Article Text

Abstract
OBJECTIVES A prospective, open study of corticosteroid hip injection (CHI) was performed to determine if different radiological patterns of arthritis vary in their response.
METHODS Forty five patients (15 with rheumatoid arthritis, 27 with osteoarthritis, and three with anklyosing spondylitis) underwent hip injection with 80 mg methyl- prednisolone and lignocaine under x ray control. Outcome was assessed at two, 12, and 26 weeks for pain, range of hip movement, and graded functional questionnaire. Patients estimated their pain in four components, night pain, rest pain, weight bearing, and referred pain, each measured by 10 cm visual analogue score and summed to give a total score out of 40 cm. Hip radiographs were evaluated blindly for pattern and severity of arthritis, as well as for progression between 0 and 26 weeks.
RESULTS Median total pain score decreased from 29 cm at baseline to 22 cm at two weeks (p=0.0001), 24 cm at 12 weeks (p=0.03), but had returned nearly to baseline by 26 weeks (25 cm, p=0.3). Greatest improvement was seen for night pain. Mean range of internal rotation increased from 16 to 28 degrees at two weeks (p=0.03) and 23 degrees at 12 weeks (p=0.06). Functional ability did not change. Hips with an atrophic pattern of arthritis on plain radiography gained negligible pain relief at two weeks compared with hips with a hypertrophic or mixed bone response (p=0.04). The degree of pain relief was similar in patients with OA and RA, and was not influenced by radiographic severity or by the direction of migration of the femoral head.
CONCLUSION Pain and internal rotation improve for up to 12 weeks after CHI. CHI offers a useful and safe therapeutic option for patients with hip arthritis, with the exception of those with a purely atrophic radiological pattern.
- intra-articular injection
- radiography
- hip
- outcome
- arthritis
- corticosteroid
Statistics from Altmetric.com
Arthritis of the hip is a significant cause of morbidity in the elderly population. Osteoarthritis (OA) is the commonest cause and affects 4% of people over the age of 65 years.1 The prevalence of hip involvement in rheumatoid arthritis (RA) may approach 50% in established disease2 with protrusio acetabuli in 5%.3 Although ankylosing spondylitis (AS) is uncommon, the hip is the most commonly involved of the peripheral joints. Total hip replacement provides a successful intervention in end stage hip arthritis, but it is often preceded by years of pain and disability. Moreover, elderly patients may not be suitable for surgery or may not be referred.4 Intra-articular corticosteroids are widely used in inflammatory joint diseases, although their use in OA is more controversial, partly because of lesser efficacy and also because of concerns over deleterious effects.5 ,6
Recently hip arthritis has been separated into radiological subsets.6 The pattern of bone response has been separated into atrophic and hypertrophic types, both of which occur in OA and RA. Atrophic hip arthritis is associated with chondrocalcinosis at the hip and tends to progress more rapidly.7-9 Using the direction of migration of the femoral head, OA has been divided into superior pole and medial (central) types. Superior migration is more common in men, more often unilateral, and more likely to progress.8 ,10 Medial OA is more common in women, tends to be bilateral, and is less likely to progress8 10: there are conflicting data regarding its association with generalised nodal OA.7 ,11 In OA 82% of hips show superior pole migration,7 whereas in RA axial migration is the most common pattern. If these subsets do represent distinct pathological categories, they may respond differently to corticosteroid injection; this question has not previously been studied.
The objectives of this prospective, open study were: (1) to evaluate the changes in pain, function, and range of movement after corticosteroid hip injection (CHI) under radiological guidance; (2) to determine which radiographic types of hip disease respond best.
Methods
PATIENTS
Forty five adult patients underwent CHI over a two year period. Eleven patients were recruited from the orthopaedic waiting list for hip replacement and 34 were referred from routine rheumatology clinics. Criteria for inclusion were: (1) hip pain for more than one month requiring regular analgesia, (2) pain on weight bearing and at night, (3) restriction of hip movement. Exclusion criteria comprised: (1) pregnancy, (2) Paget’s disease of hip or pelvis, (3) previous surgery or corticosteroid injection to the affected hip, (4) suspected sepsis of hip or surrounding tissues.
HIP INJECTION
All patients received an injection of 4 ml 1% lignocaine and 80 mg methylprednisolone (Depomedrone, Upjohn) into the synovial cavity of the affected hip. A 22G spinal needle was introduced under fluoroscopy by the anterior approach, and intra-articular position was confirmed by instillation of 2 ml of contrast medium (Ultravist 300) in all patients. All injections were performed by the same operator (AAB). Patients were returned to the ward by chair for four hours bed rest, before discharge in the early evening. They were not given any special instuctions thereafter and were allowed to resume usual activity. Local ethical committee approval was obtained before commencement of the study.
ASSESSMENT OF OUTCOME
Patients were assessed by the same physiotherapist for pain, functional ability, and range of movement (ROM). Assessments were made three hours before the injection (baseline) and after two, 12, and 26 weeks.
Pain was assessed by four 10 cm visual analogue scales (VAS) with reference to night pain, rest pain, weight bearing pain, and referred pain. These were summed to give a total pain score (max 40 cm). Pain relief at two weeks was calculated by subtracting the total pain score at two weeks from the baseline score.
Movement was measured by a goniometer in both hips for flexion, abduction, internal rotation, external rotation and extension; leg length was also determined.
Functional ability was estimated using a lower limb questionnaire (0–13 scale), graded according to walking distance. 1 = walk more than five miles. 3 = walk more than one mile. 5 = walk >100 yards. 7 = walk <100 yards (if walking stick required, add 1 mark.). 9 = walk upstairs. 11 = rise from chair. 13 = chairbound.
RADIOGRAPHY
Anteroposterior radiographs of the hip were taken at baseline and at 26 weeks. These radiographs were graded by one observer (MJP) with training in musculoskeletal radiology, and who was unaware of the primary diagnosis, clinical outcome or physiotherapy measurements. The joint space was measured in millimetres at the narrowest point. Overall grading of severity was made according to the scales of Kellgren and Lawrence12 for OA, and by Larsen’s method for RA.13 The pattern of bone response was described as being atrophic or hypertrophic or mixed.14 Cysts were estimated on a 0–3 scale in both the femoral head and the acetabulum15: 0 = none, 1= one or two small cysts, 2 = single large or multiple small, 3 = multiple large cysts. Other features graded on a 0 to 3 scale included joint space narrowing (JSN), osteophyte formation, and sclerosis.16
The pattern of migration of the femoral head was defined as superior, medial, axial or indeterminate.11 For analysis, medial and axial groups were combined and compared with the superior group; four radiographs in which the migration pattern could not be determined were excluded from the analysis.
Follow up x rays after six months were available on 39 patients. The paired films were blinded to order by covering the patient identification area and serial films were compared for radiological change.
STATISTICS
The study was analysed on an ‘intention to treat’ basis: for patients who withdrew before 26 weeks, their last measures were carried forward. Analyses were performed using the NCSS statistical software package (Number Cruncher Statistical System, version 5.01: Dr J L Hintze, Kaysville, Utah). Pain and function data were analysed by non-parametric methods, using Wilcoxon signed rank test and the Kruskal-Wallis test: measurements of range of movement were compared by paired t test. Reproducibility of grading of radiographs was tested by κ statistic, which compares the observed proportional agreement with the agreement that would have been expected by chance.
Results
PATIENT CHARACTERISTICS
Forty five patients (10 male:35 female) entered the study The underlying disease was RA in 15, OA in 27, and AS in three. Mean age was 59 years, range 21–79. A wide range of radiological abnormality was covered: minimum joint space width ranged from 0 mm to 5 mm (median 1 mm), Kellgren OA grade from 1 to 4 (median 3), and Larsen grade from 1 to 5 (median 3).
All 45 patients were assessed at baseline and at two weeks; 37 patients were reviewed at three months, and 30 at six months. Outcome was compared at the four time points using intention to treat analysis: for the 15 patients who withdrew early their last measurements were carried forward. Factors affecting response to CHI were investigated in the complete study group at the two week assessment.
Of the 15 study withdrawals, nine were lost because of hip surgery and six declined or failed to attend for follow up. The withdrawal group had higher baseline pain scores (29.8 v 26.3), but this was not statistically significant (p=0.22). The groups were similar for age, initial function, and radiographic severity. Hip movement tended to be more restricted in the withdrawal group, but this was only significant for flexion (61° v 78°; p=0.01), and internal rotation was actually slightly greater in the withdrawal group (21° v 16°). Median pain relief at two weeks was the same for study drop outs and completers (6.1 v 6.2), and so the patients who defaulted were not all non-responders.
OUTCOME
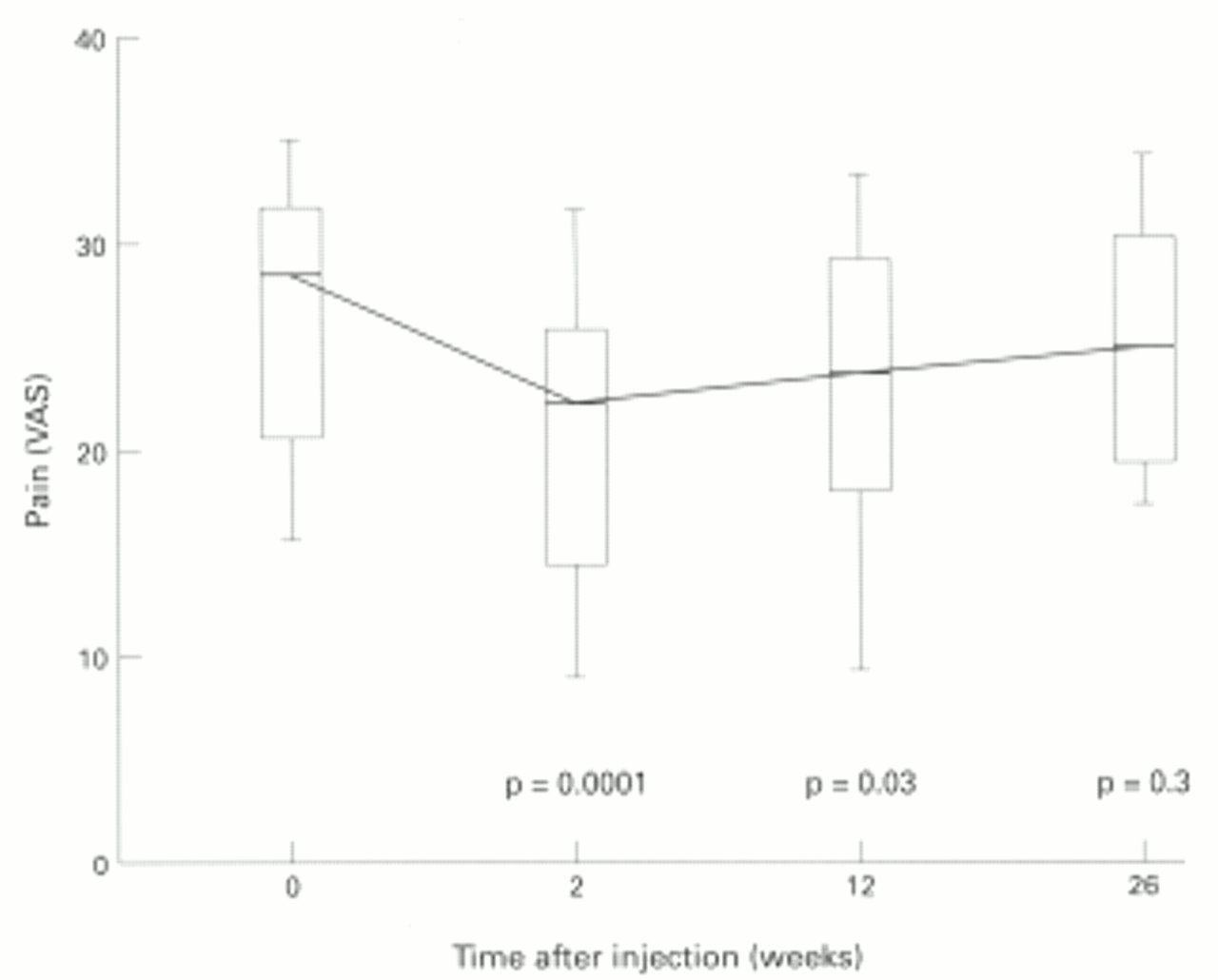
Median total pain score (max = 40 cm) decreased from 28.5 cm at baseline to 22.4 cm at two weeks, 23.8 cm at 12 weeks and had returned to near pre-injection values (24.9 cm) by 26 weeks (fig 1 and table 1). The improvement with respect to baseline was highly significant at two weeks (p=0.0001), and still significant at 12 weeks (p=0.03). Night pain, rest pain, referred pain, and weight bearing pain all improved, particularly night pain (table 1). These findings were not changed by restricting the analysis to the 30 patients who completed all study visits.

{kind=link}
Total hip pain after corticosteroid hip injection. Total hip pain by visual analogue scale (max = 40 cm) is shown in 30 patients followed up for six months after injection of 80 mg methylprednisolone under x ray guidance. The middle bar represents the median: the box represents the 25% and 75% quartiles: the whiskers represent the 10% and 90% centiles. p Values are for comparison with baseline pain scores (Wilcoxon signed rank test).
Pain and functional ability after corticosteroid hip injection
Nineteen patients achieved at least a 25% decrease in total pain score at two weeks; of this group 12 patients maintained 25% improvement to 12 weeks and five to 26 weeks. Median pain relief at two weeks in all 45 patients was similar for OA, RA, and AS patients (table2).
Pain relief after corticosteroid hip injection related to underlying disease and radiographic features
Functional ability showed no change (table 1). Internal rotation increased significantly from a mean of 17 degrees to 27 degrees at two weeks, but had fallen back to 23 degrees by 12 weeks (p=0.06) (table3). Other movements showed no change; there were no significant changes in ROM for the non-injected hip.
Range of movement after corticosteroid hip injection
RADIOGRAPHY
To determine if the radiological pattern of hip disease influenced the response to injection, the atrophic, hypertrophic, and mixed subtypes were compared in terms of the pain relief obtained at two weeks—total pain at 0 weeks minus pain at two weeks (table 2). Pain relief was significantly less in atrophic hips (median 0.9 cm) compared with mixed or hypertrophic ones (median 7.5 cm and 7.6 cm respectively). One possible statistical flaw of this analysis is that if atrophic hips tended to have less initial pain, they would be less able to demonstrate pronounced pain relief (regression towards the mean). However, the mean initial pain for atrophic hips was 26 cm compared with 29 cm for hypertrophic/mixed hips (p>0.6), making this unlikely to have an important impact.
The degree of radiological severity as judged by minimum joint space had no effect on pain relief after CHI (table 2); neither was there any significant difference in pain relief when analysis was made by Kellgren grade for the OA patient group (p=0.6) or by Larsen grade for the RA patients (p=0.2). The direction of migration of the femoral head did not seem to influence pain relief and nor did the degree of joint space narrowing, cysts or osteophyte formation.
Fifteen of 39 hips (38%) deteriorated radiographically at 26 weeks compared with baseline, although only five actually increased their Larsen or Kellgren grade. The hips that showed radiological worsening tended to have more severe initial disease; they had a narrower joint space (mean of 0.8 mm v 2.1 mm, p=0.01) and a worse overall grade (3.3 v 2.5 for OA hips by Kellgren and 3.4v 2.4 for Larsen RA hips, p=0.006). There was a tendency for atrophic hips and those with a superior migration pattern to progress more often, but this was not significant using the χ2 test with Yates’s correction (p=0.4 and p=0.11 respectively).
REPRODUCIBILITY OF RADIOGRAPHIC SCORING
Intraobserver reproducibility was tested on a subset of 19 hip radiographs that were still available to be rescored by the primary observer after an interval of 12 months. The observed proportional agreement (po) for the various radiographic features was: JSN 79% (κ=0.71), osteophyte 68% (κ=0.53), sclerosis 47% (κ=0.11), cysts 58% (κ=0.45), Kellgren grading 68% (κ=0.53), Larsen grading 47% (κ=0.28), direction of migration of femoral head 68% (κ=0.43). For the pattern of bone response, observed agreement was 79% and κ value was 0.65.
The intraobserver reproducibility data compare reasonably well with other reports,7 with the exception of sclerosis and Larsen grading. Sclerosis is a difficult feature to grade quantitatively. Most disagreements for the Larsen assessment involved grades 2 and 3, and all but one of the disagreements were within one grade of each other. However, in view of this finding, evaluation of radiographic severity was based on minimum joint space, which proved more reproducible than Kellgren or Larsen scales.
To further validate the grading of pattern of bone response, the 19 radiographs were reviewed by a musculoskeletal radiologist (JS) and the results compared with those of the primary observer (MJP): interobserver agreement, po, was 74% and κ 0.64. The disagreements were between mixed/hypertrophic grades in four cases and between atrophic/insufficient abnormality in the other case.
Discussion
Results from this open study of corticosteroid injection of the hip joint indicate that pain is improved significantly for approximately 12 weeks. The drift back to initial pain values was nearly complete by 26 weeks. Various aspects of hip pain improved, including referred, weight bearing, and rest pain, but night pain reduced the most. A sonographic study has shown that night pain correlates strongly with the presence of effusion in the hip.17
Hip injection was also associated with a temporary but notable increase in the degree of internal rotation. As internal rotation is the earliest sign of hip disease, this finding suggests a genuine effect on hip pathology, as opposed to a coincidental or placebo response. No increase in functional ability was found using our self report questionnaire, but in retrospect other more objective measures, such as the 50 yard walking time, may have been more sensitive.
To our knowledge only three studies of hip injection have been reported in the medical literature, and two of these used hydrocortisone, which is a comparatively short acting preparation. In a prospective study of hip injection in patients awaiting hip replacement, Flanagan et al 18 found little difference between saline or bupivicaine or bupivicaine with triamconolone. Between 58% and 75% of patients improved in all groups. However, this small trial was biased towards a negative result because patients were told that they would be given priority for surgery if their pain worsened after injection. An earlier paper in 1956 showed that hips treated with hydrocortisone and lidocaine do gain greater subjective improvement than with lidocaine alone.19In arecent retrospective analysis of 38 patients injected with hydrocortisone and lignocaine, hip pain improved after 69% of procedures for more than three months.20 However, these results should be interpreted with caution, as a major element of recall bias cannot be excluded.
Recent data have suggested that immobilisation for 24 hours after injection of weight bearing joints confers a more longlasting effect.21 In our study patients were rested in bed for four hours; it is possible that a longer period of bed rest might further improve the efficacy.
A control group treated by placebo injection was not included in this study as it was felt to be unethical because the patients all had severe symptoms not responding to maximal analgesia. We would accept that part of the improvement shown could have been a placebo effect, and so the results should be interpreted with caution while awaiting randomised comparative studies. However, the primary objective of this study was to discover if the radiographic pattern of arthritis had any effect upon response to CHI. Indeed, the pattern of bone response was found to be an important factor in response to injection and it proved a reliable measure both within and between observers. Atrophic hips did not gain any significant benefit compared with hips with a hypertrophic or a mixed bone response. Consequently, patients with atrophic disease should perhaps be considered for arthroplastic surgery rather than for corticosteroid injection. This interesting finding may be explained by either atrophic disease being less inflammatory and hence less corticosteroid responsive, or alternatively corticosteroid may actually worsen bone resorption in these hips—this has been reported as a possible adverse effect of such injections.22
The radiographic severity of the hip arthritis did not have an important influence on response to CHI. Severity was graded by minimum joint space as well as by Kellgren and Larsen scales as the former proved to be a more reproducible measure. It is also noteworthy that patients with RA and OA responded equally well. In contrast with our results, other workers have found greater improvement in RA than OA, both in the hip20 and the knee.22 This might be explained by the fact that, in this study, atrophic disease was more common in RA patients (six of 15) compared with OA patients (six of 27).
Predictive factors for response to intra-articular corticosteroid have not previously been investigated for the hip joint. Two recent studies have attempted to identify such factors in the osteoarthritic knee.23 ,24 Gaffney et al found increased benefit in patients with evidence of joint effusion, but radiographic severity did not seem to be important.23 Conversely, Joneset al were unable to identify any clinical predictors, although radiographic parameters were not investigated. In both studies improvement over placebo was seen in the short-term (1–3 weeks) but not over the medium term (6–8 weeks).
In this study, 15 of 39 (38%) of hips showed radiological worsening after six months. Although this rate may seem high it should be remembered that serial films were compared for any small degree of change and the percentage showing a discrete change in Kellgren or Larsen grade was less (12%). The hips showing radiographic progression had significantly more severe initial disease with more subchondral cysts and greater JSN. Atrophic and superior migration pattern hips tended to progress more often but this was not statistically significant because of the small numbers in each group; however, these findings are in keeping with other studies.8
In our experience accurate intra-articular hip injection requiresx ray screening as surface landmarks are unreliable. The procedure was well tolerated by the patients and the technique was easily learnt by the operator; up to three patients could be treated in one hour of x ray time. Radiological exposure is minimal with an average screening time of 30–60 seconds. There are several clinical situations in which CHI may be particularly useful: (1) when surgery is contraindicated because of coexisting medical conditions, (2) in young patients when there is concern over the potential longevity of a hip prosthesis, (3) as a diagnostic trial to confirm the hip as the source of pain, (4) patients awaiting hip replacement who might benefit not only from temporary amelioration of symptoms but also reduction in the need for potentially toxic non-steroidal anti-inflammatory treatment.
In conclusion, this open study suggests that CHI can improve pain and internal rotation for up to 12 weeks in both inflammatory arthritis and osteoarthritis. However, response is negligible in atrophic hips compared with those with a hypertrophic or mixed bone response. We feel that CHI offers a further therapeutic option for hip arthritis in those patients whose radiological pattern is not purely atrophic.
Acknowledgments
We should like to thank Dr T E Hothersall and Dr M F Shadforth for referring their patients, and the Haywood Foundation, which funded Dr A A Borg and Ms K Dziedzic. Upjohn Pharmaceuticals Ltd kindly supplied Depomedrone.