Article Text

Abstract
OBJECTIVE To examine the relation between rate of synovial membrane enhancement, intra-articular pressure (IAP), and histologically determined synovial vascularity in rheumatoid arthritis, using gadolinium-DTPA enhanced magnetic resonance imaging (MRI).
METHODS Dynamic gadolinium-DTPA enhanced MRI was performed in 31 patients with knee synovitis (10 patients IAP study, 21 patients vascular morphometry study). Rate of synovial membrane enhancement was quantified by line profile analysis using the image processing package ANALYZE. IAP was measured using an intra-compartmental pressure monitor system. Multiple synovial biopsy specimens were obtained by a blind biopsy technique. Blood vessels were identified immunohistochemically using the endothelial cell marker QBend30 and quantified (blood vessel numerical density and fractional area).
RESULTS Median blood vessel numerical density and fractional area were 77.5/mm2 (IQR; 69.3–110.7) and 5.6% (IQR; 3.4–8.5) respectively. The rate of synovial membrane enhancement (median 2.74 signal intensity units/s, IQR 2.0–3.8) correlated with both blood vessel numerical density (r = 0.46, p < 0.05) and blood vessel fractional area (r = 0.55, p < 0.02). IAP did not influence the rate of enhancement.
CONCLUSIONS Gadolinium-DTPA enhanced MRI may prove to be a valuable technique for evaluating drugs that influence angiogenesis.
- magnetic resonance imaging
- rheumatoid arthritis
- synovitis
- vascularity
Statistics from Altmetric.com
Magnetic resonance imaging (MRI) after intravenous administration of gadolinium-diethylenetriamine pentaacetic acid (Gd-DTPA) has become an established tool for demonstrating inflammatory synovial proliferation in rheumatoid arthritis (RA).1-4Rate of contrast enhancement has been shown to correlate with the inflammatory activity of the proliferating synovium,1-3and is significantly reduced after intra-articular glucocorticoid installation.5 The technique has also been proposed as being superior to clinical or radiographic techniques for evaluating disease progression and may have prognostic value with regard to the future development of bone destruction.6 ,7
Inflammation is characterised by increased tissue perfusion and capillary permeability. Synovial uptake of Gd-DTPA (enhancement) is dependent on local tissue perfusion and microvascular permeability,8 resulting in leakage of intravenously injected contrast medium into the interstitial space. This is manifest as increased signal intensity (brightness) on T1-weighted MR images. We have previously described a method for defining the “synovium-only” phase of Gd-DTPA uptake in the synovium of patients with RA using the image processing package “ANALYZE”, and demonstrated a significant correlation between rate of synovial membrane enhancement and certain histopathological features of synovitis; polymorphonuclear leucocyte infiltration, hyperaemia, fibrin deposition.1 It has been proposed that it may be possible to grade the vascularity of proliferative synovitis using this technique, and therefore differentiate “active” hypervascular, pathologically permeable, inflammatory synovial proliferation from non-inflammatory, “inactive” fibrous tissue.3 No study however has attempted to quantitatively validate this hypothesis.
The rate of transport of small plasma solutes such as Gd-DTPA into the synovial bed and joint fluid depends on multiple factors; systemic blood pressure and vascular resistance, the flow of fluid from the synovial bed to the joint space and clearance thereof, synovial permeability, and the concentration gradient across the synovium. The net flow of solutes and fluid is therefore largely determined by the balance between the osmotic and hydraulic pressures within the capillaries and joint space.9 ,10 Intra-articular pressure (IAP) is raised in patients with RA,11 ,12 and can theoretically compromise synovial microvascular blood flow. For these reasons, the influence of IAP on synovial membrane enhancement needs to be evaluated.
This study was designed to develop a quantitative technique for assessing synovial vascularity based upon Gd-DTPA enhanced MRI and discover if IAP can compromise the validity of the technique.
Methods
PATIENTS
All study protocols were considered and approved by the City and East London Research Ethics Committee. Patients fulfilled the American College of Rheumatology criteria for the diagnosis of RA,13 and were recruited from a general rheumatology clinic. All presented with a “disease flare” as defined by an Index of Disease Activity (IDA) greater than 2,14 and clinical evidence of knee synovitis (pain, tenderness, joint effusion; positive bulge sign and patellar tap). In patients with bilateral knee synovitis, the most painful joint was selected for study. Informed written consent was obtained from all participants.
MRI PROTOCOL
Imaging was performed using a 0.5 Magnetom Unit (Shimadzu Medical Systems, Tokyo, Japan) equipped with a dedicated cylindrical knee coil. During the examination, patients were placed in the supine position with the knee fully extended in the neutral position. A dynamic T1 weighted spin echo sagittal sequence was obtained through the suprapatellar bursa (TR/TE 180/20 ms, FOV 30 cm, Ma 256 × 256, four slices, slice thickness 5 mm, imaging time 48 seconds, 16 loops). Immediately after the acquisition of baseline images (1st loop), bolus intravenous Gd-DTPA (0.1 mmol/kg body weight; Nycomed, UK) was administered via a 21 G butterfly needle inserted into an ante-cubital fossa vein. The total imaging time was 12 minutes 46 seconds.
MRI QUANTIFICATION
Data were transferred from the MRI console to a SUN workstation and analysed using the image processing package ANALYZE from the Mayo clinic (15; CN Software Inc, Rochester, Minnesota, USA). Significant patient knee movement was assessed by performing line profile analysis in two orthogonal planes as outlined in previous studies.1Line profile measurements were conducted in synovium lining the anterior surface of the suprapatellar bursa. The voxel demonstrating the maximum rate of enhancement (increase in voxel signal intensity/time) in the initial linear phase of development of increased signal intensity (SIt -SIo/t) was recorded in each line profile, where SIt is the signal intensity obtained t seconds after contrast injection, SIo is the signal intensity in the first non-enhanced image, and t is the time taken to reach peak enhancement in the initial linear phase of development of increased signal intensity. Four approximately equidistant sample sites were selected for line profile analysis in each of the four slices, extending from apex to inferior pole of the suprapatellar bursa and without specific reference to apparent synovial thickness at any site. This provided 16 readings for each patient from which the median value for rate of synovial membrane enhancement was calculated. To assess reproducibility of the system, MR data analysis was undertaken on two occasions in 10 randomly selected patients (160 measurements).
CONSECUTIVE DAY MRI
Studies were undertaken to assess the reproducibility of MRI as an imaging technique. Five female patients were recruited to undergo MRI on consecutive days. The median patient age and disease duration were 58 years (range 41–78) and 10 years (8–41) respectively. All patients were seropositive (rheumatoid factor>40 iu/l) and had radiographic evidence of bone erosion as assessed by standard hand and feet radiographs.
INTRA-ARTICULAR PRESSURE STUDY
IAP was measured in the knee joints of 10 patients; 8 female, median age 60 years (range 40–78), median disease duration 12 years (range 7–41) and recorded in mm Hg. Five of these patients also participated in the consecutive day MRI study and were recruited at the time of the day 2 MR examination. IAP was measured immediately after MR examination before the patient was moved from the examination couch using the hand held portable 295–1 Intra-Compartmental Pressure Monitor System (Stryker, UK). This method is outlined in our previous IAP studies.12 Immediately after the procedure, the joint was aspirated to dryness and volume of synovial fluid recorded.
VASCULAR MORPHOMETRY STUDY
Patients
Twenty one patients; 14 female, median age 58 years (range 37–72), median disease duration 15 years (range 1–38) were recruited. Clinical, laboratory, and semi-quantitative histological data derived from these patients has previously been reported.1Seventeen patients had seropositive disease and 19 had radiographic evidence of bone erosion (hand and feet radiographs). Ten patients were receiving disease modifying anti-rheumatic drugs (three sulphasalazine, three azathioprine, two methotrexate, one gold, one penicillamine).
Synovial biopsy and tissue preparation
Immediately after MRI examination, patients underwent blind synovial biopsy of the suprapatellar bursa. Subcutaneous tissues were infiltrated with local anaesthetic (2% lignocaine), and multiple biopsy specimens taken using a Parker Pearson synovial biopsy needle (16; Popper and Sons Inc, New York, USA). The needle was positioned to obtain all biopsy specimens from the anterior surface of the suprapatellar bursa and within the range of the needle. Specimens were embedded in optimal temperature cutting compound (OCT; Miles Laboratories, Elkhart, IN), snap frozen using isopentane in liquid nitrogen, and stored at −70°C. Cryostat sections were cut at 5 μm— 6 μm.
Immunohistochemistry
Blood vessels were identified immunohistochemically using the endothelial marker QBend30 (Serotec Ltd, Kidlington, Oxford, UK), by an immunoperoxidase technique.17 Endogenous peroxidase activity was blocked by incubating the tissues with 0.3% H2O2 in methanol for 30 minutes. The slides were then rinsed in phosphate buffered saline (PBS; two washes of five minutes each). Non-specific binding sites were blocked by incubating the slides in PBS containing 0.05% bovine serum albumin (BSA) and 0.015% horse serum for 20 minutes at room temperature. The primary antibody, made up in PBS containing 0.05% BSA and 0.015% horse serum, was applied at a dilution of 1:200.
After an incubation period of one hour at room temperature, the sections were rinsed (two washes of five minutes each) in PBS. The binding of the primary monoclonal antibody was detected by the avidin-biotin-peroxidase (ABC) method,18 using a Vector Elite biotinylated antimouse ABC kit (Vector Laboratories, Wolfric Square, Peterborough, UK). A standard diaminobenzidine tetrahydrochloride (DAB) enhancement technique was used to increase staining sensitivity.19 The slides were then washed in cold running tap water, dehydrated in alcohol, cleared in xylene, and mounted. Tonsil sections served as positive controls, and sections where the primary MAb was omitted as negative controls.
Vascular morphometric assessment
Only synovium in which the lining was clearly evident was included in the study. Blood vessels greater than 15 μm in diameter were quantified throughout the superficial 200 μm of synovium in all biopsy specimens using the Symphony image analysis system (SeeScan, Cambridge, UK) and expressed as blood vessel numerical density (number of vessels per square millimetre) and blood vessel fractional area (area enclosed within and including vascular endothelium expressed as a percentage of the total biopsy specimen area) respectively. Vascular morphometric analysis was repeated in one randomly selected biopsy specimen from each patient to assess reproducibility of this technique.
STATISTICAL ANALYSIS
Data were not normally distributed, therefore, non-parametric statistical methods were applied. All results are reported as medians (interquartile range). Reproducibility measurements were calculated using the interclass correlation “r 1”.20 Other data were compared using Wilcoxon’s signed rank test or Spearman’s rank correlation coefficient, as appropriate. p Values less than 0.05 were considered significant.
Results
CONSECUTIVE DAY IMAGING AND REPRODUCIBILITY OF THE MRI QUANTIFICATION TECHNIQUE
Figure 1 is a sagittal section through an RA knee joint before and after intravenous administration of Gd-DTPA. Four of five patients exhibited synovial membrane enhancement on consecutive days, the fifth patient did not show enhancement on either day. The median change in rate of enhancement was 0 (−0.187 to 0.525) signal intensity units/s. The interclass correlation’s for consecutive day imaging and the MRI quantification technique were r 1=0.93 andr 1=0.98 respectively.

Sagittal section through a rheumatoid knee joint before and after intravenous administration of gadolinium-DTPA.
IAP STUDY
The median resting IAP was 16 mm Hg (14–20) and median volume of aspirated synovial fluid 14 ml (8–23). Synovial membrane enhancement was observed in nine of 10 patients, median rate 2.93 signal intensity units/s (2.4–3.4). There was no relation between rate of synovial membrane enhancement and IAP (fig 2; r =−0.091, p =0.69), however, a significant relation was observed between rate of synovial membrane enhancement and volume of synovial fluid aspirated (fig 3; r =0.755, p <0.05).
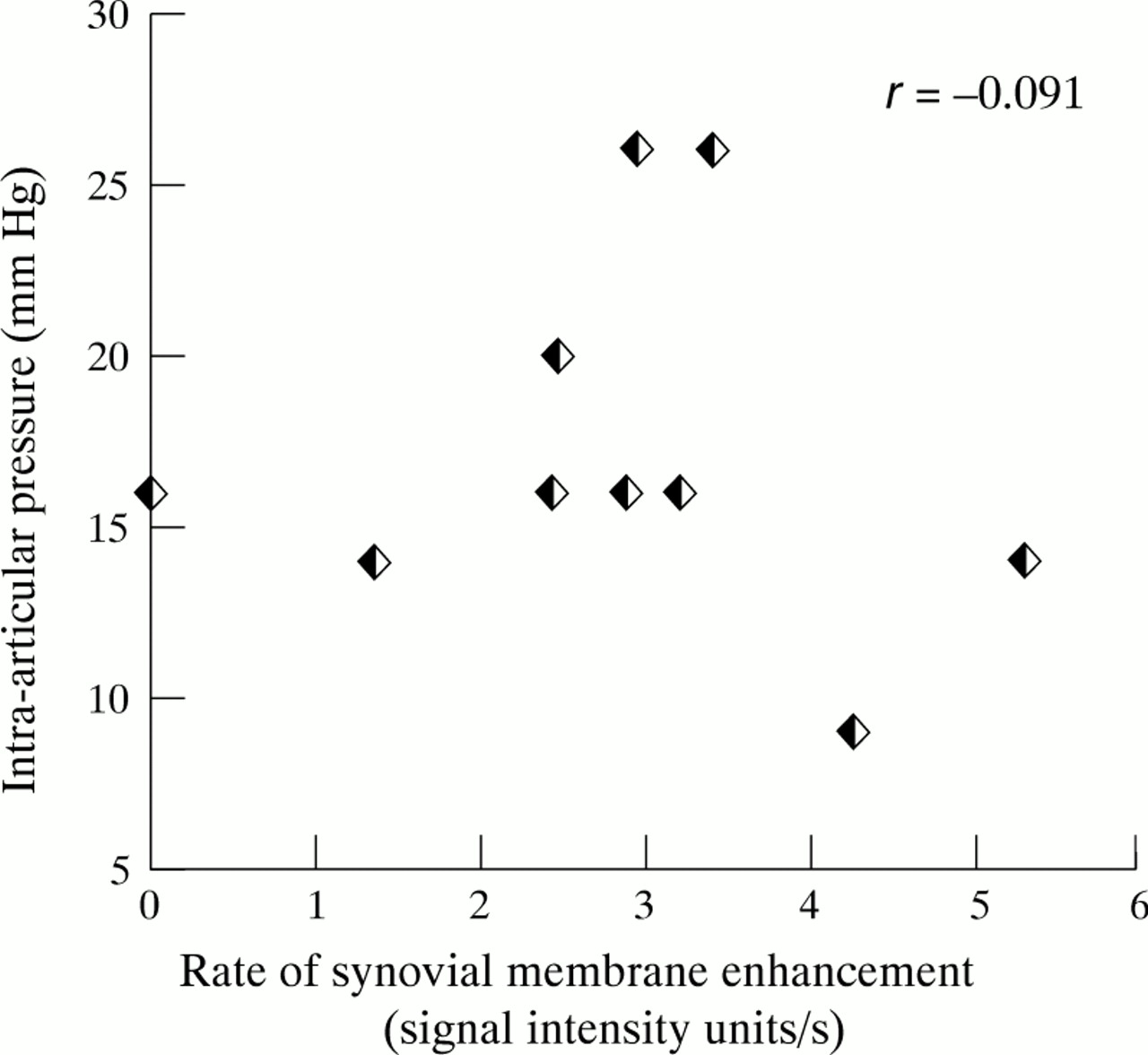
Relation between rate of synovial membrane enhancement and resting intra-articular pressure.

Relation between rate of synovial membrane enhancement and volume of synovial fluid aspirated.
VASCULAR MORPHOMETRY STUDY
Significant knee movement was detected in one patient who was excluded from the data analysis. Nineteen of the remaining 20 patients exhibited synovial membrane enhancement after administration of Gd-DTPA, median rate 2.7 signal intensity units/s (2.0–3.8). Figure 4shows the synovial microvascular bed as identified by QBend 30. Ninety eight biopsy specimens were examined; median four specimens per patient (IQR 3–6). The median blood vessel numerical density and fractional area were 77.5 vessels/mm2 (56.4–104.9) and 5.6% (3.8–7.8) respectively. An evaluation of the reproducibility of the vascularity quantification system showed that the interclass correlations between blinded duplicate assessments on the same sections (n=20, one randomly selected biopsy specimen from each patient) werer 1=0.93 (numerical density) andr 1=0.95 (fractional area) respectively. Figures 5 and 6 show the relation between rate of synovial membrane enhancement and blood vessel numerical density (r=0.46, p<0.05) and blood vessel fractional area (r=0.55, p<0.02) respectively.

Rheumatoid synovial microvascular endothelium identified immunohistochemically by QBend 30.
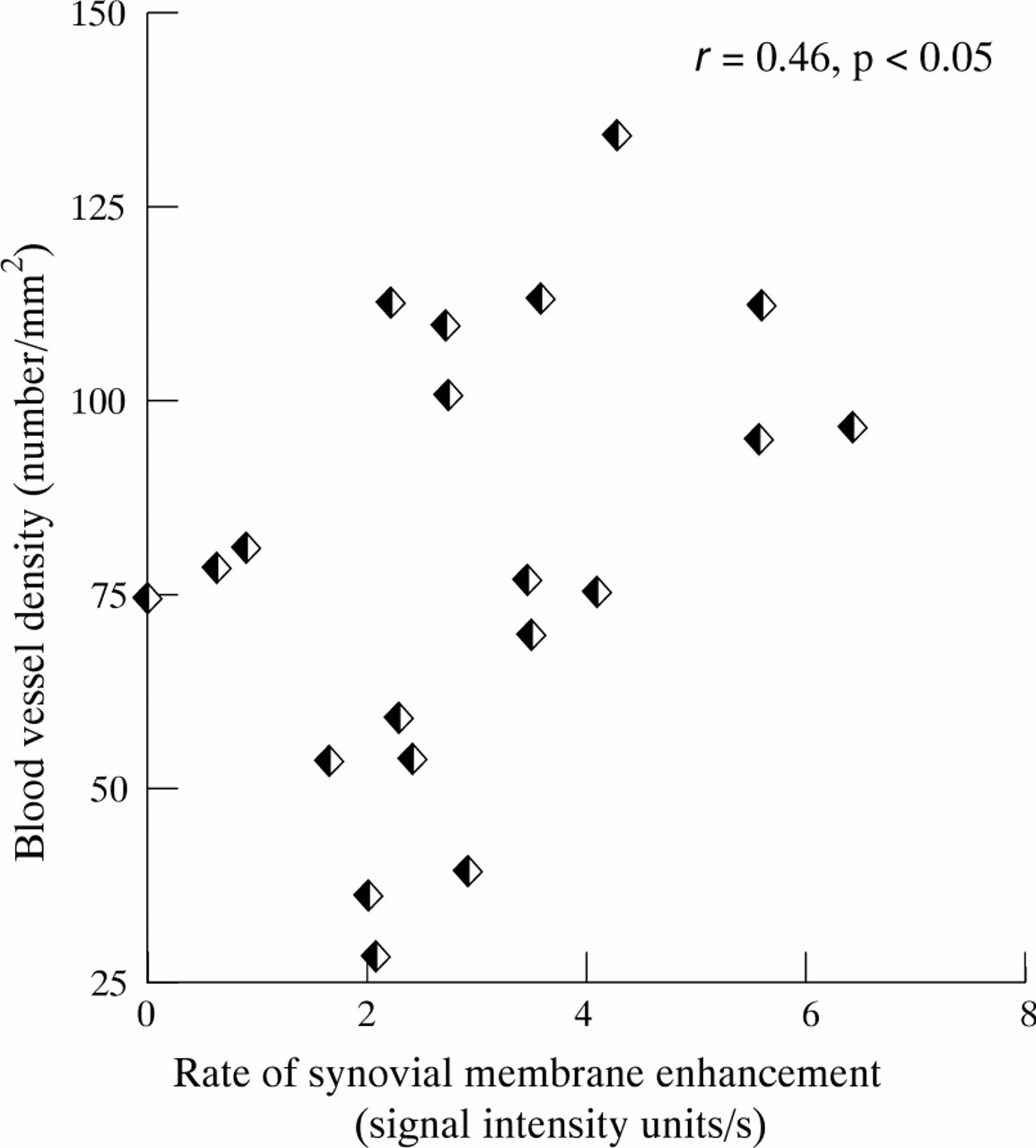
Relation between rate of synovial membrane enhancement and blood vessel numerical density.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Relation between rate of synovial membrane enhancement and blood vessel fractional area.
Discussion
This study describes a reproducible method for quantifying histologically determined synovial vascularity using Gd-DTPA enhanced MRI in rheumatoid patients with knee synovitis. The rate of synovial membrane enhancement correlated with both blood vessel numerical density (p<0.05) and blood vessel fractional area respectively (p<0.02). IAP did not influence the rate of synovial membrane enhancement.
One of the earliest features of rheumatoid synovitis is the development of a new vascular network, which serves to promote the delivery of cells and nutrients to the invading pannus.21 Histological studies in patients with early RA (disease duration less than three years), who had clinical and histological evidence of knee synovitis have shown a significant increase in both vascular proliferation and number of blood vessels per square millimetre as compared with postmortem control samples.22 In patients with longstanding “burned-out” disease, there is a gradual loss of vascularity resulting in hypervascular pannus being replaced by fibrous tissue.23 ,24 Stevens et al examined synovial tissue specimens from rheumatoid patients undergoing knee arthroplasty (mean disease duration 15 years) who by definition had chronic disease.25 Synovial capillaries were buried at a modal depth of 75 μm, approximately twice that found in normal synovium, with a numerical density of 80.2 mm2, approximately one third of normal. In clinically unaffected knee joints, the number of vessels per square millimetre is similar to control samples and vascular proliferation is not seen even though perivascular mononuclear cell proliferation and synovial lining layer thickening may be evident.22 These findings suggest that angiogenesis represents a critical stage in the evolution and progression of synovitis.
The role of neovascularisation in the pathogenesis of RA is supported by other findings. Angiogenic cytokines have been demonstrated in rheumatoid synovial biopsy specimens; platelet derived growth factor, tumour necrosis factor α (TNFα), interleukin 8 (IL8), Groα, and vascular endothelial growth factor (VEGF26). VEGF is a hypoxia induced endothelial cell selective mitogen and mediator of changes in synovial permeability, which has been demonstrated in both SF and synovium from active RA patients.27-29 It is therefore a potentially key mediator of the microvascular changes seen early in the pathogenesis of RA.30 Antibodies to VEGF have been found to partially neutralise the proliferative activity of endothelial cells in RA tissue explant cultures,28 and in the rat model of collagen induced arthritis, angiogenesis inhibitors prevent the onset of collagen induced arthritis, suppress established disease,31 ,32 and reduce serum concentrations of VEGF.33 The effects of certain anti-rheumatic drugs—gold salts, D-penicillamine, methotrexate, anti-TNFα—are known to be partly mediated by changes in vascular endothelium.34-36
Although we have shown that the rate of synovial membrane enhancement relates to histologically determined synovial vascularity, rate of enhancement is a complex process, which also reflects changes in synovial perfusion and microvascular permeability. 133Xenon clearance and laser Doppler flowmetry studies indicate increased synovial perfusion,11 ,37-39 and radionucleotide studies indicate increased synovial permeability40-42 in patients with inflammatory arthritis, however, these variables have proved difficult to quantify in a reproducible fashion. It was beyond the scope of our study to calculate the contributions from synovial perfusion and synovial permeability to the “enhancement” equation. This may explain why the correlation demonstrated between rate of synovial membrane enhancement and histologically determined synovial vascularity was not more statistically significant. To explore the precise physiological mechanisms of “enhancement” further, three dimensional MRI studies at high resolution combined with three dimensional volume imaging and principal component analysis would be needed.
Resting IAP is at or below atmospheric pressure in normal joints becoming more sub-atmospheric during periods of exercise.9 ,12 ,43-45 Low IAP facilitates the flow of fluid into the joint, preserves capillary patency, and ensures that tissue blood supply and nutrition are maintained. In contrast, patients with RA have significantly higher IAP at rest, rising further during exercise.11 ,12 ,45 Artificial volume expansion of both normal and rheumatoid knees (thereby mimicking the effect of an effusion) also increases IAP, the highest pressures being generated in rheumatoid subjects.12 ,43 ,44 ,46 In addition, when an external pressure cuff is applied to rheumatoid knee joints with effusions, even modest increasess in IAP (20 mm Hg) compromise synovial blood flow.47 If IAP exceeded capillary perfusion pressure (estimated to be between 30 and 60 mm Hg), synovial uptake of Gd-DTPA could theoretically be compromised, potentially limiting the ability of this technique for assessing synovial vascularity. In our studies, we did not demonstrate a significant relation between IAP and rate of synovial membrane enhancement, however, there was a significant positive correlation between rate of enhancement and volume of synovial fluid aspirated. These data suggest that IAP does not significantly influence rate of Gd-DTPA uptake by synovium in the rheumatoid knee joint, however, because IAP was measured in the joint cavity itself, whereas MRI was undertaken in the SPB, IAP may not have been the same at both sites because of loculation or compartmentalisation of synovial fluid. The positive correlation between IAP and synovial fluid volume may provide indirect evidence for a relation between synovial enhancement and inflammatory activity as synovial fluid volume itself may be an indicator of inflammatory activity within an individual joint.48
This work describes for the first time the relation between Gd-DTPA enhanced MRI and a quantitative histological measure of disease state. Our findings support the view that Gd-DTPA enhanced MRI may allow us to distinguish “active” hypervascular pannus from “inactive” fibrous disease,3 however further quantitative studies are required to confirm whether this truly represents blood volume or flow or leakage from blood vessels into synovial tissue. Quantifying the rate of synovial membrane enhancement may prove to be a useful technique for evaluating drugs that influence angiogenesis.
Acknowledgments
We are grateful to the staff of the MRI Department, Royal London Hospital, John Holman, PhD, The Hill Centre, Paul Mapp, PhD, David Walsh, PhD, Bone and Joint Research Unit, St Bartholomew’s and The Royal London School of Medicine and Dentistry for technical assistance and advice. This work was supported by a grant from the Arthritis and Rheumatism Council.