Article Text

Abstract
OBJECTIVE To determine the efficacy of corticosteroid irrigation of the parotid gland in relieving salivary flow deficiency in patients with Sjögren’s syndrome.
METHODS The parotid glands of 31 patients with primary (24) or secondary (seven) Sjögren’s syndrome were irrigated either with saline solution followed by corticosteroid solution, or with saline solution alone. Salivary function was assessed by Saxon test.
RESULTS Corticosteroid irrigation significantly increased the salivary flow rate in patients with Sjögren’s syndrome (p< 0.0001), with clinical improvement detectable 3.7 (2.4) weeks (mean (SD)) after initial corticosteroid irrigation. The extent of improvement in salivary function was reciprocal to the clinical severity of the disease, with patients at the early stages obtaining 1.20 (0.57) g net increase in salivary flow rate, and patients at the most advanced stages obtaining 0.20 (0.47) g net increase. Repeated corticosteroid irrigations did not evoke corticosteroid refractoriness of the salivary gland; similar levels of net increase in salivary flow rate were observed after the second to fourth challenge of the corticosteroid in these patients. The sustained period was 8.4 (3.5) months (mean (SD)).
CONCLUSION These findings suggest the clinical usefulness of corticosteroid irrigation therapy in relieving xerostomia in patients with Sjögren’s syndrome.
- Sjögren’s syndrome
- xerostomia
- corticosteroids
Statistics from Altmetric.com
Sjögren’s syndrome is characterised by dry eyes (keratoconjunctivitis sicca) and dry mouth (xerostomia). Xerostomia is thought to be irreversible, and may lead to decreased quality of life. Patients complain of a continued oral dryness and have difficulty in swallowing dry foods, chewing, and speaking. These patients are susceptible to increased caries, a burning sensation of the tongue, and oral infection.
Several approaches have been attempted to relieve these symptoms.1-5 The efficacy of such treatments may depend on the level of severity of the symptoms; the management of xerostomia should differ between patients whose salivary flow can be increased by means of appropriate stimuli and those whose salivary flow is refratory to such stimuli.
We report the results of a clinical trial of corticosteroid irrigation of the parotid glands in patients with Sjögren’s syndrome. The long term (up to 28 months) follow up study was performed to evaluate the corticosteroid irrigation treatment. The results clearly showed that corticosteroid irrigation was as equally effective as previous methods of treatment for xerostomia, the effect was sustained for longer periods, and no corticosteroid refractory was observed.
Methods
PATIENTS
Thirty one female patients (age range; 29–71 years) with Sjögren’s syndrome took part in this study. The diagnosis of Sjögren’s syndrome was made on the basis of criteria proposed by Fox.6 Of these patients, 24 were primary Sjögren’s syndrome patients, and seven were secondary Sjögren’s syndrome patients associated with rheumatoid arthritis (five) or systemic lupus erythematosus (two). All patients presented with varying degrees of xerostomia associated with decreased salivary flow rate, as evidenced by Saxon test (less than 3 g/2 min). Informed consent was obtained from each patient before starting the corticosteroid treatment.
CORTICOSTEROID IRRIGATION
Prednisolone sodium succinate was used for the parotid gland irrigation. The agent was dissolved in saline solution at a concentration of 2 mg/ml. The treatment procedure included irrigation of the parotid gland duct system with the saline solution (1 ml) followed by irrigation with the corticosteroid solution (1 ml). The irrigation was performed in both parotid glands of each patient via a catheter adjusted for sialography (SIA-2, Cathex, Tokyo, Japan) (fig1). The catheter had a 1 mm calibre and its tip was tapered for easy insertion into the Stensen’s duct. Before insertion, the catheter was filled with the saline or corticosteroid solution, as patients with Sjögren’s syndrome cannot fill up the catheter with their own saliva. The solutions were retained in the parotid glands for two minutes, the catheter removed, and then the solutions were allowed to run out from the ducts. Figure 2 summarises the corticosteroid irrigation procedure. Irrigation with saline solution was carried out at every two weeks. This continued for at least two months. Saline irrigation was followed by irrigation with corticosteroid solution. This continued for three weeks, and the irrigation was performed four times at intervals of one week. The corticosteroid solution (1 ml) was injected into, and retained for two minutes in each of the parotid glands. To avoid a backflow of the corticosteroid solution, the catheter remained inserted in the ducts. A Saxon test was carried out just before every irrigation with the saline or corticosteroid to evaluate the pretreatment level of salivary flow rates of the patients and the efficacy of the treatment.

A catheter used for the saline or corticosteroid irrigation of the parotid gland. It was connected to a 5 ml cylinder and filled with saline or corticosteroid solution. For corticosteroid irrigation, the catheter was inserted 1 to 2 cm into the Stensen’s duct, and was held in the duct for two minutes.

A schematic chart showing the procedure for corticosteroid irrigation in a patient with Sjögren’s syndrome. The treatment started with irrigation using saline solution, which continued for two to three months, depending on the presence or absence of inflammatory symptoms of the parotid glands. This was followed by corticosteroid irrigation for three weeks and then by the follow up period. A Saxon test was performed at the time of irrigations and also periodically (every two weeks) during the follow up period (arrow heads). The results (salivary flow rates) are expressed as g/2 min. A schematic drawing of the results of the Saxon test is shown below. (A) A time point when the improvement in the salivary flow rate was confirmed; (B) a time point when the loss of the treatment effect was confirmed.
After the completion of the series of corticosteroid irrigations, we determined that improvement was evident when the salivary flow rate increased at consecutive two time points during the follow up period (fig 2). Conversely, when the salivary flow rate decreased on consecutive two time points during the follow up period, we determined that the salivary function was down regulated and the effect of the treatment was lost. Therefore, the sustained period of improvement by corticosteroid irrigation was between the day when improvement in salivary flow rate was evident and the day when the effect of the treatment was lost (between time points A and B in fig 2).
SALIVARY FLOW RATE TEST
The salivary flow rate of patients with Sjögren’s syndrome was quantified by Saxon test and expressed as grams per two minutes, as described previously.7 Briefly, a sterile gauze was placed in a screw topped 50 ml plastic tube (Blue Max, Falcon Labware, Oxnard, CA) and the dry gauze and tube were weighed. After pre-existing oral fluid was removed, saliva was collected by having patients chew vigorously on the gauze for exactly two minutes (once at every one second). Salivary flow rate was determined by subtracting the original weight from the weight obtained after chewing. A previous work showed that normal control subjects produced ⩾2.75 g/2 min of saliva.8
GRADING OF PATIENTS
We divided all patients with Sjögren’s syndrome into three groups; early, intermediate, and advanced stages. The grading system was based on magnetic resonance (MR) imaging features of the parotid glands in these patients. Those changes in MR features of the glands were proved to reflect increased fat deposition in the glands,7 and, more importantly, were found to be well correlated to the severity of the disease as assessed by the other diagnostic criteria, such as the salivary flow rate (Saxon test),7 the histopathological grading for the labial gland biopsy,9 and the grading for sialographic features of the parotid gland.9 Briefly, patients were categorised as early stages, when they showed MR imaging features of the parotid glands that were slightly affected by the disease, corresponding to grades 1 and 2 as described previously.9 Patients were categorised as intermediate or advanced stage, when they showed MR features of the glands affected moderately or severely, corresponding to grade 3 or 4, respectively.
DATA ANALYSIS
Differences in the salivary flow rates were compared by paired or unpaired t test. Effects of corticosteroid irrigation on the progress of the disease were assessed by χ2 test. Calculations were performed by StatView II software (Abacus Concepts, Berkeley, CA).
Results
The improvement in salivary flow rate was evident at as early as two weeks after the initial corticosteroid irrigation, with the mean (SD) latent period being 3.7 (2.4) weeks after the initial treatment. To exclude the possibility that the observed effects of corticosteroid irrigation on the salivary flow rate was simply because of the irrigation procedure itself, and not because of the corticosteroid action on the parotid gland, we sought to determine whether irrigation with saline solution may have similar effects on the salivary flow rate of these patients. Accordingly, we compared in each of the 28 patients with Sjögren’s syndrome the effects of saline irrigation and corticosteroid irrigation on the salivary flow rate. Saline irrigation did not produce any apparent effect on salivary flow rate in these patients (fig 3A). In contrast, corticosteroid irrigation resulted in significant increases in the salivary flow rate in the same patients (fig 3B). The mean (SD) salivary flow rate of the 28 patients was 0.88 (0.67) g/2 min before saline irrigation and 0.92 (0.70) g/2 min after saline irrigation. In contrast, the mean salivary flow rate increased to 1.74 (1.12) g/2 min after the corticosteroid irrigation.

Effects of irrigation using saline solution (A) and the following corticosteroid solution (B) on the salivary flow rate in patients with Sjögren’s syndrome. The durations between pretreatment and post-treatment were 2–3 months and three weeks for irrigations with the saline and the corticosteroid, respectively. NS: not significant.
Corticosteroid irrigations with aid of the catheter were not associated with any adverse reactions such as pain or infection. Analgesia was not required in placing the catheter in the parotid duct, as we did not need ligations of the catheter to the patient’s oral mucosa.
Next, we compared the efficacy of corticosteroid irrigation between patients at early stages of the disease and those at the advanced stages. To this end, the patients were tentatively classified into three groups (early, intermediate, and advanced stages) on the basis of the grading system described previously,7 ,8 and we determined in each of the different three groups net increases in salivary flow rate after the initial corticosteroid irrigation. Of the 28 patients, 13 were classified as early stage, 11 were intermediate stage, and four were advanced stage. The salivary flow rate determined by Saxon test at the initial examination of these patients were 1.42 (0.59) g/2 min (early), 0.62 (0.47) g/2 min (intermediate), and 0.24 (0.08) g/2 min (advanced). The difference between any two of these groups was statistically significant. The results showed that patients at the advanced stages (0.20 (0.47) g/2 min) obtained smaller net increases compared with patients at the early and intermediate stages of the disease (early; 1.21 (0.57) g/2 min, and intermediate; 0.52 (0.57) g/2 min) (fig 4). Patients in the intermediate stages showed significantly decreased net gain compared with those in the early stages.
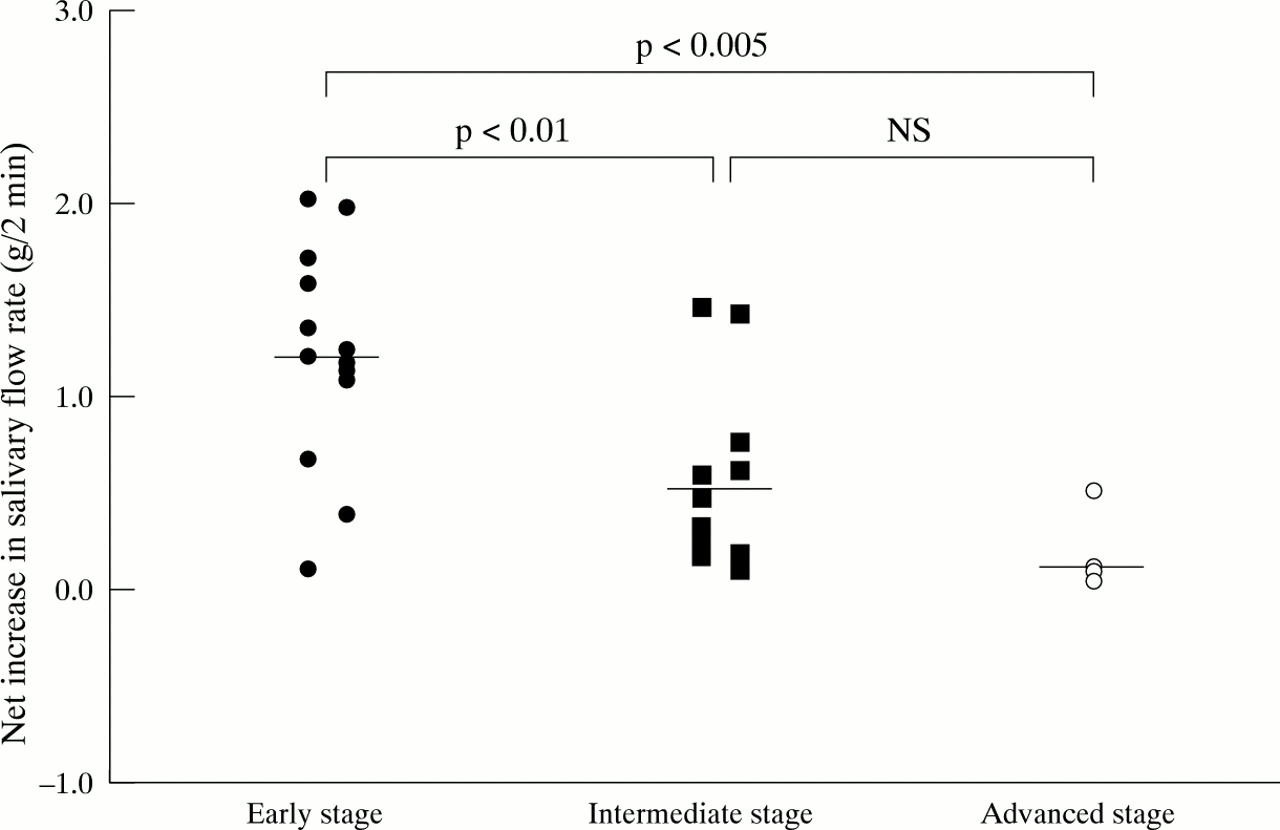
Differences in magnitude of effects of corticosteroid irrigation on the salivary flow rate of patients with Sjögren’s syndrome at early, intermediate, and advanced stages of the disease in the parotid gland. The criteria for the classification of patients into the three groups were described previously (references 7 and 8).
Another concern may be that repeated corticosteroid irrigation may evoke refractoriness of the parotid gland to the agent. If so, corticosteroid irrigation would greatly diminish its value in the treatment of xerostomia. To examine this possibility, we assessed changes in the net increase of the salivary flow rate in the patients who received repeated corticosteroid irrigations. The net increase in salivary flow rate was not found to diminish after repeated corticosteroid irrigations (fig 5). Of the 12 patients treated with more than two series of corticosteroid irrigation (patients 1, 3–5, 7–9, 12, 21, 22, 27, 28), 11 showed net increases similar to, or more than, those observed at the initial corticosteroid treatment. The average sustained period on the 20 patients who had completed at least one series of corticosteroid irrigation (patients 1–9, 11–14, 19–23, 27, 28), was 8.4 (3.5) months (fig 5). The overall percentage of the patients in whom any improvement in symptomatic xerostomia had been recognised was 64% (18 of 28 patients).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
A diagram showing effects of repeated corticosteroid irrigation on improvement of the salivary flow rate of patients with Sjögren’s syndrome. The left column represents the patient’s number (patient no). The second column shows salivary flow rates (SFR (NT) (g/2min)) of 28 patients at the start of corticosteroid irrigation (patients 1 to 28), and of the patients who received long term (up to 35 months) saline irrigations before the start of the saline irrigation (patients 29 to 31). The values in the horizontal tandem bars represent means of the maximum two salivary flow rates (SFR (T)) obtained during the treatment and follow up periods and also sustained periods of improvement in the salivary flow rate (in parentheses) in each of the patients. Each of the tandem bars represents first, second, third, fourth, and fifth series of the corticosteroid irrigation and follow up periods. The three horizontal tandem bars at the bottom demonstrate patients with Sjögren’s syndrome treated with the saline solution alone.
To exclude further the possiblity that the irrigation period was a potent factor in determining the efficacy of irrigation and the presence of the corticosteroid was not a determinant factor, we irrigated the parotid glands of three other patients with Sjögren’s syndrome by saline solution alone for 19 to 35 months. However, the prolonged saline irrigation did not significantly increase the salivary flow rate in these patients (fig 5, patients 29–31). These results were highly suggestive of the usefulness of corticosteroid irrigation in improving impaired salivary flow rate in patients with Sjögren’s syndrome.
Discussion
In this study, we have introduced corticosteroid irrigation using a catheter as a potent candidate for the treatment of xerostomia in patients with Sjögren’s syndrome. The results clearly showed that corticosteroid irrigation could relieve xerostomia in these patients. In addition, improved salivary flow rate was sustained for several months, and repeated irrigation after these sustained periods could again increase the salivary flow rate as effectively as the initial treatment. We were able to perform the repeated cannulation safely in all patients.
Several attempts have been made to improve defective salivary flow rates in patients with Sjögren’s syndrome. Shiozawaet al, in a preliminary study, showed that interferon α increased salivary flow rate in 6 of 10 patients with primary Sjögren’s syndrome.2 Of these, eight showed per cent increases in salivary flow rate of more than 38%. In this study, 23 of 28 patients showed per cent increases of salivary flow rate of more than 40% after the first series of corticosteroid irrigations, with the average per cent increase being 123%. An electrostimulator has been used to increase the salivary flow rate in patients with Sjögren’s syndrome.1 The treatment was successful and resulted in an increase in the production of saliva associated with a reduction of patients’ symptoms, including difficulty in swallowing and the burning sensation of the tongue. More recently, efficacy of polymer based saliva substitutes were evaluated for treatment of xerostomia in patients with primary and secondary Sjögren’s syndrome.3 This approach was not intended to increase salivary flow rate, but to reduce the symptoms of the patients. However, no saliva substitute was found to be truly effective; there was no significant difference in the reduction of patients’ symptoms after using the substitutes. We found in this study that corticosteroid irrigation was as equally effective as interferon α or an electrostimulator in increasing salivary flow rate. We also found that corticosteroid irrigation was useful for the long term treatment of xerostomia.
Systemic corticosteroid treatment has been widely used to control various autoimmune diseases, including systemic lupus erythematosus, rheumatoid arthritis, systemic sclerosis, and autoimmune hepatitis.10-12 Systemic corticosteroid treatment was also effective in improving lymphocytic interstitial pneumonitis associated with Sjögren’s syndrome.13 However, to date, corticosteroid treatment has not been reported as a method of treatment for xerostomia in patients with Sjögren’s syndrome. Systemic corticosteroid treatment improved the condition of xerostomia in patients who had developed Sjögren’s syndrome associated with one or more of the other autoimmune diseases. It is unlikely, however, that systemic absorption of the prednisolone from the parotid ducts caused the observed increases in the salivary flow, as the improvement in the salivary flow rate after systemic administrations of corticosteroids were reported to be short lived.14 In contrast with this, the corticosteroid irrigation caused long lived improvement of the salivary flow rate in this study. Taken together with the present findings, these results suggest a possible role of corticosteroids in improving the impaired salivary flow rate in patients with Sjögren’s syndrome.
At present, the precise mechanism of the improvement by corticosteroid of impaired salivary flow rate in patients with Sjögren’s syndrome is not clear. The observed ineffectiveness of irrigation using saline solution alone indicated that the increased salivary flow rate in patients receiving corticosteroid irrigation was not a result of non-specific effects produced by the irrigation procedures. The salivary gland pathology of Sjögren’s syndrome is characterised by a focal periductal infiltrate consisting mainly of T and B lymphocytes.15 Corticosteroids not only have anti-inflammatory effects, but also inhibit T cell activation. Therefore, it is reasonable to consider that corticosteroids inhibited the activation of the T cells infiltrating into the parotid glands. However, the inhibitory effects of corticosteroids on T cell function was observed to be short lived in patients with multiple sclerosis who were treated with intravenous administrations of the drug14; a result that was inconsistent with the long lived effects of corticosteroid irrigation of the parotid glands observed in the present study.
This study has shown that corticosteroid irrigation treatment was very effective in improving the salivary flow rate in patients with Sjögren’s syndrome. However, corticosteroid did not upregulate the salivary flow rate to the levels of healthy subjects, and at most it inhibited the further progress of the disease.
Therefore, it may be critical to start corticosteroid irrigation as soon as possible after the diagnosis of the disease is made. In addition, the present findings that corticosteroid irrigation was less effective in patients with advanced Sjögren’s syndrome may indicate that it is the patients at early stages who may benefit from corticosteroid irrigation. Doctors should refrain from corticosteroid irrigation in patients with hypersensitivity to corticosteroids. Otherwise, corticosteroid irrigation has not been associated with any toxicity or side effects. However, it should be noted that repeated irrigations with saline solutions before the start of corticosteroid irrigation seem critical for avoiding unexpected swelling of the gland during the treatment period.
We did not irrigate the patients’ submandibular glands, which contribute greatly to the salivary flow rate of these patients. The salivary irrigation involved only both parotid glands in each of the patients, but assessment included only whole salivary flow measurement. Separate measurements of the parotid flow rate should have been used to assess more precisely the effect of corticosteroid irrigations on the salivary function of the parotid gland. In this context, Hallet al previously introduced a device, which allows the collection of the saliva only from the parotid gland,16 but this was not available for this study. In any case, it is plausible that simultaneous corticosteroid irrigation of the submandibular glands could further improve the impaired salivary flow rate in patients with Sjögren’s syndrome, and this is a promising clinical trial to be undertaken in future studies.
Acknowledgments
This work was supported by the Grant in Aid for Scientific Research (C) (no 09671927) from the Japanese Ministry of Science, Education, Sports, and Culture.