Article Text

Abstract
OBJECTIVE To confirm the impression of a better outcome of patients withdrawn from parenteral gold salt therapy compared with those withdrawn from methotrexate.
METHODS Patients with early, active, and erosive RA were randomised for a double blind trial to receive either weekly 15 mg intramuscular methotrexate or 50 mg goldsodiumthiomalate. If the drug had to be withdrawn because of side effects treatment was continued with the other drug in still active disease. Patients with insufficient response were treated with a combination of both drugs. All patients were followed up by an extended clinical and radiographic evaluation.
RESULTS 64 patients each were allocated to methotrexate and gold treatment. After 72 months a complete record was available for 88% of patients. Within the first 36 months 38 patients withdrew from gold treatment (95% because of side effects) and 23 patients withdrew from methotrexate (57% because of side effects). A significant 40% to 70% improvement of all parameters (erythrocyte sedimentation rate, C reactive protein, swollen and tender joints, radiological progression) compared with baseline was observed in patients completing their randomised treatment with gold or methotrexate. The same improvement over three years was seen in patients who withdrew from gold treatment, while patients withdrawing from methotrexate experienced a deterioration of their disease.
CONCLUSION Withdrawals represent the majority of patients in long term drug trials. Patients with early RA stopping gold because of side effects show almost the same sustained improvement as patients continuing gold or methotrexate. Patients withdrawn from methotrexate experience a reactivation of their disease.
- rheumatoid arthritis
- methotrexate
- gold
Statistics from Altmetric.com
Methotrexate (MTX) and parenteral gold salts have been shown to improve clinical and laboratory parameters of disease activity and to reduce radiological progression thereby improving the outcome of rheumatoid arthritis. Randomised clinical trials could not demonstrate any difference in efficacy between patients treated with methotrexate or with parenteral gold.1-5 MTX shows a rapid onset of action and has been shown to be efficacious also in the long term treatment.6-11 Usually, it is well tolerated, has a low drop out rate and therefore can be continued for a longer period of time than any other disease modifying anti-arthritic drug (DMARD).12-16 In comparison with methotrexate, parenteral gold treatment is complicated by higher toxicity related drop out rates.17-23
Several authors have reported a marked improvement or even longlasting remissions in patients with gold related toxicity.23 This clinical observation has never been confirmed by prospective clinical trials. For that reason we followed up over several years patients from a double blind study who discontinued a randomised treatment with parenteral gold salt (GSTM) or MTX.
Methods
PATIENTS
The study design has been outlined previously.2 It was conducted as a double blind randomised parallel group trial comparing the efficacy of MTX and GSTM in patients with definite rheumatoid arthritis according to the American College of Rheumatology criteria.24 At study entry all patients had active disease defined as the presence of three of the following criteria: (1) erythrocyte sedimentation rate (ESR) > 20 mm 1st h in men and >30 mm 1st h in women; (2) morning stiffness > 1 hour; (3) > 6 swollen joints; (4) > 9 tender joints. Additionally, patients had to have erosive disease, defined as at least a 2 mm discontinuation of cortical bone at one site.
Patients were excluded if they had advanced disease with (1) deformities (for example, subluxation, ulnar deviation) or (2) serious radiographic changes according to Larsen stage III-V in any joint25; patients were excluded if they had been treated with MTX or GSTM previously, if they had been treated with any other DMARD during the past three months, if they had had intra-articular corticosteroid injections within the previous four weeks or had conditions that preclude treatment with MTX or parenteral gold. All patients signed informed written consent to participate in the study.
TREATMENT
Patients were randomly assigned to weekly injections of 50 mg GSTM or 15 mg MTX in a double blind fashion during the first year. After unblinding at month 12 treatment was continued with the same dose in MTX treated patients while the GSTM dose was reduced to 50 mg every second week. Patients who showed no improvement or a deterioration according to the predefined criteria (see below) after 12 months continued treatment with the combination of 50 mg GSTM and 15 mg MTX/week.
In case of intolerable side effects the study medication was paused for two weeks. If toxicity remained or reappeared, the corresponding study medication was stopped permanently. Withdrawn patients who showed a remission or at least a “marked improvement” were followed up without treatment until the disease flared up again. Patients with active disease were switched to the counter study medication.
Concomitant treatment with NSAIDs and prednisone in a daily dose < 10 mg was allowed, the doses were recorded.
CLINICAL AND LABORATORY EVALUATIONS
Clinical evaluations were done at baseline and after months 1, 3, 6, 9, 12, 18, 24, 30, 36, 48, 60, and 72 by the same physician (GH). All patients who completed the trial on their original study medication and those who discontinued the randomised treatment were examined according to study design.
Safety monitoring included a physical examination and control of laboratory parameters. All side effects were recorded according to the WHO classification.26
Efficacy assessments included the number of tender and swollen joints (38 joints were counted: metacarpophalangeal (MCP) joints I-V, proximal interphalangeal (PIP) joints II-V, interphalangeal (IP) joints of the thumbs, wrists, elbows, shoulder joints, knee joints, ankle joints, metatarsophalangeal (MTP) joints II-V), C reactive protein (CRP), and ESR.
Response to treatment was defined as follows: (1) clinical remission: no swollen and < 2 tender joints; ESR < 20 mm 1st h in men, < 30 mm 1st h in women and no systemic or intra-articular corticosteroids during the past four weeks; (2) marked improvement: swollen joint count < 50% of baseline and daily dose of prednisone < 5 mg during the past four weeks; (3) improvement: swollen joint count at 51–80% of baseline and daily dose of prednisone ⩽ 7.5 mg; (4) no improvement: swollen joint count at 81–120% of baseline; (5) deterioration: swollen joint count of more than 120% of baseline values.
The response rates according to the European League Against Rheumatism (EULAR) response criteria based on the disease activity score (DAS)27 were calculated retrospectively.
Standardised radiographs of hands and forefeet were taken at baseline and after 6, 12, 24, 36, 48, 60, and 72 months. All radiographs were read by one observer (GH) blinded to patient identity and treatment but knowing the sequence of films. The radiographic destruction was measured semiquantitatively by a validated new scoring method28 in 38 joints, respectively regions (IP joints of both thumbs, the PIP joints II-V, MCP joints I-V, Os naviculare, Os lunatum, radius, ulna, IP joints of both big toes, MTP joints II-V). Grading entails a semiquantitative evaluation of the destruction of the joint surface: grade 1 = definite erosion with < 20% destruction of the joint surface, grade 2 = 21–40%, grade 3 = 41–60%, grade 4 = 61–80%, grade 5 ⩾ 80% destruction of the joint surface; total scores ranged from 0–190.
The radiological progression was calculated as the average monthly increase in the total score per patient. The pretreatment radiological progression was estimated by dividing the baseline score through the disease duration in months.
STATISTICAL ANALYSIS
Three cohorts were analysed: patients continuing randomised MTX or GSTM treatment for at least 36 months (completers) and patients discontinuing during the first 36 months (MTX withdrawals, GSTM withdrawals). MTX and GSTM completers were analysed as one group to increase statistical power of the tests, as there were no significant differences between both cohorts.2-4 Continuous variables were tested with a two tailed t test after confirming standardised distribution. Qualitative variables were tested according to χ2 statistics.
Results
The study was started as a two centre study and included 174 patients.2-4 The prospective six year follow up of all patients was only performed in one centre: 128 patients were enrolled between December 1986 and January 1990. After randomisation 64 patients each were allocated to the MTX and GSTM treatment group, respectively. Baseline demographic data showed no significant differences between the patients in both treatment groups. There were also no significant differences between the completers, the MTX and the GSTM withdrawals (table 1). After 72 months a complete record of safety and clinical efficacy data as well as radiological progression was available for 113 patients representing 88% of the randomised population. Seven patients were deceased and eight patients were lost to follow up. During the first 36 months the majority of patients randomised for GSTM (38 of 64, 59%) stopped treatment. The mean time to discontinuation was 11.3 months (range 1–31). During the same period MTX treatment was discontinued in 23 patients (36%) after a mean of 11.9 months (1–24). GSTM was discontinued significantly (p<0.05) more often because of toxicity than MTX (95% v 57%), whereas lack of efficacy was observed more often in the MTX group (43%v 5%).
Baseline patient characteristics (mean values (SD))
Twelve GSTM withdrawals continued treatment with MTX and 23 were followed up without DMARD treatment because they had reached remission or at least a predefined state of “marked improvement”. One patient died and two were lost to follow up. Eight of 10 MTX withdrawals related to a lack in efficacy were treated with the combination therapy according to the study design and two were lost to follow up. Eleven MTX withdrawals related to toxicity still had active disease with a flare up after discontinuation. All were consequently treated with GSTM but in three patients a lower dose of MTX was reintroduced in combination with GSTM because of an extended flare up, and two patients died.
The side effects in GSTM treated patients leading to discontinuation were exanthema (n=22), exanthema and stomatitis (n=7), stomatitis (n=3), alopecia (n=1), nausea (n=1), and neuropathy (n=1). Similar side effects also occurred in GSTM completers—exanthema (n=13), exanthema and stomatitis (n=5), stomatitis (n=2), and alopecia (n=1)—but did not lead to discontinuation of the drug. Also in MTX treated patients exanthema (n=5) and stomatitis (n=6) were not uncommon.
The predominant reasons for withdrawal of MTX were lack of efficacy (n=10), nausea (n=7), nausea and arthralgia (n=2), and respiratory tract infection (n=2). All drug related side effects were mild or moderate according to the WHO criteria and resolved spontaneously within the observation period. Three patients died because of pre-existing cardiovascular disease (two myocardial infarctions, one cerebral insult).
The most favourable outcome, clinical remission, according to the predefined criteria, was reached by 58% of the completers. Sixty six per cent of the GSTM withdrawals but only 26% of MTX withdrawals fulfilled the criteria of clinical remission. The mean time to clinical remission in GSTM withdrawals was 9.4 months (range 1–30), approximately two months before withdrawal. The improvement was transient in some patients but nine GSTM withdrawals (24%) were still in remission after 36 months and 12 patients (32%) showed marked improvement. In contrast with gold withdrawals the mean time to remission within the MTX withdrawals was 16.2 months (6–36)—on average 4.3 months after withdrawal (table2).
Study status at month 36 (mean values (range))
The data were confirmed by the EULAR response criteria, retrospectively. The proportions of patients with a good response (DAS < 2.4) and moderate response (DAS decrease > 1.2) are shown in figure1A and B. Completers and GSTM withdrawals show the same favourable results being superior to MTX withdrawals.

(A) Proportion of patients with good response according to the EULAR criteria in completers and withdrawals (GSTM and MTX). (B) Proportion of patients with moderate response according to the EULAR criteria in completers and withdrawals (GSTM and MTX).
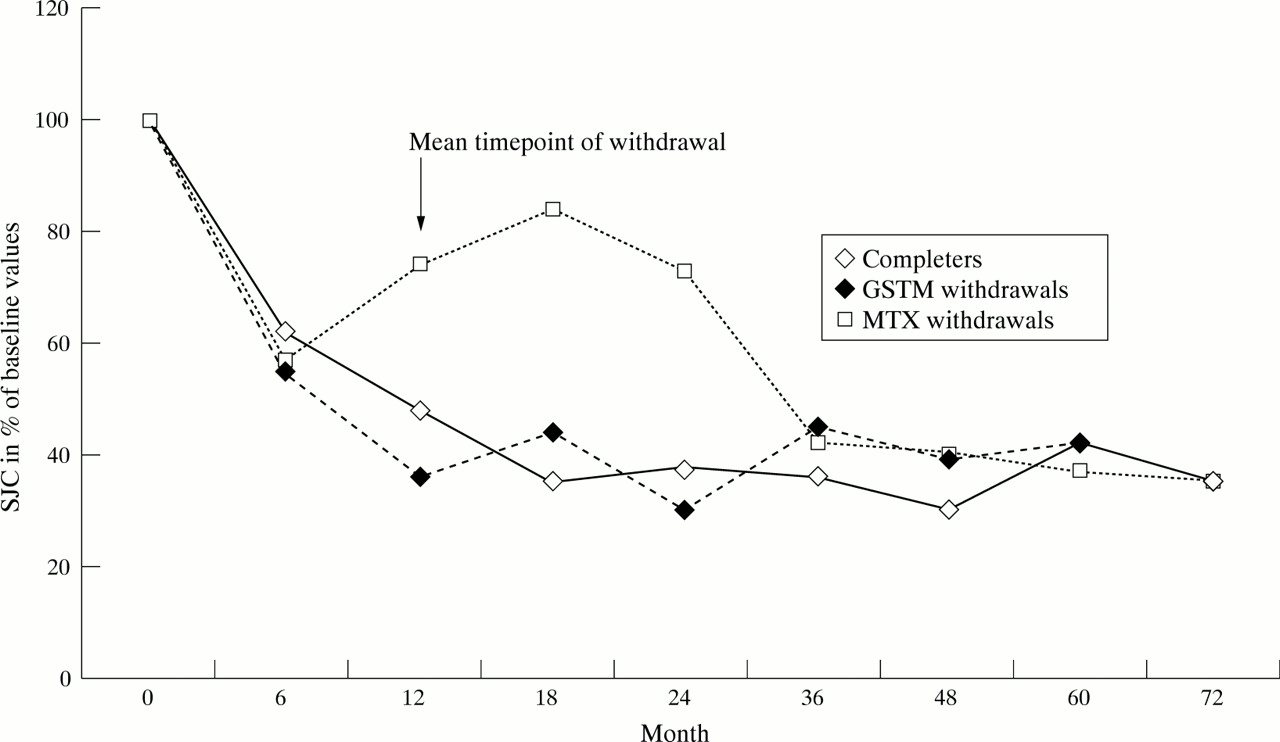
In GSTM withdrawals swollen and tender joint counts declined to an average of 30% of baseline values at month 24 (12 months after withdrawal) compared with 40% in completers. In contrast, MTX withdrawals improved only to 70% of baseline values in the swollen joint count (SJC) and 53% in the tender joint count (TJC). Later in the course of the disease the average values of the three cohorts assimilated reaching 35% for SJC and 32%–50% for TJC at month 72 (table 3, fig 2).
Outcome parameters shown as percentage of baseline

Swollen joint count in completers and withdrawals (GSTM and MTX). Response to treatment shown as percentage of baseline.
ESR and CRP were reduced to on average 50% in completers and GSTM withdrawals already after 12 months. The decline of the ESR in the MTX withdrawals was significantly smaller reaching an value of only 91% of baseline after 12 months. In addition the CRP concentrations increased to 148% of baseline after 12 months. At month 36, after treatment had been changed, MTX withdrawals showed the same improvement as completers (table 3, fig 3).
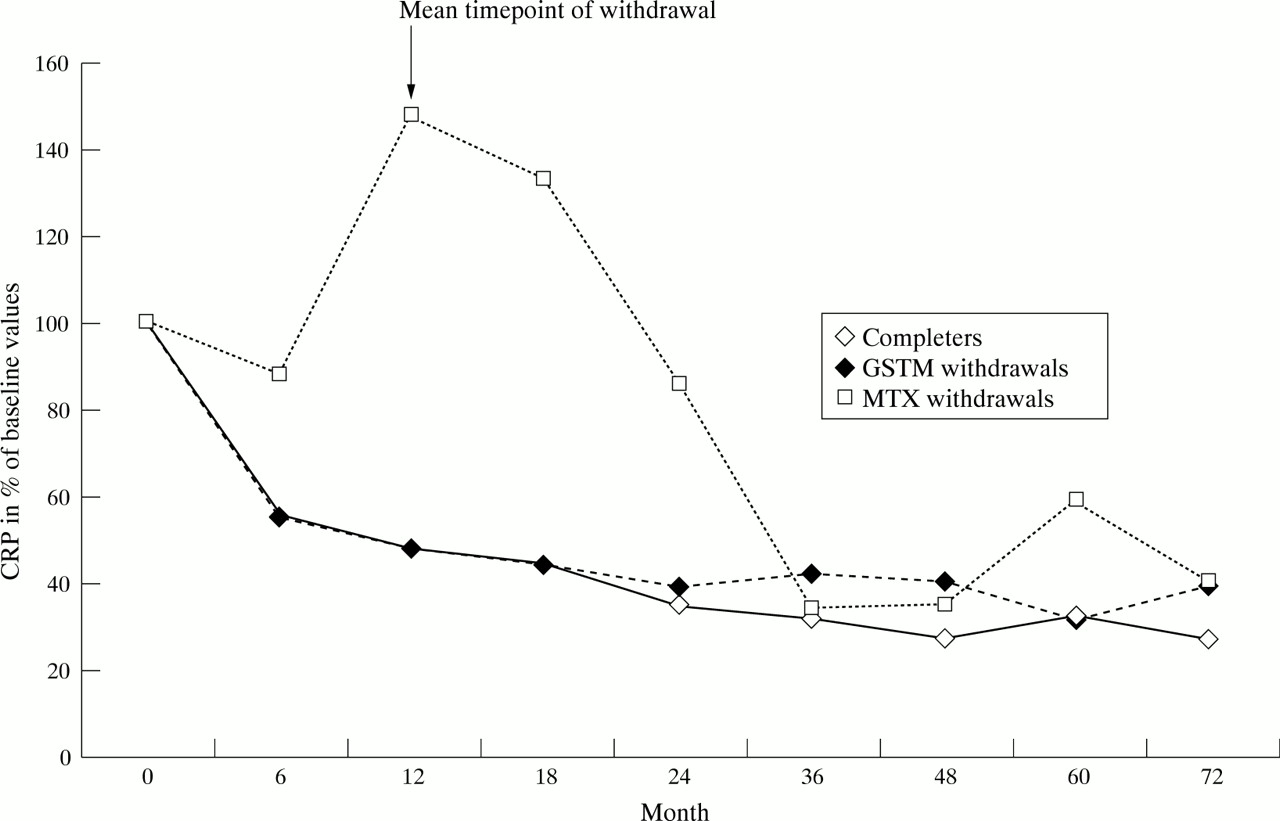
C reactive protein in completers and withdrawals (GSTM and MTX). Response to treatment shown as percentage of baseline.
The increase in the Ratingen score per month from the beginning of joint symptoms to the start of treatment was calculated to be 0.53 in the group of completers, 0.41 in GSTM withdrawals and 0.29 in MTX withdrawals. During treatment the slope of radiographic progression in the group of completers decreased to 0.30/month between month 12 and 24 with further decrease thereafter. In the group of GSTM withdrawals the progression rate decreased from 0.41 during the first six months of treatment to 0.17 during the second year of treatment, remaining low up to month 48 and gradually increasing thereafter. In contrast, MTX withdrawals showed an increase in radiographic progression from 0.69 during the first half year to 0.86 during the second half year and decreasing after the start of gold or combination treatment. Between month 48 and 60 the progression rate was the same in both cohorts withdrawn from randomised treatment while patients continuing treatment still had a low progression rate (table 4, fig 4).
Radiological progression (increase in Ratingen score per month, mean values, (standard deviation))

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Slope of radiological deterioration in completers and withdrawals (GSTM and MTX). Average increase in Ratingen score per month.
In the GSTM withdrawal cohort 14 of 38 patients (37%) showed no radiographic progression from the beginning of treatment, compared with 21 of 67 (31%) in the group of completers and 6 of 23 (26%) in the group of MTX withdrawals.
Discussion
Parenteral gold salts29-38 and MTX6-11 ,39 ,40 modify the course of rheumatoid arthritis when given in sufficient doses over a longer period of time. Although the mode of action may be different both drugs extend a similar efficacy in patients with early erosive rheumatoid arthritis.2-4 ,15 In several trials and meta-analyses drug survival for MTX has been shown to be significantly longer than that for gold treatment because of a higher toxicity related withdrawal rate in gold treated patients3 ,14 ,41 with more than 50% of patients dropping out within 36 months. Withdrawals are often described as treatment failures, their outcome is usually not reported in the publication of clinical trials, and these patients are not followed up prospectively for a longer period of time. The only prospective trial performed by the Empire Rheumatism Council42 ,43 failed to demonstrate an additional beneficial effect in patients suffering from gold induced toxicity.
This is the first prospective six year follow up of patients withdrawn from a randomised DMARD trial.
Our data are based on a follow up rate of 88% after 72 months and therefore represent the vast majority of patients recruited for a DMARD trial in early erosive rheumatoid arthritis. Patients withdrawn from the randomised treatment were treated in a standardised fashion and followed up the same way as patients continuing treatment.
Relevant and significant differences could be demonstrated in the clinical and radiological course of patients withdrawn from GSTM and MTX treatment.
MTX improves the course of rheumatoid arthritis only when the treatment is continued in a sufficient dose. MTX treated patients who were later withdrawn showed only a transient improvement after the start of MTX treatment lasting a mean of three months and worsened thereafter. These patients showed a sustained improvement only after starting GSTM as monotherapy or in combination with MTX.
A worsening (relapse) after discontinuation of MTX is a common clinical experience and has been confirmed in numerous trials.11 ,44 Even the four week discontinuation of “insufficient” MTX treatment before starting treatment with novel drugs resulted in a flare up in the majority of patients.45 A trial on elective drug discontinuation in patients being in remission showed a significant deterioration in patients receiving placebo when compared with patients continuing their DMARD treatment.46
In our study, patients withdrawn from gold treatment demonstrated an improvement of 40% to 70% in all clinical parameters similar to patients who continued their randomised treatment. (The good clinical condition of the patients at the time of their discontinuation may reflect the tendency of patients doing well to discontinue treatment for minor side effects.) This improvement was sustained for an average of 24 months after discontinuation of the drug even in patients without further DMARD treatment. Twenty four months is also the duration of gold induced remissions reported by others.23 ,47
Completers and withdrawals had a comparable disease activity at baseline and after six years. The reversibility of the improvement in the GSTM withdrawals and the transient deterioration in MTX treated patients after withdrawal, improving again after introduction of gold treatment, indicates a treatment effect and cannot be explained by a selection of patients with milder or more severe disease.
As the beneficial effect in GSTM withdrawals seems to be limited in duration in many patients, a remission keeping strategy seems to be necessary. After a temporary discontinuation of treatment a further course of gold could be started as soon as the side effects have disappeared48 or treatment could be continued with a very low dose despite the existence of side effects.49 Ten Wolde et al described a better 12 month outcome in patients continuing DMARD treatment in remission compared with patients stopping and reintroducing after a flare up50 confirming the preference for continued treatment.
The clinical observation of a marked improvement or even longlasting remission in patients with gold related toxicity has been confirmed by this prospective six year trial.
In addition, our data support the need for a modification of trial designs: as withdrawals represent the majority of patients in long term drug trials they should not be excluded from efficacy analysis. (Clinically relevant differences between MTX and GSTM treatment are more likely to be detected in withdrawals than in completers). Patients stopping treatment because of relatively mild side effects, being in remission or marked improvement should not be regarded as treatment failures.
Acknowledgments
We thank Ms Gudrun Krüger for her secreterial work.
References
Footnotes
Funding: the trial was sponsored in part by a research grant from Lederle Laboratories.