Article Text

Abstract
Objective To examine the association of biologic therapy use for psoriasis with incident psoriatic arthritis (PsA) diagnosis.
Methods A retrospective cohort study was conducted in the OptumInsights Electronic Health Record Database between 2006 and 2017 among patients with psoriasis between the ages of 16 and 90 initiating a therapy for psoriasis (oral, biologic or phototherapy). The incidence of PsA was calculated within each therapy group. Multivariable Cox models were used to calculate the HR for biologic versus oral or phototherapy using biologics as a time-varying exposure and next in a propensity score-matched cohort.
Results Among 1 93 709 patients with psoriasis without PsA, 14 569 biologic and 20 321 cumulative oral therapy and phototherapy initiations were identified. Mean age was lower among biologic initiators compared with oral/phototherapy initiators (45.9 vs 49.8). The incidence of PsA regardless of therapy exposure was 9.75 per 1000 person-years compared with 77.26 among biologic users, 61.99 among oral therapy users, 26.11 among phototherapy users and 5.85 among those without a prescription for one of the target therapies. Using a multivariable adjustment approach with time-varying exposure, adjusted HR (95% CI) for biologic users was 4.48 (4.23 to 4.75) compared with oral or phototherapy users. After propensity score matching, the HR (95% CI) was 2.14 (2.00 to 2.28).
Conclusions In this retrospective cohort study, biologic use was associated with the development of PsA among patients with psoriasis. This may be related to confounding by indication and protopathic bias. Prospective studies are needed to address this important question.
- psoriatic arthritis
- epidemiology
- outcome assessment
- health care
- biological therapy
Data availability statement
Data may be obtained from a third party and are not publicly available. Optum EHR data and Optum administrative claims data are available from Optum for a cost. The authors will share code lists and stata do files with those who have an interest.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Psoriasis often precedes psoriatic arthritis (PsA) development; treating psoriasis with biologic therapies reduces subclinical joint inflammation and may help to prevent or slow PsA development. Recently published studies in selected cohorts seem to support this concept.
What does this study add?
Contrary to the study hypothesis, patients with psoriasis using biologic therapies were more likely to develop PsA. This may be related to confounding by indication or protopathic bias.
How might this impact on clinical practice or future developments?
Prospective clinical trials are needed to address whether biologic therapies can mitigate or modify the risk for PsA among patients with psoriasis.
Introduction
Psoriasis is a chronic immune-mediated skin disease that affects approximately 2% of US adults. Up to 10%–30% of patients with psoriasis will develop psoriatic arthritis (PsA), a chronic inflammatory musculoskeletal disease, at some point during the course of the disease.1 Despite treatment advances, patients with PsA still experience significant morbidity, functional disability, increased healthcare costs and diminished quality of life and less than half of patients achieve minimal disease activity in clinical practice.2–5 Earlier diagnosis and treatment initiation could improve therapeutic response, but there often remains a delay in diagnosis.6 7
Psoriasis remains one of the strongest known risk factors for the development of PsA.8 As the severity of psoriasis increases, the prevalence and incidence of PsA also increase.9–12 Given the shared pathogenetic pathways (tumour necrosis factor (TNF), IL-17), one would expect the treatment of psoriasis to be associated with reduced progression to clinically overt PsA.8 13–17 Furthermore, biologics, such as TNF alpha inhibitors, IL17i, 12/23i and IL23i, have demonstrated a clear benefit in improving the signs and symptoms of both psoriasis and PsA.18–23 However, the relationship between a treatment for psoriasis and resulting PsA may be confusing in that some biologic therapies and retinoids have been purported to result in altered stimulation of the immune system, which has led to the paradoxical onset of PsA or the onset of pustular psoriasis among TNF inhibitor (TNFi) users.20 24
Studies addressing the impact of therapy for psoriasis on development of PsA are lacking. Few sufficiently large cohort studies, and no population-based studies, have addressed the impact of biologic therapy on development of PsA, and no prospective studies have been published. One of the greatest challenges in examining the impact of treatment for psoriasis on the development of PsA is confounding by indication, the concept that an individual receives a therapy for a reason (eg, severe psoriasis).25 For example, patients with more severe psoriasis are more likely to receive systemic therapy for psoriasis and are also at an increased risk for PsA.8 Additionally, ‘protopathic bias’, a situation in which treatment is prescribed because of a symptom or an undiagnosed disease that is also the outcome of interest, may be at play and could induce an apparent association between therapy and the development of the disease of interest.26 Finally, confounding by prognosis describes the phenomenon in which clinicians prescribe more aggressive therapy when the outlook is poor, as is the case with severe psoriasis.27 Together, these biases challenge the validity of results from retrospective cohort studies addressing this important question.
In this study, we aimed to examine the impact of biologic therapies on the development of PsA and to examine the potential role of these biases on the results. We used data from an electronic health record (EHR) database obtained from OptumInsights. We hypothesise that, theoretically, patients receiving a biologic therapy for psoriasis should be less likely to develop PsA than those receiving a non-biologic therapy for psoriasis. The alternative hypothesis is that biologic use is either not associated with or positively associated with development of PsA.
Methods
Study design
A retrospective cohort study was performed within the OptumInsights EHR Database (USA) between 2006 and 2017.
Data source
The OptumInsights EHR database is a longitudinal EHR repository derived from dozens of healthcare organisations in the USA including more than 150 000 providers, 2000 hospitals and 7000 clinics. Data captured include demographics, medications prescribed and administered and coded diagnoses and procedures.28 In a sensitivity analysis, we repeated the analyses in the OptumInsights Administrative Database. The administrative database contains claims data from over 85 million patients in the USA and between 15 and 20 million patients annually.
Patients
Patients with two or more International Classification of Diseases (ICD) codes for psoriasis who were aged 16–90 were identified. For cohort entry, patients were required to have at least 12 months in the dataset prior to the first code for psoriasis.
Exposures
The primary exposure of interest was biologic therapy (adalimumab, alefacept, brodalumab, certolizumab, etanercapt, golimumab, guselkumab, infliximab, ixekizumab, secukinumab, ustekinumab) compared with non-biologic systemic oral therapy (acitretin apremilast, cyclosporine, etretinate, methotrexate) or phototherapy. Because it remains unclear how long exposure to a given medication could affect the patient, we used a ‘once exposed, always exposed’ approach in the primary analysis. In other words, once a patient was exposed to a biologic therapy, they did not transition back to the ‘oral therapy’ group.
Outcome
The outcome was PsA defined by a single ICD code. A single code for PsA in the setting of psoriasis and a relevant therapy has a high positive predictive value.29 In a sensitivity analysis, we required two codes for PsA.
Time
The risk window over which the outcome was assessed varied by analysis (shown in online supplemental figure S1). In the time-varying exposure analysis, the outcome could occur at any point after diagnosis of psoriasis. In the propensity score (PS)-adjusted models, the outcome could occur any time after initiation of therapy.
Supplemental material
Covariates
Covariates at baseline were determined in the 12 months prior to therapy initiation. The incidence of PsA was described overall and within each therapy group. Comorbidities were also identified using ICD codes. The code list was developed by two coders independently and reconciled.
Statistical analysis
Incidence was calculated among each of the key subgroups: all patients, those initiating oral therapy, phototherapy or biologic therapy (as well as subgroups including TNFi, IL12/23i and IL17i) from initiation of therapy to end of follow-up or development of PsA. We also examined incidence while on therapy (ending at end of therapy plus 90 days). We then compared incidence of PsA between patients on biologic therapy versus those not on biologic therapy and versus those initiating oral and/or phototherapy and censoring at switch to biologic therapy. The following models were used: (1) a multivariable Cox model using a time-varying exposure where the exposure was biologic initiation (once patients were exposed to a biologic, they were considered always exposed) adjusted for covariates selected using purposeful selection30 and (2) after excluding patients with a prior history of biologic and/or oral therapy use, PS matching between patients initiating biologic therapy and oral or phototherapy. In the PS-matching analysis, the date of initiation of biologic therapy or oral or phototherapy, respectively, was the start date. PS was developed at therapy initiation using the age, sex, psoriasis duration and comorbidities and conditions (see online supplemental methods 1). Patients were matched 1:1 using a greedy-matching algorithm with calliper 0.1. Overlap of the PS and balance of covariates were checked to ensure adequate matching (online supplemental figure S2A and online supplemental figure S2B). Sensitivity analyses are described in the online supplemental methods 1. All statistical analyses were performed within Stata software, V.16.0 (College Station, Texas, USA).
Ethics approval and patient involvement
This study was considered exempt by the University of Pennsylvania Institutional Review Board. Patients were not involved in designing or analysing this study.
Results
Among 1 93 709 patients with psoriasis without PsA at baseline, 34 890 initiated phototherapy, oral therapy or biologic therapy during follow-up. In the cohort, there were 14 569 new biologic initiations and 20 321 cumulative oral therapy and phototherapy initiations. The mean age was slightly lower in the biologics group compared with the oral/phototherapy group (45.9 vs 49.8). The proportion of women was slightly lower among biologic users (51.8% vs 57.0%), and there was a similar proportion of Caucasians (85.8% vs 85.8%) in each group (Table 1). Observation time was similar across both groups (2.6 years in the biologic therapy group and 2.5 years in the oral systemic therapy or phototherapy group). Among those with a new prescription for a new biologic therapy, 10% had a history of prior biologic therapy, 8% had a history of prior oral systemic therapy and 2% had a history of prior phototherapy at any point in the past. Among those initiating a new oral therapy, 4% had a history of prior biologic therapy, 3% had a history of prior oral systemic therapy and 1% had a history of prior phototherapy.
Baseline characteristics of patients with psoriasis who initiated therapy
Among all patients, regardless of therapy exposure, the incidence of PsA was 9.8 per 1000 person years (table 2). The incidence was lower among those who did not receive therapy during follow-up (5.9 per 1000 person-years). Patients who received phototherapy also had a relatively low incidence of PsA, particularly when censoring patients at the start of either oral or biologic therapy. Patients who initiated biologic therapies or oral therapies for psoriasis had a substantially higher incidence of PsA (77.3 cases per 1000 person-years and 62.0 cases per 1000 person-years, respectively). Among patients who received oral therapy who were censored at initiation of a biologic therapy, the incidence was much lower (58.5 per 1000 person-years). The incidence decreased by increasing line of therapy and among those on a single biologic therapy for at least 5 years (37.3 per 1000 person-years) (online supplemental table S1).
Incidence of PsA by therapy initiated
To examine whether the incidence of PsA differed between patients using biologic therapy and those using oral therapy or phototherapy (after adjusting for potential confounders), we constructed two different types of models: (a) traditional Cox proportional hazards multivariable-adjusted model with a time-varying exposure and separately (b) Cox proportional hazards models starting time at therapy initiation and in a PS-matched cohort. The unadjusted Kaplan-Meier (KM) curves are shown in figure 1A,B and the KM curves for each of the individual biologics are shown in figure 1C. In a model in which biologics are a time-varying exposure compared with no biologic therapy (including patients who have received oral therapy, phototherapy or no therapy), receiving biologic therapies was associated with a higher incidence of PsA (HR 4.84, 95% CI 4.64 to 5.05). The results are similar, though more attenuated, when restricting the cohort to patients who have received either a biologic, an oral therapy, or a phototherapy (HR 4.48, 95% CI 4.23 to 4.75). When time is started at first biologic therapy, the results are further attenuated though similar whether using multivariable adjustment (2.14, 95% CI 2.00 to 2.28) or PS matching (HR 2.17, 95% CI 2.03 to 2.33) (table 3). In examining time from therapy start to diagnosis of PsA, many patients who developed PsA did so shortly after biologic or oral therapy initiation (figure 2). In contrast, diagnosis of PsA occurred more evenly over time in patients receiving phototherapy or no therapy prescriptions.

Kaplan-Meier curves for development of psoriatic arthritis. Kaplan-Meier curves for two separate analyses: (A) In the time-varying covariate analysis, we examined patients with psoriasis who initiated a biologic versus no therapy. In this case, time is started at first diagnosis of psoriasis (n=199 204); (B) In the propensity score analyses, time begins at the new initiators of therapy (biologic vs oral vs phototherapy) (n=29 612); (C) Finally, we examined time to diagnosis by individual biologic subclass (N=29 612).
Primary multivariable models

Timing of PsA diagnosis by therapy start. Among patients who receive a new diagnosis of PsA, we examined the time to new PsA diagnosis. Time represents the time from start in the study: initiation of the specified therapy or 1 year after psoriasis diagnosis for those who do not receive therapy. PsA, psoriatic arthritis.
Sensitivity analyses resulted in very similar results, including when patients who developed PsA within the first year after biologic use in the PS model were excluded (online supplemental table S2). Additionally, results were also similar, although the HR attenuated, when run within the administrative data set (online supplemental table S2).
Discussion
PsA is a chronic inflammatory disease that currently has suboptimal clinical outcomes with at least 50% of patients achieving remission by any definition. One strategy for improving outcomes in PsA is to treat psoriasis more aggressively with the goal of preventing the onset of clinically overt PsA. Some proof-of-concept studies have demonstrated that treatment with biologics reduces subclinical joint and enthesial inflammation in patients with psoriasis.31 32 This would suggest that treating patients with biologics could potentially prevent PsA. Our study sought to examine whether treatment with a biologic agent among patients with psoriasis has an impact on the development of PsA. Several approaches were used to address this question, but the key outcome was that patients on biologics seemed to have a higher incidence of PsA than patients on oral or phototherapy. We do not suggest that these results should be interpreted causally; in other words, biologics likely do not cause PsA. On the contrary, there are several biases that may play a role in this finding, suggesting that caution should be used in interpreting observational studies that study the impact of biologic therapy on the development of PsA.
Two recent publications in this journal and one in another journal have addressed this topic in selected dermatology clinic-based populations (as opposed to the population-based cohorts studied here).33–35 One demonstrated a similar HR to our PS analysis in their PS analysis comparing biologics to phototherapy (HR 2.07, 95% CI 0.87 to 4.93). In contrast, their primary analysis34 and the analyses in a second and third study33 35 found a decreased incidence of PsA in the biologics cohort compared with phototherapy and no therapy. Why are the results different within studies and between these studies and our study? This may in part be related to the patient population studied. The other two studies were based in dermatology populations with dermatology–rheumatology collaborations. This is a small subset of the population observed in the current study, and the opposing results may be the result of collider stratification bias where the collider is being seen in a dermatology–rheumatology centre.36 Additionally, Gisondi et al required the patients studied to be on therapy for at least 5 years, essentially excluding these patients that developed PsA in the first 5 years. After we restricted the biologics cohort to that described in Gisondi et al, the incidence in this subgroup was reduced to approximately half the incidence when this restriction was not applied and was lower than the incidence in the oral therapy group. Thus, selection bias may be contributing to the differential results; the population observed is important to consider in interpreting the results of any of these retrospective studies, including this study. The only prospective cohort study of psoriasis and the risk for PsA, a Toronto-based cohort, found that patients with psoriasis using a TNFi had a higher risk of PsA than those who did not use a TNFi, although the results were not statistically significant (HR 1.56, 95% CI 0.19 to 12.6).37 This was likely related to the relatively small number of patients on a TNFi in that study.
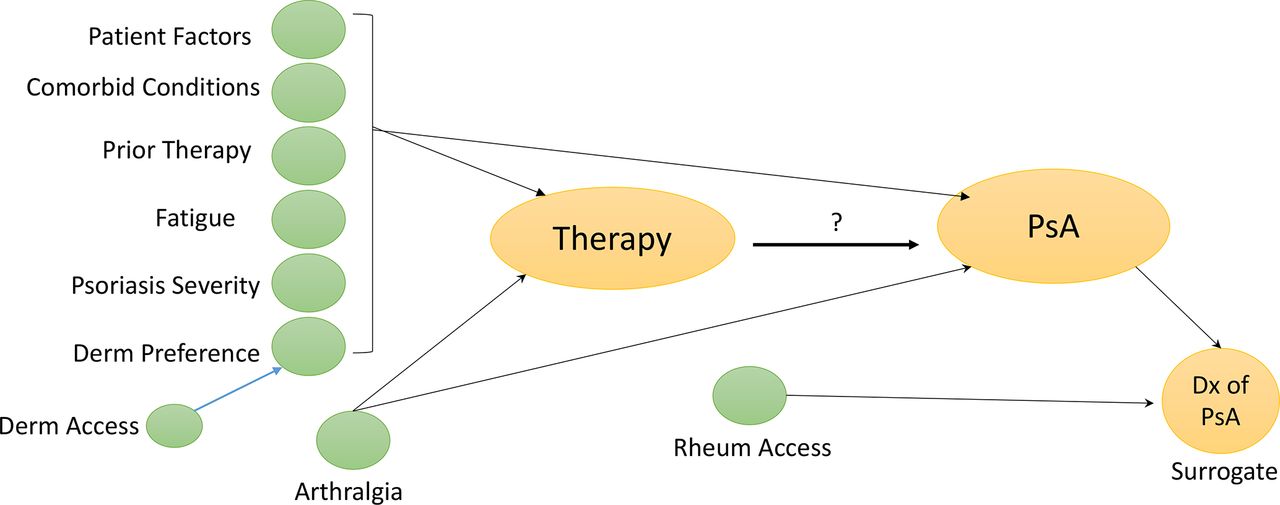
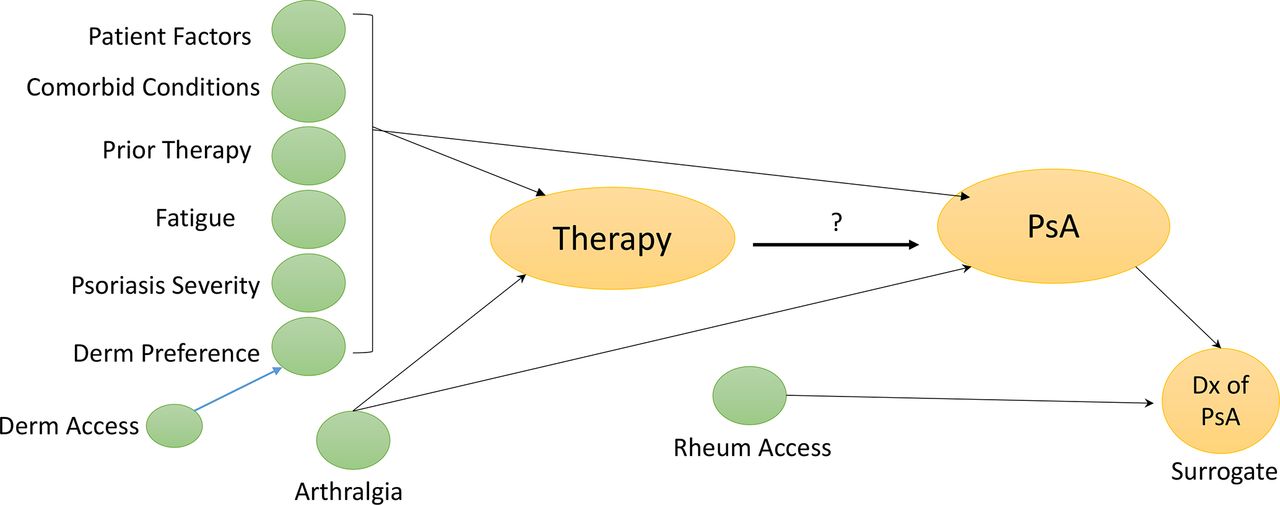
Several biases may contribute to the results of retrospective studies. First, selection of a therapy for a given patient is motivated by many factors (see figure 3); this is known as confounding by indication. Most of the factors that influence therapy selection (ie, a patient’s risk tolerance) are not measured in any of the three studies and thus are potential unmeasured confounders. PS-matching and marginal structural models are two strategies for addressing confounding by indication, but these cannot be causally interpreted if important confounders, particularly those that may be differential between the exposure groups, are not measured.25 38 39 Next, in an extension of confounding by indication, patients may be prescribed a biologic because there is either a perceived increased risk for PsA or symptoms that may suggest early PsA. This is known as protopathic bias. For example, a dermatologist may see a patient with psoriasis who complains of joint issues and the dermatologist switches the patient to a biologic (believing the patient may have PsA). When a rheumatologist then sees the patient, the rheumatologist may code for PsA. This was evident in our study as a large number of the incident PsA diagnoses occurred shortly after initiation of the biologic therapy. In another recent study, we observed that dermatologists rarely coded for musculoskeletal complaints, suggesting that misclassification of the outcome may be particularly problematic in this context.40 In the current study, a sensitivity analysis suggested that while protopathic bias seems to be playing a role (ie, there is a considerable number of diagnoses of PsA within the first year of biologic treatment), the increased risk of PsA with biologic use seemed to persist throughout the first 5 years. Next, survival bias may be playing a role in these results. In other words, a patient has to ‘survive’ without PsA to receive a biologic therapy and they are, thus, closer to the development of PsA if they are going to develop it, enhancing the observed risk of PsA in the biologic group. To address this concern, we adjusted for duration of disease and we performed an additional analysis within the PS-matched cohort to address the concern for survival bias and these did not meaningfully change the HR.
{kind=link}
{kind=link}
{kind=link}
Directed acyclic graph: potential confounders in studying biologic therapies and the risk for PsA. Directed acyclic graphs are a graphical method of displaying relationships between variables. Shown here are the potential confounders in the relationship between therapy prescription and diagnosis of PsA, many of which are unmeasured in EHR and administrative datasets. EHR, electronic health records; PsA, psoriatic arthritis.
Besides the biases that may lead to seeing a higher incidence of PsA among biologic users, is it possible that biologics due in fact stimulate development of PsA? Some have theorised that paradoxical reactions may be the result of shifting polarisation of T cell responses, leading to inflammation in alternate tissues (ie, development of palmoplantar pustular psoriasis with TNFi and eczematous reactions with IL17i).41 Alternatively, other theories include disruption of negative feedback loops, secondary effects of antidrug immune response (ie, drug-induced lupus erythematosus with TNFi) or non-specific interactions with Fc receptors leading to activation of innate immunity.41 Unlike skin-related paradoxical reactions and development of new inflammatory bowel disease, development of de novo inflammatory arthritis with biologic therapies among patients with psoriasis has not been commonly reported beyond drug-induced lupus.42 Thus, while a paradoxical reaction may explain some of these cases, we believe that the more likely explanation is the epidemiologic phenomena described above.
This study should be interpreted in light of limitations. EHR data were used in this study as the primary data source. Health systems in the US function as open systems in that patients may be seen in one system for their psoriasis and also seen in another system by their primary care physician. This leads to a situation where not all codes are captured in one system. We addressed this concern in two ways. First, by restricting the study to the subpopulation of patients with a primary care physician in the system. Second, when the analyses were repeated within an administrative data set, there were no substantial differences in the results. In addition, reliance on codes as a surrogate for psoriasis and PsA diagnosis may be associated with misclassification.29 The results were similar when using one and two codes for PsA, and that the use of a therapy for psoriasis makes the likelihood of truly having psoriasis or PsA much higher.29 Misclassification may influence the results of this study.43 If misclassification is balanced between the biologic and oral therapy initiators, known as non-differential misclassification, the results would bias toward the null.44 The misclassification would not lead to excessive type I error but would lead to reduced statistical power in identification of risk factors that are associated with PsA.45 However, it is possible that there is more misclassification in the biologic group given the larger number of new diagnoses after therapy, which could lead to excessive false-positive findings (ie, inflation of type I error).46 Given the large number of patients, we are unable to examine these patients. Use of patient-reported outcomes or physician examination could have improved our understanding of the timing and reasons for therapy prescriptions, but unfortunately this was not available. Next, in an EHR, medications may have been prescribed but never filled. To address this limitation, we used two prescriptions for a given therapy (suggesting a refill was initiated) as the primary analysis. We also repeated the analyses in the administrative data set where the prescriptions were dispensed and the results were similar. Finally, mortality was not addressed as a competing risk in the development of PsA because we did not have data on mortality. Given that this is a relatively young and healthy patient population overall, we believe that this would not have a significant impact on the results.
There remains much to learn about the development of PsA including the best methods for studying whether interventions, such as biologic use or weight loss, may have an impact on disease prevention.47 48 Ongoing efforts seek to define the stages of PsA development,49 to understand the predictors of PsA development among patients with psoriasis47 and to identify the pathophysiologic and imaging features that may signal development of PsA.50–52 While retrospective observational studies offer several advantages, questions of therapeutic effectiveness for preventing PsA may not be ideally addressed in these data sets. While EHR data sets capture coding as it happens in the real world, the development of PsA can be insidious, subtle and challenging to recognise, particularly when assessing PsA development retrospectively. It is important to consider the population analysed; selection bias (ie, only selecting patients with moderate to severe psoriasis or those that have been continuously on therapy for several years), and resulting collider stratification bias can result in very different estimates and should be considered in all study designs. Prospective observational studies are needed to study the pathophysiology of PsA development. In addition, randomised controlled trials that remove confounding by indication are needed to better understand the effect of therapy for psoriasis on the prevention, or delayed development, of PsA.
In summary, in this retrospective cohort study, patients with psoriasis initiating biologic therapy were more likely to develop PsA than patients initiating phototherapy or oral therapies or those not receiving therapy. Caution should be used in interpreting retrospective studies of the impact of biologic therapy on development of PsA. Future randomised controlled trials with long-term follow-up are needed to address the impact of therapy for psoriasis on the prevention of and/or the delay in development of PsA.
Data availability statement
Data may be obtained from a third party and are not publicly available. Optum EHR data and Optum administrative claims data are available from Optum for a cost. The authors will share code lists and stata do files with those who have an interest.
Ethics statements
Patient consent for publication
Acknowledgments
We thank Tori Fischer for assistance in medical editing and administrative assistance.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Josef S Smolen
EM and JFM contributed equally.
Contributors Study concept and planning: JFM, TJL, HC, JUS, CTR, JMG, AO. Analysis: RF, DS, YC, SX, AO. Interpretation: all. Wrote first draft: EM. Revised draft and edited: all.
Funding AO and RF received funding from National Psoriasis Foundation.
Competing interests No commercial entities provided support for the work in the submitted manuscript. Dr. Gelfand served as a consultant for Abcentra, Abbvie, BMS, Boehringer Ingelheim, Cara (DSMB), GSK, Lilly (DMC), Janssen Biologics, Novartis Corp, UCB (DSMB and Mindera Dx, receiving honoraria; and receives research grants (to the Trustees of the University of Pennsylvania) from Abbvie, Boehringer Ingelheim, Janssen, Novartis Corp, Celgene, Ortho Dermatologics, and Pfizer Inc; Dr Gelfand is a Deputy Editor for the Journal of Investigative Dermatology receiving honoraria from the Society for Investigative Dermatology, is Chief Medical Editor for Healio Psoriatic Disease (receiving honoraria) and is a member of the Board of Directors for the International Psoriasis Council, receiving no honoraria. Thorvardur Love has received reimbursement from Celgene for speaking about guidelines for the treatment of psoriatic arthritis. Alexis Ogdie has served as a consultant for Abbvie, Amgen, BMS, Celgene, Corrona, Global Health Living Foundation, Janssen, Lilly, Novartis, Pfizer, and Takeda and has received grants to the University of Pennsylvania from Pfizer and Novartis and to Forward from Amgen. Her husband has received royalties from Novartis. The remaining authors have no COI to report.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.