Article Text

Abstract
OBJECTIVES The aim of this study was to evaluate serum interleukin (IL) 12 concentration in patients with juvenile chronic arthritis (JCA), according to disease subtype, activity, and duration. IL12 has been demonstrated to prime the selective expansion of T helper (Th) cells with a Th1-type pattern of cytokine production.
METHODS Sixty eight serum samples from 50 JCA patients (12 systemic, 12 polyarticular, 26 pauciarticular), 20 serum samples from age matched healthy controls were tested with two different immunoassays specific for total IL12 (p40 and p70 heterodimer) and for IL12 (p70) heterodimer, respectively. The following disease activity parameters were evaluated: (a) presence of arthritis at least in one joint, (b) physician global estimate of disease activity, (c) disability index according to the Childhood Health Assessment Questionnaire (CHAQ), (d) C reactive protein (CRP).
RESULTS Total IL12 (p40 and p70 heterodimer) was significantly higher in JCA active patients than in those on clinical remission and in healthy controls (p < 0.001). Conversely, detectable concentrations of IL12 (p70) heterodimer were found in three active JCA patients only. Moreover, total IL12 (p40 and p70 heterodimer) showed a significant negative correlation both with time from disease diagnosis (r = −0.29, p = 0.04) and, for the pauciarticular subgroup, with disease activity duration (r = − 0.71, p < 0.001).
CONCLUSIONS This study shows that the p40 moiety of IL12 is increased in serum samples from active JCA patients, especially in the earliest phases of the disease, whereas biological active IL12 (p70) heterodimer is virtually undetectable.
- juvenile chronic arthritis
- interluekin 12
- cytokines
- T helper cells
Statistics from Altmetric.com
T cells are thought to play a pivotal part in the initiation of the inflammatory process in rheumatoid arthritis (RA).1 In the recent years, T helper (Th) cells have been functionally subdivided into two major subpopulations, namely Th1 and Th2 according to their patterns of cytokine production after activation.2 ,3
In humans, Th1 cells produce mainly interferon (IFN) γ and interleukin (IL) 2, whereas the Th2 subset is characterised by a selective production of IL4 and IL5.4-6
Recently, evidence has been provided that some immunoregulatory cytokines play a pivotal part in inducing the polarisation of naive CD4+ T cells (Th0) after activation into the Th1 or Th2 subsets.2 In this respect, IL4 has been shown to be the most potent inducer of Th2-like polarisation, whereas IL12 has been identified as the best stimulator of Th1-like differentiation.7
IL12 is a cytokine composed of a heavy (p40) and a light chain (p35) covalently linked to form a biologically active heterodimer (p70); IL12 is produced by phagocytic cells, B cells, and other antigen presenting cells.7
During the early phases of infection with intracellular pathogens, IL12 favours a Th1 polarisation through: (a) the rapid induction of IFN γ production by NK and T cells, (b) the inhibition of IL4 producing cells, and (c) the induction of optimal proliferation and cytokine production by mature Th1 cells.8 ,9
Both immunohistological and cellular studies have shown that T cells infiltrating the synovial membranes10 as well as synovial fluid T lymphocytes of patients affected with rheumatoid arthritis(RA)11 and JCA12 display a predominant Th1-type pattern of cytokine production.
The aims of this study were: (a) to investigate IL12 serum concentrations in JCA patients according to the various subtypes and to the degree of disease activity and (b) to look for possible differences in IL12 expression according to the duration of disease activity.
Methods
Fifty patients with JCA (28 male, 22 female) followed up at the Paediatric Rheumatology Unit of the Institute and 20 age matched controls were included in the study. The mean age of the JCA patients ranged from 1 to 16.3 years. According to the EULAR criteria13 12 patients were affected with systemic JCA (mean age: 5.8 years, range 2.7–12), 12 with polyarticular JCA (mean age 10.4 years, range 3.1–14), and 26 with pauciarticular JCA (18 with an early onset subtype and eight with a late onset subtype; mean age 6.7 years, range 2.1–15).
Clinical parameters for disease activity were (a) presence of active arthritis (with presence of swelling and/or limitation of movement or tenderness) at least in one joint at the clinical examination,14 (b) physician global estimate of disease activity ranging from 3 to 4,15 (c) Disability Index according to the Italian version of the Childhood Health Assessment Questionnaire (I-CHAQ) > 0.4.16
Criteria for inactive disease were (a) no history of arthritis or arthralgias the week before and absence of any sign of active arthritis (as defined above) at the clinical examination, (b) negative C reactive protein (CRP < 0.2 mg/dl), (c) physician global estimate of disease activity = 0,(d) Disability Index = 0.
Sixty eight serum samples obtained from 50 JCA patients were retrospectively tested for IL12 concentrations. The corresponding values of white blood cell (WBC) count, haemoglobin concentration (Hb), CRP, and erythrocyte sedimentation rate (ESR) were recorded on each occasion (table 1).
Disease activity parameters (mean (SD)) of the different JCA subgroups at the time of the study
Time from disease diagnosis was recorded for all active JCA patients. The mean time was 82.3 weeks (range 4–336). Moreover, in the 26 pauciarticular active JCA patients, the time between the first onset of symptoms or disease relapse and serum collection was also recorded. The mean time was 5.2 weeks (range 1–16). Serum samples from most recent onset arthritis were obtained from patients seen at the orthopaedic department during a paediatric rheumatological consultation for an “arthritis of unknown origin”. Only serum samples from patients with a final diagnosis of JCA after three months of disease were retrospectively evaluated.
Aliquots of serum samples were frozen at −80°C soon after sample collection. IL12 was assayed by two different immunoassays specific for total IL12 (p40 and p70 heterodimer) and for the IL12 (p70) heterodimer from Amersham International plc (Amersham Place, England) according to the instructions of the manufacturer.Sensitivity are reported to be 5 pg/ml for IL12 (p40 and p70) and 3 pg/ml for IL12 (p70). For each patient, IL12 (p40) was calculated as the difference between total IL12 (p40 and p70) and IL12 (p70) serum concentrations.
Twenty age matched healthy subjects attending at our clinic for a control visit after an acute self limiting inflammatory or infectious disease were used as controls after informed consent of the parents. Only patients with no history of inflammatory disorders in the four weeks before the examination and with negative clinical and laboratory signs of inflammation were considered.
Quantitative differences between patient groups as for IL12 serum concentration were assessed by non-parametric statistical analysis using the Mann-Whitney U test. Correlations among serum IL12 and parameters of disease activity were determined by Spearman’s rank parameters test.
Results
Total IL12 (p40 and p70 heterodimer) was detected both in active (range 70–1130 pg/ml) and in inactive (range 20–365 pg/ml) JCA patients and in healthy controls (range 15–156 pg/ml). Conversely, detectable concentrations of IL12 (p70) were found (mean (SD): 5.3 (0.3) pg/ml; range 4.6–6.5 pg/ml) in three active JCA patients (one systemic, one polyarticular, and one pauciarticular) only. These results clearly demonstrated that virtually all of the total serum IL12 detected in JCA patients was attributable to IL12 p40 alone. Therefore, from now onwards, we shall refer to IL12 (p40) instead of total IL12.
Figure 1 shows the behaviour of IL12 (p40) serum concentration for the three JCA subgroups and statistical differences among active and inactive JCA patients and healthy controls. Notably, systemic inactive JCA patients displayed significantly higher IL12 (p40) serum concentrations as compared with controls (p = 0.02, not shown). No differences were noted between inactive polyarticular and pauciarticular JCA and controls.

Difference in IL12 (p40) serum concentration among systemic, polyarticular, and pauciarticular JCA patients with active and inactive disease and age matched healthy controls. The horizontal lines represent the mean values detected in each study group.
Overall, IL12 (p40) serum concentrations displayed a significant positive correlation with major inflammatory parameters: CRP (r = 0.35, p = 0.01) and ESR (r = 0.3, p = 0.04). Moreover, a negative significant correlation with Hb (r = −0.4, p < 0.001) was disclosed (not shown).
An additional goal of our study was to look for possible variations in IL12 (p40) serum concentration according to the disease duration. When IL12 (p40) serum concentrations were correlated in all active JCA patients with the time from disease diagnosis a significant negative correlation was disclosed (r = −0.29, p = 0.04). Notably no other disease activity parameter showed such a similar negative correlation (not shown).
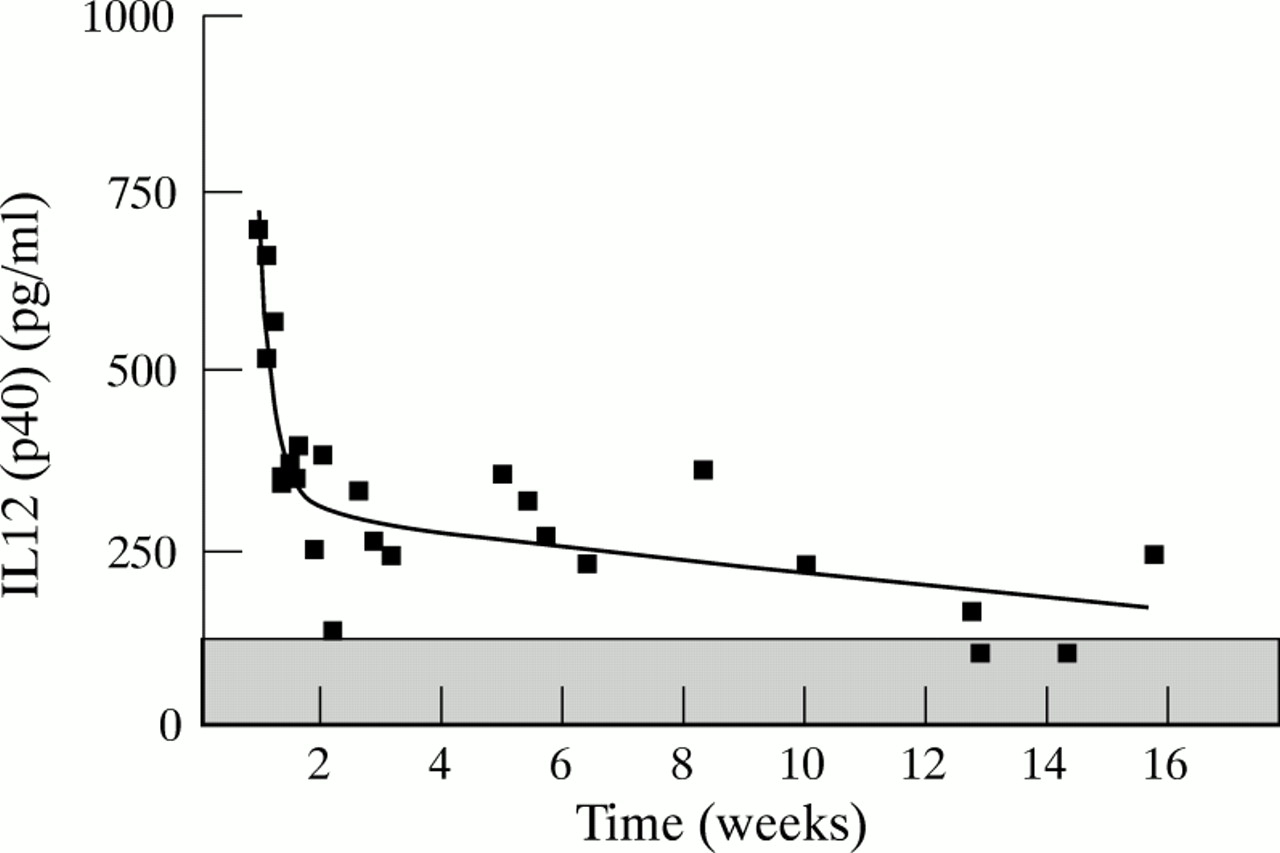
More interestingly, the same pattern was observed when the series of 26 active pauciarticular JCA patients was next evaluated according to the time from the onset or last relapse of their arthitis. Also in this case, the IL12 (p40) serum concentrations and not other disease activity parameters, showed a significant negative correlation with the time from disease onset or last relapse (r = −0.71, p < 0.001). IL12 (p40) decreased steeply during the first weeks of active disease with a slower decrease in the subsequent weeks. The data obtained fit with the two phase exponential decrease curve reported in figure 2 (r 2 =0.77). The time corresponding to the change of the slope of the curve was 13.7 days (fig 2).
{kind=link}
{kind=link}
Cross sectional study of IL12 (p40) serum concentrations in active pauciarticular JCA patients according to duration of disease activity. Cut off value was 145 pg/ml (hatched area). Data were fitted by a two phase exponential decrease curve (r2 = 0.77).
Based upon these kinetics the clinical features and treatment at the time of the study of patients evaluated during (group A) or after (group B) the first two weeks of active disease were retrospectively evaluated. As reported in table 2 no difference in the degree of disease activity was disclosed. Although no patient was receiving any disease modifying anti-rheumatic drug or intra-articular corticosteroids for a period lesser than four months, it cannot be formally excluded that such a difference could be related to the different proportion of NSAID treated patients between group A and B (table 2).
Clinical and laboratory features of active pauciarticular JCA (pJCA) patients at the time of the study
Discussion
A major feature of IL12 is its ability to prime the selective expansion of T helper cells with a Th1-type pattern of cytokine production that plays a central part in host protection against intracellular pathogens.2 ,7
Preferential expansion of Th1 cells has been recently associated with some animal models of immunopathological disorders such as, for example, autoimmune diabetes and collagen induced arthritis.17 ,18 As for RA, T cell cloning experiments, staining of freshly isolated cells for intracellular cytokines, and RT-PCR analyses of biopsy samples have all demonstrated that CD4+ lymphocytes present in the synovial fluid or membranes produce IL2 and IFNγ, but little or no IL4 or IL5.10 ,11 The same pattern was recently described also for JCA.12
Based upon these premises, we have here investigated the serum concentrations of IL12 in a group of JCA patients. The working hypothesis was that an increase of circulating IL12 would have been strictly connected with the in vivo generation of Th1-type effector cells. Although the serum concentrations of total IL12 (p40 and p70 heterodimer) were found to be significantly increased in active JCA patients compared with inactive patients and healthy controls, the biologically active IL12 (p70) heterodimer was virtually absent from all the samples tested. Thus IL12 (p40) alone was the only cytokine moiety detected in our patient series, showing a good correlation with disease activity.
These data are in line with a recent report in adult RA patients showing mRNA overexpression of IFNγ and IL12 (p40) by synovial fluid mononuclear cells during the arthritic flare up.19 In the same study serum IL12 (p70) heterodimer was practically undetectable.19
The finding that IL12 (p40) but not IL12 (p70) heterodimer was detected in serum samples from JCA patients is not easily explained. A 10–100 excess of IL12 (p40) over IL12 (p70) heterodimer secretion has been detected in the supernatants of cultured macrophages and EBV infected B lymphoblastoid cell lines.7 Thus, IL12 (p40) overexpression in the serum samples of patients may simply reflect the physiological ratio between secreted IL12 (p40) and (p70) heterodimer. Notably in this respect, expression of IL12 (p40) mRNA is restricted to those cell types that can produce the IL12 (p70) heterodimer.7
An alternative hypothesis is that the newly produced IL12 (p70) heterodimer is rapidly sequestered by binding to surface receptors on target cells. This assumption holds true especially for IL12 (p70) synthesised at the site of an ongoing inflammatory process. A similar behaviour has been reported in RA and JCA for tumour necrosis factor (TNF)α that, although considered as a major player in the pathogenesis of these diseases, is barely detectable in the serum samples of patients. In contrast, TNF soluble receptors levels are increased in RA and JCA and correlated with disease activity.21 ,22
An additional aim of our study was to investigate the behaviour of IL12 serum concentration according to disease duration. In this respect our data seem to support the hypothesis of a major involvement of the cytokine during the early phases of the disease. In particular, when pauciarticular active JCA patients were studied, IL12 (p40) serum concentrations were clearly higher during the first weeks of disease activity. This issue is in line with the observations that (a) IL12 dependent Th1 polarisation occurs during the very early phases of intracellular infection and experimental autoimmune diseases,7 ,17 and (b) IL12 primes CD4+ and CD8+ cell clones for high production of IFNγ during the first weeks of culture. After that time the priming is irreversible even in the absence of IL12.22
In conclusion, this study provides the first, although circumstantial, evidence of a possible role of IL12 in JCA, especially in the earliest disease phases. Further studies to elucidate the mechanisms governing the release of IL12 (p40) and IL12 (p70) heterodimer into biological fluids in JCA are needed.
Acknowledgments
We would like to thank Dr M P Sormani for her help in statistical analysis.