Article Text

Abstract
OBJECTIVES Stress proteins (HSPs) are highly conserved immunodominant antigens found in various species. The purpose of this study was to assess the prevalence and prognostic significance of antibodies to HSC 70 kDa and HSP 90 kDa in three groups of patients with longstanding rheumatoid arthritis (RA) defined based on the severity of articular erosions.
METHODS 73 patients with longstanding (> 6 years) RA whose HLA-DR genotype was known were divided in three groups according to Larsen’s score and compared with 47 recent onset (<1 year) RA patients and with control groups composed of patients with other inflammatory diseases (n=137) or of normal controls (n=48). IgGs and IgMs to HSC 70 kDa and HSP 90 kDa were determined using an ELISA with purified bovine HSC 70kDa or HSP 90 kDa.
RESULTS Concentrations of IgGs and IgMs to HSC 70 were significantly increased in 41.1% and 42.5% of longstanding RA patients, respectively. Corresponding figures for IgGs and IgMs to HSP 90 were 39.7% and 56%. IgMs to HSC 70 and HSP 90 were less frequent in recent onset RA (19% and 13% respectively). Among the groups with other inflammatory diseases, only the MCTD group exhibited high frequencies of IgGs to HSC 70 (80%) and HSP 90 (85%). DRB1*0401 positive RA patients (n=23) were not more likely to have increased concentrations of antibodies to HSC 70 kDa or HSP 90 kDa than other RA patients (DR4 positive but DRB1*0401 negative, or DR1 positive, n=31; or negative for both DR4 and DR1, n=14). IgGs to HSP 90 kDa were significantly more frequent (p<0.05) in longstanding RA patients whose Larsen’s score was 4 or more (57%) than in those whose Larsen’s score was 2 or 3 (39.4%) or less than 2 (16%). No associations were found between Larsen’s score and IgGs or IgMs to HSC 70 kDa or IgMs to HSP 90 kDa. A significant correlation was demonstrated between IgGs to HSP 90 kDa and two other serological markers for RA, rheumatoid factor, and anti-Sa antibody; there were no correlations with antikeratin antibody, antiperinuclear factor, or anti-RA 33.
CONCLUSION IgGs to HSP 90 kDa are most common in longstanding RA patients with articular erosions, suggesting that they may be related to the articular prognosis in RA
- rheumatoid arthritis
- heat shock proteins
- prognosis
Statistics from Altmetric.com
Heat shock proteins (HSPs), also called stress proteins, are highly conserved between prokaryotes and eukaryotes. Concentrations vary from low or moderate in non-stressed cells to very high in cells subjected to stressors including heat, attack by reactive oxygen metabolites, and metabolic disruption induced by low pH, anoxia or toxins.1
HSPs are classified based on molecular size, sequence similarities, location within the cell, and function.2 Group 70 stress proteins maintain proteins in an unfolded, extended conformation. At least five members have been recognised among the Group 70 family: hsp 70 is characterised by some expression under basal conditions, hsp 72 by absence of basal expression and by a high level of inducibility, and hsp 73 (also called HSC 70) by a high level of basal expression and a low level of inducibility by heat. The remaining two members of the Group 70 family are GRP 78, which is located in the endoplasmic reticulum and is characterised by a high level of basal expression, and GRP 75, which is in the mitochondria.3
The HSPs are immunodominant antigens of various micro-organisms including mycobacteria. A large body of data from the adjuvant arthritis model in rats and from rheumatoid arthritis (RA) patients suggest that T cells exhibit high reactivity with microbial HSPs, most notably HSP 65 kDa of mycobacteria.4-8
In humans, B cell reactivity to mycobacterial HSP 65 kDa has been reported in RA patients.9-16 These findings, together with the conserved nature and immunogenicity of HSPs, suggest that molecular mimicry may cause a breakdown in tolerance to self if an immune response to a microbial HSP results in a cross reaction against either human HSP or another self protein.
This study describes an ELISA for autoantibodies to HSC 70 (hsp 73) and HSP 90 in patients with RA and other inflammatory joint diseases. Increased concentrations of IgGs and IgMs to HSC 70 and HSP 90 have been reported in patients with RA, mixed connective tissue disease (MCTD),17 and systemic lupus erythematosus (SLE).18-21 Among RA patients, IgGs to HSC 70 and HSP 90 were detected as early as the first year of the disease. Patients with longstanding non-destructive RA were less likely to have positive serum tests for anti-HSP 90 IgGs than patients with destructive RA.
Methods
PATIENTS AND SERUM SAMPLES
Venous blood was obtained from selected non-consecutive patients with the following diagnoses: RA (n=120), psoriatic arthritis (n=30), ankylosing spondylitis (n=30), MCTD (n=21), SLE (n=10), primary Sjögren’s syndrome (SS; n=28), and progressive systemic sclerosis (PSS; n=28).
Forty eight normal subjects served as the controls. Patients with RA according to the 1987 ARA criteria22 were divided into two groups based on whether they had recent onset RA defined as a disease duration of less than one year (n=47; 37 women and 10 men; mean age at symptom onset, 50 years (range 18–22)) or longstanding RA defined as a disease duration of at least six years (n=73; 59 women and 14 men; mean age at symptom onset 43 years (range 18–69)). The patients with longstanding RA were from a vast cohort of RA patients receiving regular follow up, including radiographs and immunogenetic studies, at the same institution from the first year of their disease. Larsen’s stage was determined after a disease duration of six years at the following sites: fingers and wrists, feet, and any site with arthritis (definition of Larsen stages (grades): stage 0 = normal joint; stage 1 = soft tissue swelling; stage 2 = erosion with <25% destruction of the articulating joint surface area; stage 3 = extensive erosions and > 25% destruction of the articulating joint surface area; stage 4 = > 50% destruction of the articulating joint surface area; stage 5: more than 75% destruction of the articulating joint surface area). Patients were categorised into three groups based on whether the hands Larsen’s stage modified by Rau and Herborn23 was: =4 (n=21), 2 or 3 (n=33), or<2 (n=19).
Anti-HSP antibodies were compared across groups.
STUDY DESIGN
Bovine brain constitutive HSC 70, bovine brain inducible HSP 90, and rat or mouse monoclonal antibodies to both these HSPs were from Stressgen (Victoria, Canada, ref SPP 750 and SSP 780). Dynatech ELISA microtitre plates were coated overnight at 4°C with 100 μl/well of purified HSC 70 or HSP 90 in a concentration of 1 μg/ml in 0.05 M bicarbonate buffer pH 9.4. Serum samples were diluted to 1:50 in phosphate buffered saline (PBS) with 2% bovine serum albumin (BSA). One hundred microlitres of each serum were added to the ELISA plate in duplicate. After incubation for two hours at room temperature followed by five washings with PBS and Tween 20 (PBS-Tween), 100 μl each of peroxidase conjugated goat antihuman IgG and IgM (Cappel USA) in concentrations of 1:3000 and 1:2000, respectively, in PBS-BSA were added. The plates were incubated for another two hours at room temperature then washed five times with PBS-Tween. One hundred microlitres orthophenylene diamine (OPD, 0.25 mg/ml) in citrate buffer pH 5.0 was added, and the colour reaction was allowed to develop. The reaction was stopped after five minutes by addition of 50 μl of SO4H2 2.5 N. The plates were read using a Dynatech ELISA reader at 492 nm. These conditions were defined based on a series of preliminary experiments. The ELISAs used in our study were initially developed using rat and mouse monoclonal antibodies to HSC 70 and to HSP 90 (Stressgen Victoria, Canada, ref SPA 835 and SPA 815) 1 μg/μl diluted to 1/100 as the first antibody, and peroxidase conjugated goat antimouse or antirat antibodies as the second antibody. Optical density (OD) values obtained from uncoated wells were subtracted from those from antigen coated wells, yielding the corrected OD value. Serum samples were considered anti-HSP positive if the corrected OD value was greater than the mean (+3 SD) in 48 healthy controls.
To avoid day to day fluctuations, each plate included five serum samples from healthy subjects (negative controls) and monoclonal murine anti-HSC 70 and HSP 90 (positive controls). Interassay variation was 12%.
DATA ANALYSIS
Values are given as the mean (SD). Differences in the frequencies of anti-HSP antibodies across patient groups were assessed using parametric statistical tests. Depending on the data type, either Fisher’s exact test (for discrete variables) or the χ2test (with Yates’s correction when appropriate) were applied. All probability values were two tailed. Relative risks and odd ratios with their 95% confidence intervals were calculated for various parameters. Sensitivity and specificity were also calculated. p Values of less than 0.05 (or less than 0.0125 after correction for multiple comparisons using the Bonferroni method) were considered significant. The non-parametric Kruskal-Wallis analysis of variance was used to compare titre values across diagnostic groups. Dunn’s multiple comparisons test was used to narrow the range of patient values that were significantly different from control values. All statistical analysis were performed using Instat statistical software for Macintosh (Graph Pad software version 2.01).
IMMUNOGENETIC ANALYSIS
HLA DR genetic oligotyping was performed using a non-radioactive reverse dot blot technique as described elsewhere.24 The nucleotide sequence of the primers used for the polymerase chain reaction (PCR) was chosen in the conserved region of the second exon of the HLA DRB1 gene. A set of 15 sequence specific oligonucleotides (SSOs) was used for DRB1 genetic oligotyping in RA patients. DRB1*01 and DRB1*04 subtyping was done using sequence specific primers (SSP) and PCR amplification.
Results
Increased concentrations of anti-HSC 70 IgGs were found in 30 (41.1%) of the 73 longstanding RA patients and 25 (53%) of the 47 recent onset RA patients. Corresponding figures for anti-HSC IgMs were 31 (42.5%) and 9 (19%) (χ2 = 6.99; p<0.01). Similar results were obtained for anti-HSP 90 IgGs and IgMs (table 1) with a significant difference between the two groups for IgM anti-HSP 90 (χ2 = 22.6; p<0.001). Mean concentrations of anti-HSC 70 IgG and anti-HSP 90 IgG were significantly higher in patients with longstanding RA than in normal controls (p = 0.001). Similar results were obtained for anti-HSC 70 IgM and anti-HSP 90 IgM (p<0.001). Mean concentrations of anti-HSC 70 or HSP 90 IgMs or IgGs (fig 1 and 2) were not significantly different in patients with longstanding RA and in those with recent onset RA. This difference was not related to a difference in mean patient age. Among patients with longstanding RA, no statistically significant difference was seen between the 41 patients younger than 50 years and the 32 patients older than 50 years at RA onset regarding anti-HSC 70 or HSP 90 IgG or IgM: 39%v 40.6% for HSC 70 IgG, 46.3%v 34.4% for HSC 70 IgM, 31.7%v 46.9% for HSP 90 IgG, and 53.6%v 56.2% for HSP 90 IgM.
IgG and IgM reactivity with HSC 70 and HSP 90 proteins by ELISA (results are percentages)

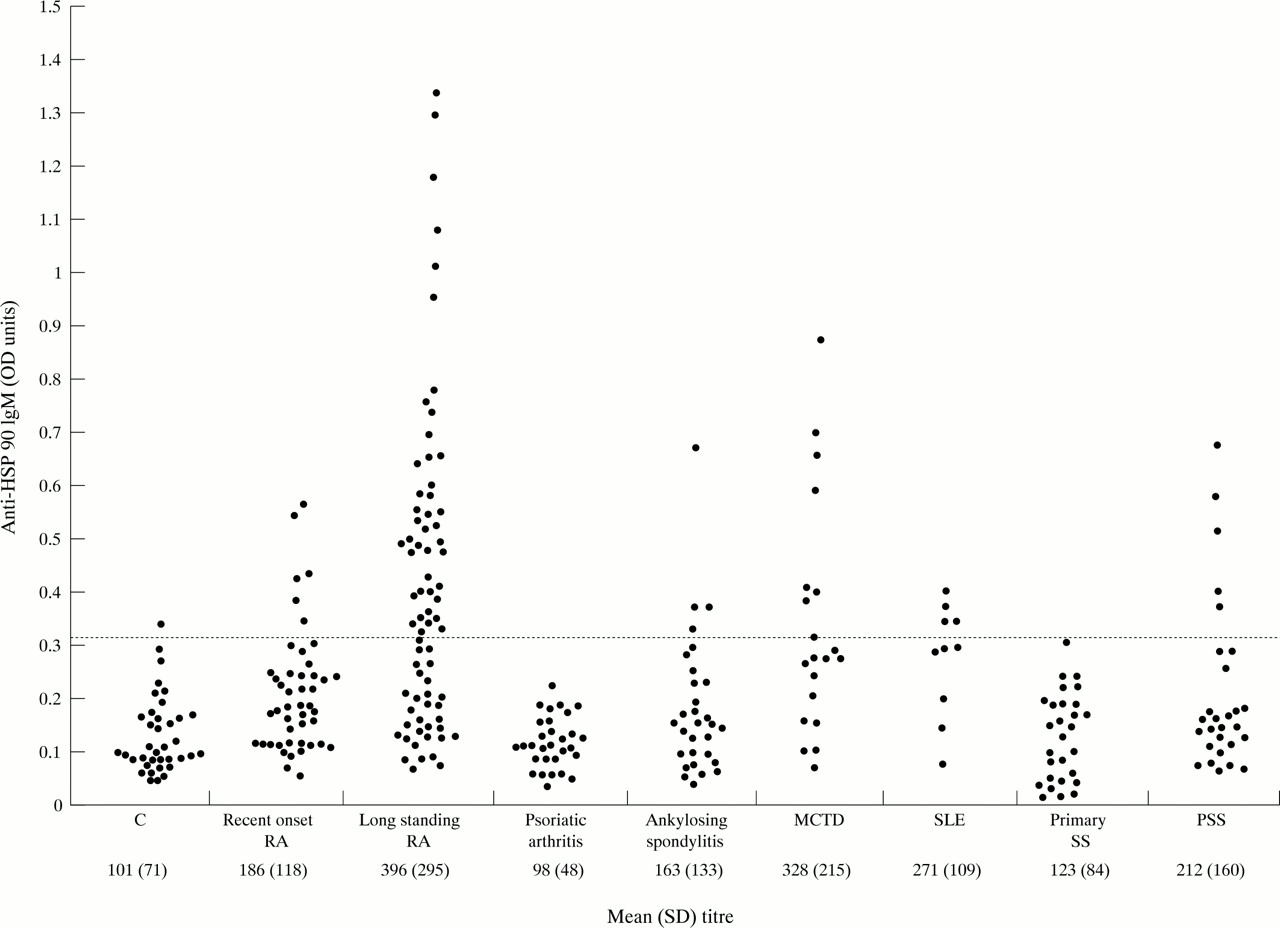
Concentrations of IgG antibodies to heat shock protein (HSP) 90 in patients with recent onset RA, longstanding RA, psoriatic arthritis, ankylosing spondylitis, mixed connective tissue disease (MCTD), systemic lupus erythematosus (SLE), primary Sjögren’s syndrome (SS), progressive systemic sclerosis (PSS), and normal controls (C). The upper limit of normal is indicated by a broken line.

Concentrations of IgM antibodies to heat shock protein (HSP) 90 in various groups of patients (see legend fig 1).
Increases in anti-HSC 70 and anti-HSP 90 were infrequent in patients with joint diseases other than RA, except those with U1-RNP antibodies—that is, with either MCTD or SLE: anti-HSC-70 IgGs were increased in 80% of MCTD and SLE patients, and anti-HSP 90 IgGs in 85% of MCTD and 70% of SLE patients (fig 1). Most MCTD and SLE patients were negative for anti-HSC 70, and 30% were positive for anti-HSP 90 IgMs. In most of the other diagnostic groups, few, if any, patients had anti-HSC 70 or anti-HSP 90 (table 1). Specificities for the diagnosis of RA of anti-HSC 70 IgGs and IgMs and of anti-HSP 90 IgGs and IgMs were 81.6%, 97.3%, 81%, and 92.5%, respectively, and the corresponding odds ratios were 3.93 (95% CI 1.6, 5.7); 25.7 (95% CI 8.6, 162); 1.4 (95% CI 0.76, 2.6); 15.3 (95% CI 1.4, 65).
The 38 recent onset RA patients received regular follow up during the first two years of their disease with collection of serial serum samples at six to12 month intervals (93 serum samples). Changes from negative to positive or from positive to negative were uncommon (table2): seven (18%) of the patients with increased anti-HSP 90 IgGs at baseline were negative for this antibody at the end of the two year follow up period, and none without anti-HSP 90 IgG increase at baseline were positive for this antibody at the end of the two year follow up period.
Recent onset RA patients. Serial determinations of anti-HSC 70 and anti-HSP 90 IgG and IgM (38 RA patients, 93 serum samples)
In RA patients, the only anti-HSP antibody that was associated with rheumatoid factor (RF) status was anti-HSP 90 IgG: 51% of RF positive RA patients compared with 21.4% of RF negative RA patients had increased anti-HSP 90 IgGs (χ2c = 5.17, uncorrected p <0.03). When correlations were looked for between increase in anti-HSC 70 or anti-HSP 90 and diagnostic markers for RA (antikeratin antibody, antiperinuclear factor, anti-RA33) in recent onset RA (data not shown) or in longstanding RA (table 3), the only correlation found was between anti-Sa antibody and IgG anti-HSP 90 (χ2c = 3.85; uncorrected p<0.05).
Frequencies (%) of anti-HSC 70 IgG and IgM and anti-HSP 90 IgG and IgM in 73 longstanding RA patients with or without serological markers for adult RA (RF: rheumatoid factor; AKA: antikeratin antibody; APF: antiperinuclear factor; Sa: anti-Sa antibody; RA-33: anti-RA-33 antibody)
Correlations were looked for between the HLA DRB1* status and the concentrations of anti-HSC 70 and 90. We found no significant correlations between IgGs or IgMs to HSC 70 or to HSP 90 and the RA susceptibility alleles DRB1*0401 or 0402, 0403, 0404, 0405, 0408, 0101, and 0102 (table 3).
Mean anti-HSC 70 IgGs concentrations in longstanding RA patients did not differ significantly (analysis of variance) among patients with a DRB1*0401 phenotype, patients with an HLA DR4 or DR1 phenotype but without DRB1*0401, and patients who had neither the DR4 nor the DR1 phenotype (244 (121) compared with 282 (89) and 307 (174), respectively).
Patients with longstanding RA and severe joint erosions were more likely to have a positive test for anti-HSP 90 IgGs (57%) than patients with moderate (39.4%) or mild joint erosions (16%) (χ2c=7.45; p<0.05 for two degrees of freedom ; specificity: 57%; RR=3.6 (95% CI 0.8, 16.3) and OR=7.1 (95% CI 1.6, 32.0)) (table 4).
Frequency (%) of anti-HSC 70 and anti-HSP 90 by HLA DRB1* status in 68 HLA typed patients with longstanding RA and prognostic significance of increased anti-HSC 70 and anti-HSP 90 IgG and IgM
Mean anti-HSP 90 IgG concentrations did not differ significantly (analysis of variance) across the three radiographic groups (Larsen<2, 273 (88); Larsen 2–3, 281 (122); Larsen=4, 321 (140)) (fig 3).

{kind=link}
{kind=link}
{kind=link}
Concentrations of IgG antibodies to heat shock protein 90 in patients with longstanding RA by Larsen’s radiographic disease severity score.
Discussion
We found increased titres of anti-HSC 70 and anti-HSP 90 IgGs or IgMs in RA serum samples compared with serum samples from healthy controls. Anti-HSP titres were measured using ELISAs with bovine HSP proteins. Bovine constitutive and human HSC 70 are identical with the exception of one amino acid. Thus, provided the three dimensional configuration of the epitope is not dependent on this single amino acid, the antibodies found in our patients were probably autoantibodies.25 ,26
IgG and IgM isotypes were present in similar numbers of patients with longstanding RA. High titres of anti-HSC 70 and anti-HSP 90 IgGs were also seen in MCTD and SLE patients with anti-U1 RNP antibodies. This finding is in keeping with previous data17-20 obtained using ELISA or western blot techniques with bovine or murine HSPs, and limits the diagnostic usefulness of anti-HSP measurement in clinical practice.21
However, significant differences were seen in disease duration between patients with and without anti-HSP IgMs: patients with longstanding RA were more likely to have high concentrations of anti-HSC 70 and anti-HSP 90 IgMs than recent onset RA patients. Using mycobacterial HSPs, Tsoulfa et al found no differences in anti-HSP concentrations between RA patients with various disease durations.16 The late appearance of anti-HSP IgM in our longstanding RA group has no clear explanation. We can speculate that many patients with recent onset RA have a self limiting disease, so that this group differs from the longstanding RA group. Also, a substantial proportion of patients classified initially as having recent onset RA may turn out with time to have another disease.27 Lastly, anti-HSC 70 or HSP 90 IgM may be cross reacting antibodies directed against articular HSPs exposed to the patient’s immune system as a result of the chronic joint inflammation.
Our two year prospective study of recent onset RA patients detected only very few instances of seroconversion for anti-HSC 70 or anti-HSP 90. No associations were found between anti-HSP and HLA DRB1* alleles, in particular the various DR4 subtypes associated with RA. This result is clearly at variance from previously reported data on T cell responses to mycobacteria and on HSP 65 kDa in RA and non-RA patients.5 ,28 As the shared epitope QKRAA in the β chain of HLA DR class II molecules has been shown to be a ligand for the bacterial chaperone DnaK,29 we expected to find that RA patients with the DR4 allele DRB1*0401 would have an increased likelihood of anti-bacterial HSC 70 kDa positivity. Also, because protein database studies have shown that bacterial and human HSC 70 kDa are closely similar, we started our study with the hypothesis that cross reactive antibody formation would result in a higher prevalence of anti-human HSC 70 and HSP 90 in DRB1*0401positive RA patients. Our data failed to confirm this.
The only correlations found between anti-HSC 70 or HSP 90 and other diagnostic markers for adult RA30-33 linked RF and anti-Sa antibody to anti-HSP 90 IgG.
RF and anti-Sa antibody have both been shown to be associated with more severe (destructive) RA.34 ,35 The association between anti-HSP 90 IgG and RF in our study is in keeping with the prognostic significance of anti-HSP 90 and of the Larsen’s score in RA patients with longstanding RA. The prevalence of anti-HSP 90 IgG was increased in patients with severe destructive RA (57% in the Larsen > 4 group) as compared with RA patients with less destructive disease (16% in the Larsen < 2 group and 33.4% in the Larsen 2 to 4 group).
These data suggest that anti-HSP 90 IgG may be an additional marker for severe RA.33
However, they were obtained using a cross sectional design. We are currently performing a long term longitudinal study of recent onset RA patients to evaluate the prognostic significance of anti-HSP 90.
Acknowledgments
Funding: we thank the ARP (Association de Recherche sur la Polyarthrite) and the SFR (Société Française de Rhumatologie) for their financial support.