Article Text

Abstract
OBJECTIVE To assess the prevalence of primary hip osteoarthritis (OA) in Iceland. To compare the prevalence of primary hip OA in Iceland with published rates of primary hip OA for related Scandinavian populations.
METHODS Roentgenographs were examined of 1530 Icelandic people 35 years or older (653 males, 877 females) subjected to colon radiography during the years 1990–1996. The radiographs examined represent approximately 40% of all colon radiographs taken in Iceland during this period. After exclusion of non-primary hip OA cases, the minimum hip joint space was measured with a mm ruler. Presence of hip OA was defined as a minimum joint space of 2.5 mm or less on an anteroposterior radiograph. Intraclass correlation coefficients for inter and intraobserver variability of assessment of mm joint space were 0.91 and 0.95, respectively.
RESULTS Of the 1517 people included, 227 hips in 165 patients (77 men, 88 women) were diagnosed as having radiological primary hip OA. The mean age at colon examination for these patients was 68 (35–89) years. The overall prevalence of coxarthrosis among all examined patients 35 years and older was 10.8% (12% for men, 10% for women), rising from 2% at 35–39 years to 35.4% for those 85 years or older. If the population structure (age and sex distribution) for those older than 35 years in Iceland was used to standardise prevalence for both Iceland and south Sweden (using previously published data for south Sweden), the age and sex standardised prevalence of hip OA for those older than 35 years in Iceland was 8%, compared with 1.2% for south Sweden.
CONCLUSIONS The prevalence of radiological primary hip OA is very high in Iceland, and in excess of fivefold higher than the prevalence found by using similar techniques in studies on related populations in southern Scandinavia. The rate difference is particularly notable for those younger than 70 years.
- hip
- osteoarthritis
- Iceland
Statistics from Altmetric.com
Epidemiological surveys of hip osteoarthritis (OA) yield varying age related prevalence rates.1-12 A comprehensive review of hip OA prevalence in different populations has been undertaken by Felson.13 Reasons for the apparent variations in prevalence may be associated with the variable definitions used for hip OA in the different studies, whether based on symptoms, clinical examination and history, radiographic signs, differences in population structure, or a combination of these.11 ,14-20 The use of varying criteria for the definition of hip OA makes the comparison of age corrected prevalence rates of hip OA between different populations very difficult. Additional reasons for the variable prevalence rates noted in these surveys undoubtedly exist, such as hereditary factors,21-27 but their contribution to population related differences in rates of hip OA are difficult to define, for reasons given.
Settlement in Iceland begun in ad 870 and was considered completed in the year of 930, at which time there were some 10–20 000 inhabitants on the island. The names and land claims of the 435 Norwegian Viking chiefs listed as Icelandic settlers in this period are known. The chiefs brought slaves into the country, mostly from Ireland, during the same period. The Icelandic population experienced several catastrophic decimations caused by disease such as bubonic plague in the years 1400–1600, and famine in connection with volcanic eruptions in the 18th century. For example, some 30% of the Icelandic population perished in connection with eruptions at Hekla and other volcanoes around the year 1783. Immigration has remained low since the time of colonisation. Until recently, much of the population lived in small isolated fishing and farming communities along the coast line. Written and oral records maintain a detailed family history for the Icelandic population since the time of colonisation more than a thousand years ago. The Icelandic population, currently a total of some 275 000, thus fulfils several conditions for an enrichment, and identification, of inherited diseases.
We have previously identified a large Icelandic family with a very high prevalence of hip OA, suggesting the presence of a hereditary risk factor.28 ,29
Recent data suggest that the incidence of surgery for primary hip OA is high in Iceland. Thus, for the period of 1990–1996, the mean age related annual incidence of hip replacements/100 000 inhabitants (men and women) was 84 for the age group 50–59 years, 308 (ages 60–69), 478 (ages 70–79), 409 (ages 80–89) and 125 (ages 90 and older), respectively (Ingvarsson, Hägglund and Lohmander, unpublished data). When calculated for ages 50 and older, the Icelandic mean annual rate was 306/100 000. The age related rate for those 50 and older with the same diagnosis in southern Sweden in 1982 was 150/100 000.30 The Icelandic rates of hip replacement for primary OA also appear to be higher than for white populations in San Francisco in 1984–1988.22
Based on these indications that suggest that the prevalence of hip OA in Iceland may be high in comparison with other populations, we have assessed the prevalence of radiographic hip OA in Iceland by examining the roentgenographs of 1530 people 35 years or older subjected to colon radiography during the years 1990–1996.
Methods
POPULATION EXAMINED
All colon radiographs (double contrast, barium enema) taken at three different radiographic departments in Iceland during the years 1990–1996 were examined. In total, radiographs from 1530 patients (653 men, 877 women) were analysed. The patients were referred for radiography at these radiographic departments from four different hospitals (community and academic), as well as from the primary health care system. Patients were from both rural and urban areas. National radiology data show that approximately 3800 colon radiographs were performed in the country during 1990–1996, and the radiographs examined in this study thus represent approximately 40% of all colon radiographs taken in Iceland during this seven year period. Only radiographs from patients 35 years of age or older at the time of the colon examination were used. All patients were Icelanders. Population statistics for Iceland and Sweden were obtained from Statistics Iceland and Statistics Sweden, respectively.
RADIOGRAPHIC TECHNIQUES
The double contrast (barium enema) colon radiographs included at least two anteroposterior (AP) and several oblique exposures of the hip joint. The hip joints were assessed from an AP control colon radiograph, which is taken with the same tube to film distance of 100 cm that is used in a standard AP view of the pelvis. The measurements of hip joint space were done on the AP film. To be included in this investigation both hips had to be clearly visualised on an AP film. The oblique exposures were used to assess osteophytes, sclerosis, cysts and any signs of secondary OA.
The age of the patient at the time of colon examination, and signs of secondary OA and hip operations were registered. Hips with signs of secondary OA (congenital dislocation or dysplasia, Perthes’ disease, slipped epiphysis) were registered, but excluded from further analysis. The localisation of radiographic changes was classified as lateral, medial or mixed.31 Clinical information was sought in hospital records for patients who had been operated on with total hip replacement, and their primary diagnosis was established. The minimal hip joint space was measured on the AP film with a ruler divided in millimetres.11 All radiographs were analysed by one of the authors (TI). All hips with a hip replacement because of primary OA were recorded as a hip with a joint space of 0 mm. A minimum hip joint space of 2.5 mm or less was used as a criterion for an OA hip, as recently suggested.11 ,20
STATISTICAL METHODS
Non-parametric statistical methods were used for group comparisons. Observer reliability for radiographic hip joint space measurements in mm was assessed by measuring 294 randomly selected hips twice by the same observer, and 174 randomly selected hips by two independent observers (TI and GH). Data reported in this study are for joint space measurements by a single observer (TI). Intra-class correlation coefficients for inter-observer variability of assessment of mm joint space were 0.906 (0.871, 0.931, 95% confidence intervals, left hip), and 0.920 (0.888, 0.9440, right hip), respectively. The corresponding intra-rater figures were 0.954 (0.930, 0.970) and 0.942 (0.914, 0.962), respectively. Full inter-rater agreement for joint space was found for 127 of 174 hips, 0.5 mm difference for 43 of 174 and 1 mm difference for 4 of 174 hips measured. Exact intra-rater agreement for joint space measurement was found for 233 of 294 hips, 0.5 mm difference for 29 of 294, 1 mm difference for 30 of 294, and 1.5 and 2 mm difference for one hip each.
Results
Of the 1530 people examined, eight were excluded because both hips were not clearly visualised and five patients because of signs of secondary OA: (three with Perthes’ disease, one with congenital hip dysplasia, and one with rheumatoid arthritis). Thus, 1517 patients (644 men, 873 women) remained for analysis. The mean age at examination was 61 years for the men and 58 years for the women (table 1).
Age related prevalence of hip OA in Iceland
The mean minimal hip joint space was 3.9 mm (range 0–7) for the 1517 patients (fig 1). Overall, the mean minimal joint space decreased from 4.0 mm for those aged 35–39 years to 3.7 mm for those aged 80 years or more (fig 2). The mean joint space was 0.3 mm less for women than for men in all age groups (fig 2). There were no significant differences in joint space between left and right hips at any age for either men or women (data not shown). Using the recommended minimum joint space of 2.5 mm or less as a cut off for the presence of radiological hip OA,11 227 hips in 165 patients (77 men, 88 women ) were diagnosed as having hip OA (table 1 and fig 1). The mean age at colon examination for these patients was 68 (35–89) years. The overall prevalence of hip OA among all patients 35 years and older was 10.8%, rising from 2% at 35–39 years to 26.3% for those 85 years or older (fig 3). The hip OA was classified as medial in 11%, lateral in 34% and mixed in 55%. Sixty two cases had bilateral hip OA, 61 cases had right hip OA and 42 had left hip OA table 2).

Histogram of hip joint space distribution measured on 1517 colon radiographs from Iceland. The vertical axis denotes the proportion of hips. The size class of 0.0 mm includes 49 hips with arthroplasty resulting from primary hip OA. The number of hips for each size class is 0 mm (81), 0.5 mm (1), 1.0 mm (22), 1.5 mm (14), 2.0 mm (53), 2.5 mm (60), 3.0 mm (471), 3.5 mm (278), 4.0 mm (1383), 4.5 mm (145), 5.0 mm (500), 5.5 mm (3), 6.0 mm (19), 6.5 mm (0), 7.0 mm (4). The vertical line indicates the joint space cut off for hip OA.
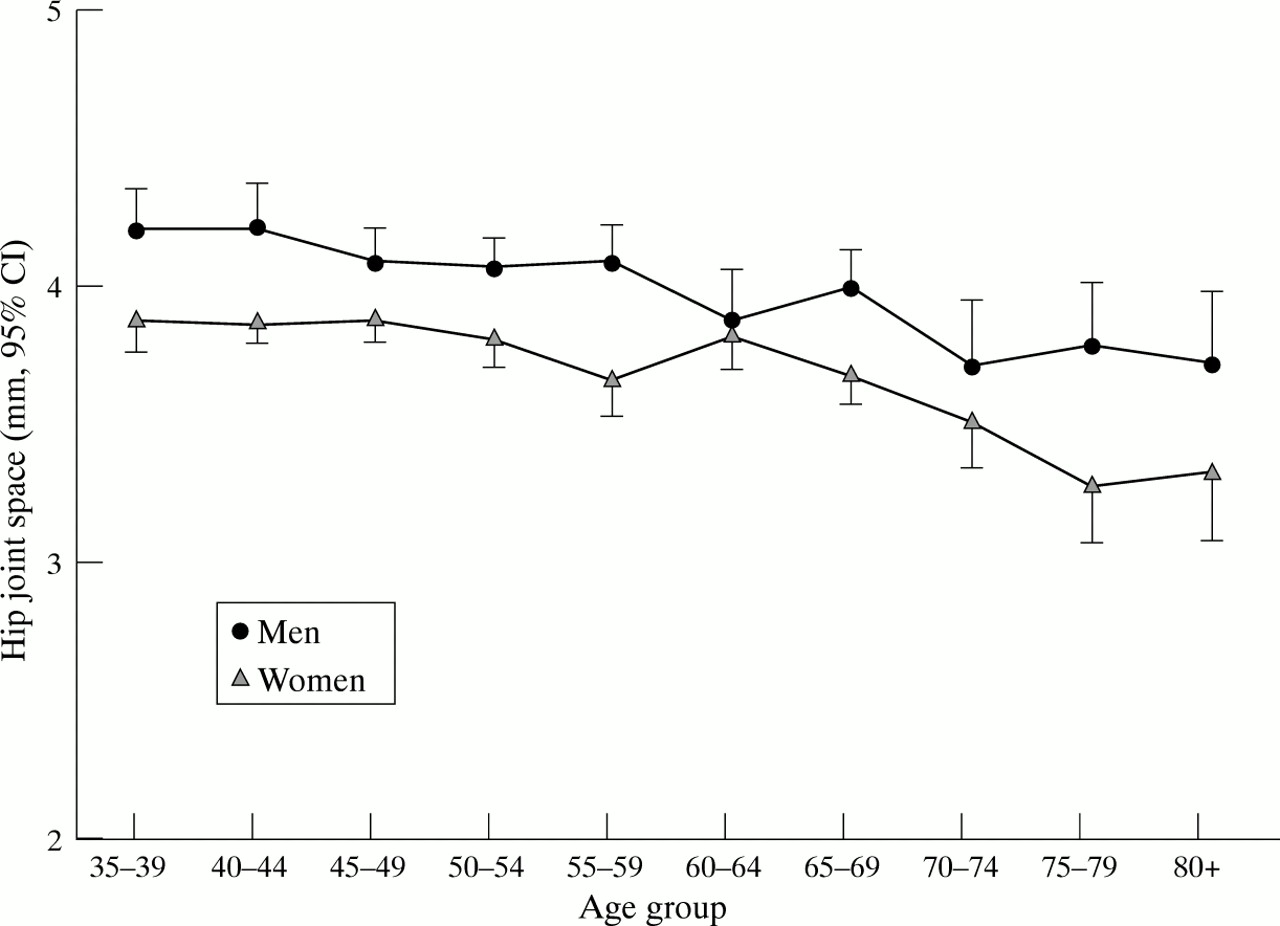
Hip joint space (mm) by age groups for men and women. Bars denote 95% confidence intervals.

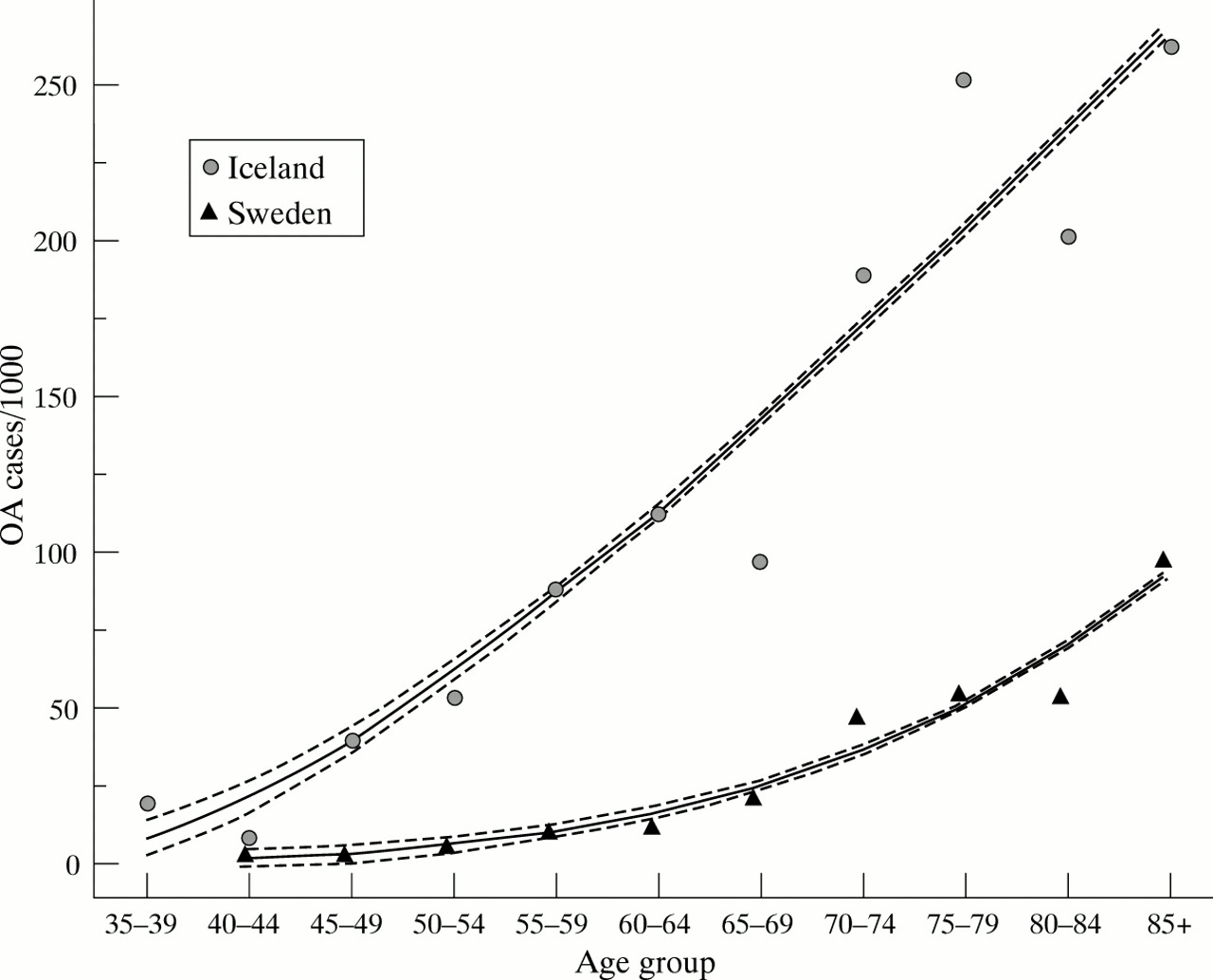
Hip OA prevalence in relation to age in Iceland and Malmö, Sweden, assessed from colon radiographs. Data points represent observed values, lines represent predicted curve fits with r2 greater than 0.9, broken lines represent 95% confidence intervals for predicted curves. Data for Malmö, Sweden from Felson.12
Unilateral and bilateral hip OA in Iceland
The overall OA prevalence rate of 10.8% within the study group aged 35 years and older calculated here does not take into consideration any differences between the age and sex distribution of the studied cohort and the population from which it was drawn. If we use the population statistics (age and sex distribution) for the country of Iceland in the relevant time period to standardise the Icelandic OA prevalence, we derive an age and sex standardised population prevalence rate of hip OA for those 35 years and older in Iceland of 8% (table 3). It should be noted that such standardisations based on actual population structure have not previously been done in published studies on hip OA prevalence. Therefore, any comparisons with published data have to be based on uncorrected rates, unless information is available on the population structure in the studied region for the relevant time, see discussion below.
Age standardised prevalence of hip OA in Iceland
Forty of the 165 patients with hip OA (20 men and 20 women) had been operated on with hip arthroplasty (31 unilaterally, 9 bilaterally) because of primary hip OA (table 1). The mean age of these patients was 72 (45–89) years. A further 13 cases were operated on because of hip fracture, 10 with osteosynthesis and three with arthroplasty (table1).
Discussion
RADIOLOGICAL DEFINITION OF HIP OA FOR EPIDEMIOLOGICAL STUDIES
Previous epidemiological studies on hip OA have used varying criteria for case definition, based on symptoms, radiological findings, or a combination of both.2 ,7 ,11 ,14-20 Even reports using only radiological criteria have rarely agreed on case definition, making it difficult to assess differences among studies of different populations, or to understand the contribution of different risk factors to those variations. Several studies have used (or discussed) minimum joint space width as the single variable for definition of hip OA, with a cut off for case definition varying between 1.5 and 4 mm.1 ,4 ,5 ,9 ,10 ,12 ,20 ,32 ,33 Some investigators have arbitrarily defined hip joint space narrowing (hip OA) as a joint space less than 4 mm in persons aged 70 years or less, or less than 3 mm in persons older than 70 years.1 ,5 ,10 ,12 In addition, a side to side difference of more than 1 mm was classified as hip OA by these investigators. Other Scandinavian investigators have used cut off values, independent of age, of 2 mm or less,9 or 3 mm or less.4
The distribution of hip joint space width is continuous, and it was noted that a more stringent case definition of 1.5 mm minimum joint space was more closely associated with risk factors than a less stringent one. On the other hand, the cut off of 1.5 mm minimum hip joint space had the disadvantage in that it would identify only the more severe and late stage subsets of the disease.20 It was stated that the measurement of the minimal joint space with a ruler is a simple, reproducible way to estimate prevalence of OA of the hip and well suited for epidemiological studies.11
METHODOLOGY AND RELIABILITY OF COLON RADIOGRAPHY FOR HIP ASSESSMENT
The colon examinations used in this investigation represent approximately 40% of those performed in the country of Iceland during 1990–1996. Subjects were recruited from both rural and urban areas, and from both academic centres and primary care. There was no difference in the prevalence of hip OA between the three different radiological departments studied (data not shown). Age and sex data for some 3000 (out of a total of 3800) of the people examined by colon radiographs in this time period was available, and the age and sex distribution for these people was similar to that of the 1517 people examined in this study. We thus suggest that the subjects studied here may be regarded as representative for the Icelandic population “at risk” in this time period.
Radiography of the colon could underestimate minor structural changes compared with radiographs that are optimally exposed for the hip joint. Earlier studies have, however, found a good agreement between colon and hip joint radiographs both in regard to prevalence and degree of hip OA.1 ,10
Hip radiographs used in OA epidemiology studies have regularly been non-weight bearing (whether using hip or colon radiographs), although a recent investigation suggested that weight bearing radiographs might be preferable in examination of OA hips.34
One report has suggested that patients who had undergone total hip replacement because of primary coxarthrosis had a higher frequency of colon examinations (1.3-fold) than age and sex matched controls from the same population.35 This could suggest that examination of colon radiographs might lead to an overestimation of the prevalence of hip OA in the general population. Recent studies further suggest that obesity is linked to colon cancer and adenoma.36Assuming that these subjects more frequently undergo colon radiographs, obese subjects could be over-represented in the group studied here. However, the linkage between obesity and hip OA is uncertain.13 In any case, similar methods (assessment of minimum hip joint space on AP colon radiographs) were used in the present work and in the studies in Sweden and Denmark, which form the main basis for our comparisons with Icelandic hip OA prevalence.1 ,4 ,5 ,9 ,10 ,12 ,32
Only one case of inflammatory hip arthritis was identified when examining these radiographs. If the prevalence of rheumatoid arthritis in Iceland is assumed to be similar to that in Sweden, or about 1%, some 15 cases would be expected to be present in the study population. However, it is uncertain how many of these would have had radiological signs of rheumatoid arthritis in the hip. The possibility of including a few cases of inflammatory hip arthritis would be similar in all studies of this type, and would not be expected to influence the relative differences in prevalence of hip OA reported here.
The intra-rater reliability of our measurement of hip joint space was high, in concordance with earlier investigations, which have shown that measurement of joint space has a higher reproducibility than other indices for hip OA.11 The joint space width is strongly correlated with other radiological and clinical features of osteoarthrosis of the hip.11
We defined radiological hip OA as a joint space of 2.5 mm or less (fig1), in agreement with previous suggestions.11 ,20 The mean joint space in the present material decreased slightly with age (fig2), and was 0.3 mm less in women than in men in all age groups (fig 2). In contrast, a previous study37 found a slight increase in joint space with age, and no difference in joint space between men and women. The latter study, however, excluded any hips with signs of OA. Here, we chose to use the same joint space width cut off for all age groups and both sexes.
In this investigation, replaced hips were assigned a joint space width of 0 mm. Had these hips been excluded from calculations, the mean minimum joint space in this material would have increased by 0.07 mm. Exclusion of replaced hips from the different age classes would, however, remove the hips with the least joint space from calculations, and the rate of joint replacements would then directly influence the estimated average minimum joint space in the population. In support of the assignment of a value of 0 mm for replaced hips, we found that the minimum joint space measured on radiographs taken shortly before joint surgery was 0 mm in 29 of 34 hips in this material (range 0–1 mm). Pre-operative radiographs were available for 34 of 49 hips.
PREVALENCE OF HIP OA IN ICELAND COMPARED WITH SOUTHERN SCANDINAVIA
The overall prevalence of hip OA in this group of Icelandic people examined by colon radiography was, for the ages 35 and older, 12% for men and 10% for women. In 62 of the 165 cases (38%) the OA was bilateral, comparing well with the previously shown bilateral proportion of 35% in Sweden.5 The distribution of cases of hip OA characterised as medial, lateral and mixed was comparable with previous reports.31
The colon examinations used here were undertaken during the years 1990–1996, in which period the population of Iceland was about 250 000. The population examined is comparable in size to the population of Malmö city, Sweden, that has provided the basis for a series of studies on hip OA prevalence, using a technique similar to that used in the present investigation.12
The overall prevalence of hip OA in the city of Malmö, southern Sweden, was thus estimated to be about 2.3% among those over 40 years of age and examined by colon radiographs1 (table 4). Later examinations of the same population in southern Sweden have yielded similar results.5 ,32 A recent review, based on the examination of a total of 12 000 colon radiographs, reported a prevalence of hip OA in Malmö for the period of 1956–1995 of 2.1% for those aged 40 years and older examined by colon radiography.12 The prevalence did not change during this 40 year time period. A study of hip OA prevalence on the Baltic island of Gotland, again using similar methods, yielded a prevalence rate for hip OA of 4.5% for those 45 years and older.9 In comparison, the prevalence of hip OA in Denmark was found to be 4.7% in the age group older than 40 years,4 using the hip OA criterion of 3 mm or less of minimum joint space measured on colon radiographs (table 4).
Prevalence of hip OA in Iceland compared with reported prevalence data for Sweden and Denmark (given as cases/1000)
The overall prevalence rates discussed here and published from southern Scandinavia, have not been corrected for the differences in distribution of age or sex between the groups studied and the populations from which these groups were drawn. Moreover, if we are to make relevant comparisons between different populations, such differences between populations must be accounted for. If we thus use the population statistics (age and sex distribution) for Iceland in the relevant time period to standardise both the Icelandic and the Swedish prevalence, we derive an age and sex standardised prevalence rate of hip OA for those older than 35 years in Iceland of 8%, compared with a similarly age and sex standardised (using Icelandic population structure) rate in Malmö, Sweden of 1.2%, a more than fivefold difference. This illustrates the importance of detailed age and sex related prevalence data, as well as the importance of taking differences in population structure into consideration when comparing prevalence rates between different countries.
The definitions for hip OA used in the studies of the related Scandinavian populations in both southern Sweden and Denmark were less stringent than those used in this study of the Icelandic population (see above). Had we used identical criteria to those used for southern Sweden (or Denmark), the estimated overall prevalence of hip OA in Iceland would be considerably higher, 25.7% (23%) instead of 10.8% for those 35 years and older. Had we, similar to the Malmö investigations, included those cases where there was a difference of 1 mm in joint space between the two hips, the number of cases in our material classified as having hip OA would have increased from 165 to 300 (or from 227 hips to 362 hips, data not shown).
In England, the prevalence of hip OA has been estimated on the basis of examination of intravenous urograms.11 With a hip OA criterion of a joint space of 2.5 mm or less, the proportion of hips in men aged 60–75 having OA was 14.4%. With a cut off of 1.5 mm, the hip OA prevalence was 2.0% for this age group. Using the same criteria for the Icelandic population, the corresponding Icelandic prevalence rates for this age class would have been 14% and 4.5%, respectively. Further investigation and proper use of population statistics will be needed to confirm whether the English and Icelandic rates are similarly high or not, in comparison with southern Scandinavia.
A recent study on radiographic hip OA in Pima Indians provided prevalence estimates for males between 3.7%–7.3% for the age groups between 45 and 74 years, and between 2.5%–3.5 % for the same ages in women.38 These estimates, based on scoring by radiographic atlas, were not significantly different from that of the US population.38
THE PREVALENCE OF RADIOLOGICAL PRIMARY HIP OA IS HIGH IN ICELAND
We conclude from these results that the prevalence of primary hip OA is very high in Iceland, compared with the related Scandinavian populations in southern Sweden and Denmark. Furthermore, it seems that the hip OA disease process begins at a younger age in Iceland than in some other studied populations (table 4). For example, the ratios between the predicted prevalence rates in Iceland and Malmö, respectively, varied between 5.1 and 7.4 for the ages 40–69 years, while the corresponding ratios for those 70 and older varied between 4.7 and 2.8 (fig 4). The existence of a high prevalence of primary hip OA in Iceland is consistent with the apparent high incidence of hip arthroplasty for primary OA in Iceland, compared with Sweden and San Francisco, as noted above22 ,30 and Ingvarssonet al (unpublished data).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Predicted age related ratios of prevalence of hip OA between Iceland and Malmö, Sweden. The prevalence data used for calculation of age related ratios are the values predicted from the curve fits in figure 3. A cubic spline fit was made to the predicted ratio values.
The risk factors associated with primary hip OA are not well defined.13 Some investigations have associated an increased risk of hip OA with heavy labour such as farm work,39-41 and with sports.10 It is notable that the higher rate of hip OA observed for the Swedish island of Gotland, as compared with that for Malmö city, Sweden, was entirely attributable to a higher prevalence among the rural, farming, population on the island9 (table 3). A higher risk for primary hip OA associated with farming was, however, only seen for men, not for women.42 In this study, we found a greatly increased prevalence of primary hip OA in both Icelandic men and women. This would perhaps suggest that physical work load is not the main reason for the high Icelandic prevalence, unless there was, in the relevant time period, a significant difference in this risk factor between rural women in Iceland and southern Scandinavia, which seems unlikely as only some 4% of the Icelandic population are farmers (Statistics Iceland). It should also be noted that the population studied in this report was both rural and urban. The observation that the “excess” of cases in Iceland was greater at younger than older age, would perhaps also speak against a heavier physical work load being a major causative factor.
Hereditary factors are suggested to contribute to primary OA,21-27 but their relative contribution to population related differences in rates of hip OA is not well defined. We have previously reported a family in Iceland with a very high frequency of hip OA.28 ,29 Separate Icelandic families with spondyloepiphyseal dysplasia43 and with knee OA44 resulting from possible genetic defects have been described. In the apparent absence of obvious differences in other risk factors between the populations compared here, it may be of interest to screen the Icelandic population for hereditary factors that could be associated with the development of hip OA at a young age.
Acknowledgments
We thank the staff at the Radiological Department at Central Hospital of Akureyri, Iceland for their assistance.
References
Footnotes
Funding: this study was supported by The Swedish Medical Research Council, Lund Medical Faculty and University Hospital, the King Gustaf V 80-year Fund, and the Zoega and Kock Foundations.