (A) flow velocity, E/A ratio, deceleration time of flow velocity in early diastole (DT) and isovolumic relaxation time (IVRT). To obtain pulmonary venous flow the sample volume was placed at the orifice of the left anterior pulmonary vein. The variables measured included peak pulmonary venous flow velocity during ventricular systole (S), peak pulmonary venous flow velocity during ventricular diastole (D), S/D ratio and peak reverse pulmonary venous flow velocity at atrial contraction (A-pw). The echocardiographic images were examined by two blinded investigators and no significant interobserver variability was detected.
STATISTICAL ANALYSIS
Data are given as mean (SD). The statistical analysis Wilcoxon's rank sum test and χ2 test were used. A value of p < 0.05 was considered statistically significant. Spearman's correlation coefficient test was used to explore the relation between the study variables.
Results
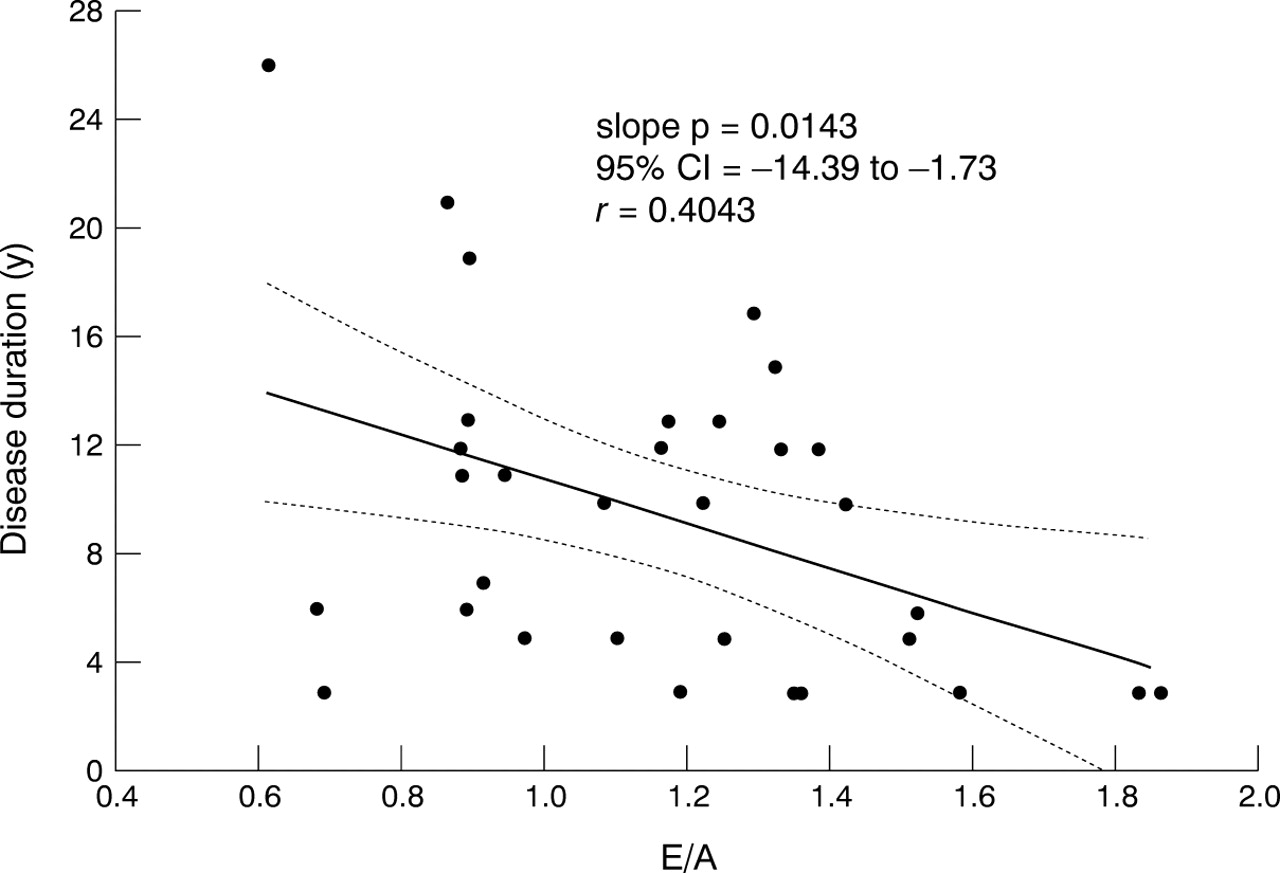
There were no differences between the two groups regarding ventricular cardiac chambers dimensions, left ventricular mass and wall thickness, except for the left atrial cavity dimension (p=0.03) (table1). None of the control group or the group of patients had left ventricular wall motion abnormalities and both groups had normal systolic function. In RA patients we have found abnormalities of the left ventricular filling characterised by a reduced E/A ratio (p = 0.02) and an increased S/D ratio (p = 0.02) (table 1). We did not find any statistically significant differences regarding other diastolic filling parameters. Moreover in the group of patients we found a relation between E/A ratio and disease duration (r= 0.40, p =0.01; fig 1). There was no statistically significant correlation between all echocardiographic parameters and disease activity , presence of rheumatoid factor, number of joints involved or Ritchie index.
Echocardiographic and Doppler variables in patients and control subjects

{kind=link}
Scatterplot of the relation between mitral E/A wave velocity ratio and disease duration.
Discussion
The main feature of our study was the selection of patients affected by RA, without clinical evidence of heart disease and their comparison with a control group matched for sex and age. Our results show significant differences between RA patients and the control group in left atrial size and diastolic function of the left ventricle assessed by transmitral flow (TF) and pulmonary venous flow (PVF), in absence of systolic abnormalities. The use of the Doppler echocardiography technique to obtain left ventricular filling profile from TMF is considered a reliable method.7 In addition, during diastole, left ventricle, left atrium and pulmonary veins form a “common chamber” that is continuous with the pulmonary capillary bed.4 Therefore the evaluation of PVF in addition to TF could represent a further parameter of diastolic function.8 Previous studies showed abnormalities in diastolic function in RA patients assessed by TF,9 ,10 and as far as we know, our study is the first report aimed at investigating diastolic function also assessed by PVF. Our results confirm abnormalities of TF characterised by a reduced E/A ratio, and also show changes of PVF, with increased S/D ratio, in RA patients compared with controls. In agreement with other reports9 ,11 we did not find any correlation between disease activity parameters, clinical findings, articular impairment and diastolic function abnormalities. The progressive impairment of diastolic function with age is well known,12 but in our study the age of the patients was matched with the control group and there was no statistically significant difference in the mean age. No difference in LV mass between patients and controls was found. Moreover increased LV mass in RA is still debated.10 ,11 ,13 The diastolic function abnormalities that we found, in absence of LV hypertrophy, could suggest an intrinsic myocardial abnormality. In fact histopathological studies have reported non-specific myocarditis, granulomatous lesions in myocardium, secondary amyloidosis, coronary vasculitis and diffuse fibrosing lesions in RA.14 So, these lesions could be responsible for abnormal left ventricular filling and consequently for mild left atria enlargement. In our study we found a statistically significant correlation between disease duration and alteration of diastolic function expressed by E/A ratio, independently from the age of disease onset. This result is in agreement with a recent report15 that showed a correlation between disease duration and an index of LV relaxation evaluated by M-mode echocardiography (+dD/dt); those results were not found by using Doppler index (E/A). It is possible that the longer period of disease of our patients caused a more evident diastolic dysfunction. In conclusion, we found a relation between diastolic dysfunction expressed by E/A ratio and disease duration in RA patients without clinical evidence of heart disease, independently from the age of disease onset. These findings suggest a sub-clinical myocardial involvement during the course of disease.
Acknowledgments
We gratefully acknowledge Ennio Rinaldi for echocardiographic technical assistance.