Article Text

Abstract
Objectives Meniscal tears have been linked to knee osteoarthritis progression, presumably by impaired load attenuation. How meniscal tears affect osteoarthritis is unclear; subregional examination may help to elucidate whether the impact is local. This study examined the association between a tear within a specific meniscal segment and subsequent 2-year cartilage loss in subregions that the torn segment overlies.
Methods Participants with knee osteoarthritis underwent bilateral knee MRI at baseline and 2 years. Mean cartilage thickness within each subregion was quantified. Logistic regression with generalised estimating equations were used to analyse the relationship between baseline meniscal tear in each segment and baseline to 2-year cartilage loss in each subregion, adjusting for age, gender, body mass index, tear in the other two segments and extrusion.
Results 261 knees were studied in 159 individuals. Medial meniscal body tear was associated with cartilage loss in external subregions and in central and anterior tibial subregions, and posterior horn tear specifically with posterior tibial subregion loss; these relationships were independent of tears in the other segments and persisted in tibial subregions after adjustment for extrusion. Lateral meniscal body and posterior horn tear were also associated with cartilage loss in underlying subregions but not after adjustment for extrusion. Cartilage loss in the internal subregions, not covered by the menisci, was not associated with meniscal tear in any segment.
Conclusion These results suggest that the detrimental effect of meniscal tears is not spatially uniform across the tibial and femoral cartilage surfaces and that some of the effect is experienced locally.
Statistics from Altmetric.com
The primary functions of the meniscus are load distribution and shock absorption.1,–,4 The meniscus provides stability by improving surface congruency and may aid in proprioception and lubrication.5,–,8 Meniscal damage or resection impairs these functions and subjects articular cartilage to focal axial and aberrant shear stresses; there is evidence of focal stress increase even after partial meniscectomy.9 10 Detrimental effects of meniscal lesions on cartilage may not be uniform across the joint surfaces, especially as some of the surface is not covered by the semicircular menisci.
In theory, the tibiofemoral cartilage subregions that the meniscus overlies may be exposed to greater load when that meniscal segment is damaged. It is not clear if meniscal lesions have a local impact, that is, specifically, whether a lesion within a meniscal segment (anterior horn, body or posterior horn) is associated with greater loss in the underlying cartilage subregion. Meniscal extrusion, a condition in which partial or full meniscal displacement uncovers the cartilage, represents another meniscal pathology that may coexist with meniscal tears in knee osteoarthritis.11,–,13 It is important to examine whether any specific meniscal tear effect on subregional cartilage loss is explained by concomitant meniscal extrusion.
Previous studies have demonstrated a relationship between meniscal lesions and the development14 and progression15,–,18 of knee osteoarthritis. Early reports describe some effort to explore the meniscal lesion/cartilage loss relationship at a subregional level.19,–,22 A meniscal lesion effect at the articular cartilage subregion(s) that the lesion overlies will add support to a local, protective role of the meniscus in cartilage integrity and to continued efforts on strategies to preserve meniscal tissue in osteoarthritic knees.
The purpose of this study was to examine the role of meniscal tears at baseline in subsequent cartilage loss in tibial and femoral subregions in individuals with knee osteoarthritis. We tested two hypotheses:
A tear in each medial meniscal segment at baseline is associated with articular cartilage thickness loss in the subsequent 2 years within the same medial subregions as the torn segment.
A tear in each lateral meniscal segment at baseline is associated with cartilage loss in the subsequent 2 years within the same lateral subregions as the torn segment.
Methods
Sample
Study participants are from a knee osteoarthritis natural history study, the Mechanical Factors in Arthritis of the Knee Study 2 (MAK-2) and were community-recruited through advertising, neighbourhood organisations, the Buehler Center on Aging, Health and Society registry at Northwestern University and medical centre referrals.
Inclusion criteria were: definite tibiofemoral osteophytes (Kellgren/Lawrence (K/L)23 ≥2) in one or both knees; and ‘a little difficulty’ or more than a little difficulty for two or more items in the WOMAC physical function scale.24 Exclusion criteria were: corticosteroid injection within 3 months; avascular necrosis, rheumatoid or other inflammatory arthritis, periarticular fracture, Paget's disease, villonodular synovitis, joint infection, ochronosis, neuropathic arthropathy, acromegaly, haemachromatosis, gout, pseudogout, osteopetrosis, meniscectomy; or exclusion criteria for MRI, for example, pacemaker, artificial heart valve, aneurysm clip or shunt, metallic stent, implanted device or orbital metallic fragment.
Approval was obtained from the Office for the Protection of Research Subjects of Northwestern University and Evanston Northwestern Healthcare; all participants gave written consent.
MRI acquisition
All participants had bilateral knee MRI at baseline and 2 years later using a commercial knee coil and 1.5 or 3.0 T (only 15 participants) whole-body scanners (GE Healthcare, Waukesha, Wisconsin, USA); previous work revealed no systematic offset and very high measurement correlation between these field strengths.25 Each knee was scanned and re-scanned on the same machine with the same protocol at the two time points.
Quantitative tibial and femoral cartilage thickness measurement was obtained from double-oblique coronal T1-weighted three-dimensional spoiled gradient-echo images with water excitation. Meniscal parameter grading utilised coronal T1-weighted spin-echo and sagittal fat-suppressed dual-echo turbo spin-echo sequences.
The 1.5 T parameters are shown in table 1; the 3.0 T parameters are shown in table 2.
Acquisition parameters, 1.5T MRI
Acquisition parameters, 3.0T MRI
Assessment of meniscal tears and extrusion
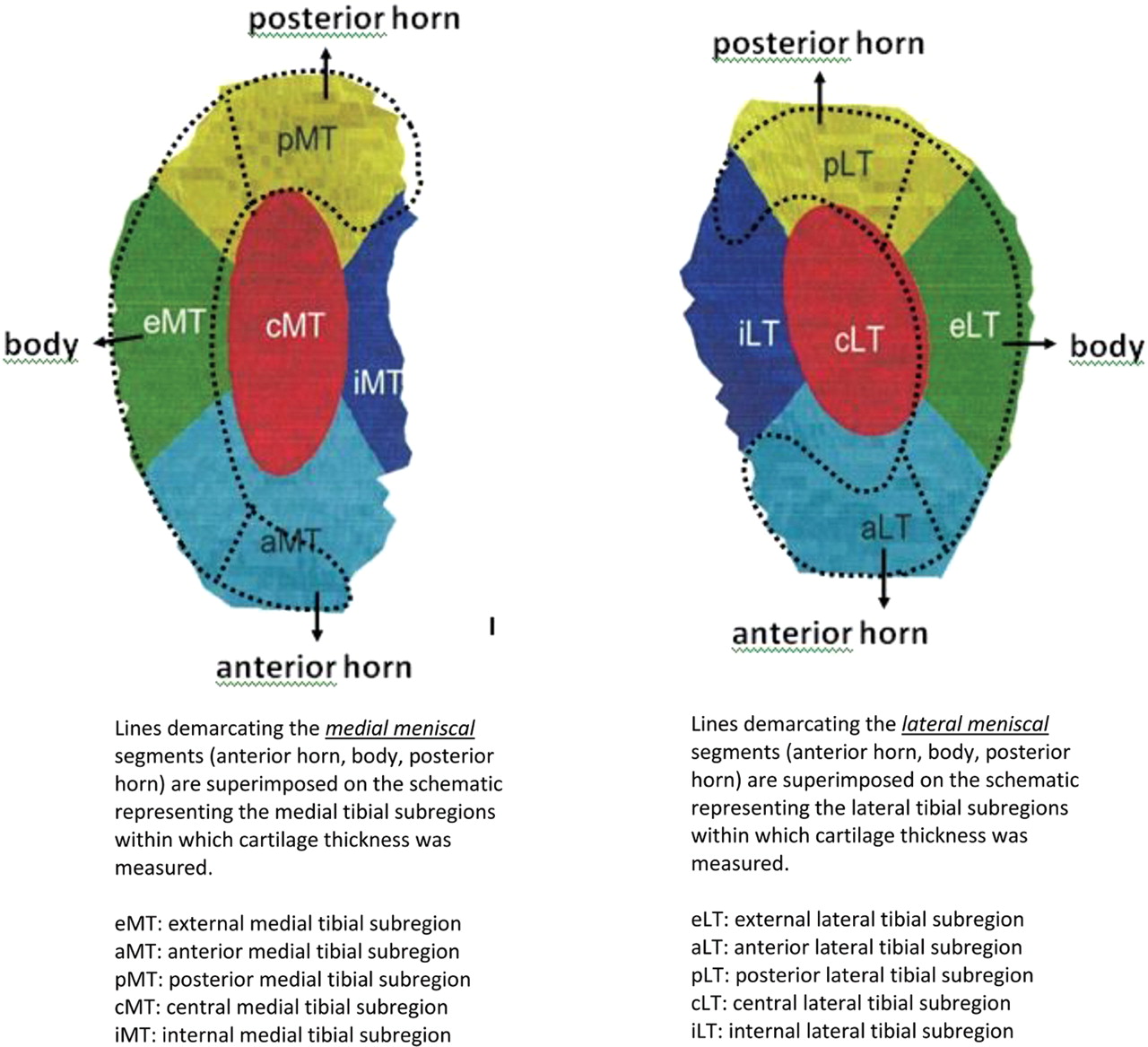
Each segment (anterior horn, body, posterior horn) of each meniscus was graded separately for tears, using the whole-organ magnetic resonance imaging score (WORMS) system,26 (0, intact; 1, minor radial or parrot-beak tear; 2, non-displaced tear; 3, displaced tear or partial maceration; and 4, complete maceration and destruction), with tear defined as grade 2 or more to maximise test specificity. Figure 1 shows the meniscal segments superimposed over tibial subregions of cartilage thickness measurement. Extrusion of each meniscus was graded 0–2 (0, none; 1, less than half of the meniscus; and 2, more than half of the meniscus) using coronal images at the collateral ligament level, with extrusion defined as grade greater than 0. One of three experienced musculoskeletal radiologist readers (including AG) graded meniscal parameters. Their interreader reliability (weighted κ) was 0.80 for tears and 0.65 for extrusion. The readers were blinded to all other data.

{kind=link}
Meniscal segments superimposed on the cartilage subregions of articular cartilage thickness measurement
Quantification of subregional cartilage thickness loss on magnetic resonance images
Segmentation involved manual tracing of the total subchondral bone area (tAB) and cartilage surface area of the medial and lateral tibia and weight-bearing femoral condyles on paired (baseline and follow-up) images by 10 operators with standardised training and expertise in knee cartilage segmentation, using dedicated software (Chondrometrics GmbH, Ainring, Germany).27 Quality control of all segmentations was performed by one expert (FE). The operators and quality evaluator were blinded to image acquisition order and all other data. Cartilage thickness was computed over the tAB and in five tibial (central, internal, external, anterior, posterior) and three weight-bearing femoral (central, internal, external) subregions.27 The central (elliptical) subregion occupied 20% of the tAB around its centre of gravity; test–retest precision error for cartilage thickness measurement was 2.4% (root mean square coefficient of variation percentage) and 1.6% for the medial and lateral central tibial subregions.27 Planes running through the tAB centre at a 45° angle with the plane connecting the centre of gravity of the medial and lateral tibia were used to define tibial anterior, posterior, internal and external subregions. Precision error ranged from 1.5% in the external medial tibial subregion to 4.7% in the posterior lateral tibial subregion.27 Each weight-bearing femoral condylar subregion occupied 33.3% of the tAB. Precision error was 3.3% and 2.4% in the central medial and lateral femoral subregions, and ranged from 2.6% in the internal medial femoral subregion to 4.3% in the external lateral femoral subregion.27 For each subregion, cartilage thickness loss was defined as a 5% or greater decrease in cartilage thickness over 2 years, a threshold exceeding the precision errors.
Knee radiographs
Bilateral, anteroposterior, weight-bearing knee radiographs were acquired in all participants at baseline in the semiflexed position with fluoroscopic confirmation of tibial plateau line superimposition and tibial spine centering,28 and read for K/L grade (0, normal; 1, possible osteophytes; 2, definite osteophytes without joint space narrowing; 3, definite joint space narrowing, some sclerosis, possible attrition; and 4, large osteophytes, marked narrowing, severe sclerosis, definite attrition). Intraobserver reliability for the single x-ray reader was high (κ coefficient 0.86).
Statistical analysis
All analyses were knee based. We used logistic regression with generalised estimating equations to estimate OR and 95% CI for the association between baseline meniscal tear in the anterior horn, body and posterior horn and subsequent within-subregion cartilage thickness loss from baseline to 2 years. Cartilage thickness loss in each subregion was defined as a decrease of 5% or greater in thickness at the 2-year measurement compared with baseline thickness in the subregion. Analyses were adjusted for age, gender, body mass index (BMI) and meniscal tear in the other two meniscal segments. The presence of a tear in a meniscal segment was coded as a 0/1 (no tear/tear) indicator variable separately for each segment; all three indicators (one per segment) were included concurrently in each of the logistic models. We first present results adjusting for age, gender, BMI and tears in the other meniscal segments. Additional logistic regression models were used to adjust further for meniscal extrusion to examine whether extrusion explained a subregional tear association with cartilage loss. As meniscal tear and extrusion contribute to the joint space component of the K/L grade, we did not further adjust for K/L grade. Results from logistic regression models are reported as OR and associated 95% CI. Statistical significance is defined at the 5% level, which corresponds to a 95% CI that excludes the value 1.0.
Results
Of 202 participants with knee osteoarthritis in one or both knees who completed the baseline evaluation, 20 did not return at 2 years for the following reasons: deceased; bilateral total knee replacement; moved away or new MRI contraindications. Among the 302 knees of 182 participants, 14 knees were excluded due to missing cartilage data at baseline or at follow-up, 11 for having baseline cartilage thickness of 0 in a subregion, 16 for missing meniscal data, leaving 261 knees from 159 persons as the analysis sample. The 159 participants included 75% women, had a mean age of 66.1 years (±11.1 SD) and a mean BMI of 30.1 kg/m2 (±5.9). Persons without longitudinal data did not differ in age (66.6±11.5) or gender (77% women) but had a higher BMI (31.9±6.2). Among the 261 knees, the K/L grade was 0 in 39 (15%), 1 in 49 (19%), 2 in 100 (38%), 3 in 54 (21%) and 4 in 19 knees (7%). Ninety-two knees (35%) had a medial meniscal tear, 91 (35%) medial meniscal extrusion, 64 (25%) a lateral meniscal tear, 48 (18%) lateral meniscal extrusion, 60 (23%) medial meniscal tear and extrusion and 33 (13%) lateral meniscal tear and extrusion. Within the medial meniscus, 13 knees (5%) had a tear in the anterior horn, 62 (24%) in the body and 77 (30%) in the posterior horn. Within the lateral meniscus, 50 (19%) had a tear in the anterior horn, 50 (19%) in the body and 37 (14%) in the posterior horn. As in table 3, medial meniscal tears were most common in the posterior horn and body concurrently and lateral tears in all three segments concurrently.
Number (%) of knees with meniscal tear in specific meniscal segment(s) (n=261 knees)
Medial meniscal segment tears and medial subregional cartilage thickness loss
At the medial tibia, in the 261 knees, 86 (33%) lost cartilage in the central, 95 (36%) in the external, 53 (20%) in the internal, 85 (33%) in the anterior and 72 (28%) in the posterior subregion. At the medial weight-bearing femur, 94 knees (36%) lost cartilage in the central, 86 (33%) in the external and 80 (31%) in the internal subregion.
The independent effects of a tear within each medial meniscal segment on subsequent subregional cartilage thickness loss, adjusted for age, gender, BMI and tears in the other meniscal segments are shown in table 4. There was no association between baseline anterior horn tear and cartilage loss in any subregion. A body tear at baseline was significantly associated with cartilage loss in the central, external and anterior subregions of the medial tibia and in the external subregion of the medial weight-bearing femur. A posterior horn tear at baseline was significantly associated with cartilage loss in the medial tibial posterior subregion. Further adjustment for meniscal extrusion affected only the external femoral result (table 4).
Medial tibial subregions and medial weight-bearing femoral subregions: adjusted OR (95% CI) for baseline to 2-year cartilage thickness loss
Lateral meniscal segment tears and lateral subregional cartilage thickness loss
At the lateral tibia, in the 261 knees, 106 (41%) lost cartilage in the central, 69 (26%) in the external, 105 (40%) in the internal, 86 (33%) in the anterior and 85 (33%) in the posterior subregion. At the medial weight-bearing femur, 84 knees (32%) lost cartilage thickness in the central, 87 (33%) in the external and 72 (28%) in the internal subregion.
Table 5 shows the independent effects of a tear within each lateral meniscal segment on subsequent subregional cartilage thickness loss after adjustment for age, gender, BMI and tears in the other meniscal segments. There was no association between baseline anterior horn tear and cartilage loss in any subregion. A body tear at baseline was significantly associated with cartilage loss in the central, external, anterior and posterior subregions of the lateral tibia. In addition, a posterior horn tear at baseline was significantly associated with cartilage loss in the lateral tibial external subregion. After further adjustment for meniscal extrusion, there was no evidence of an independent association between body or posterior horn tear and cartilage loss in any subregion (table 5). All analyses were repeated using another definition of meniscal tear, grade 1 or more, with minimal impact on results.
Lateral tibial subregions and lateral weight-bearing femoral subregions: adjusted OR (95% CI) for baseline to 2-year cartilage thickness loss
Discussion
The deleterious effect of a medial meniscal tear on cartilage thickness loss was not uniform across the medial compartment. Meniscal body tear was associated with cartilage loss in external tibial and femoral subregions and in adjacent central and anterior tibial subregions. Meniscal posterior horn tear was associated specifically with cartilage loss in the posterior tibial and no other subregion. These relationships were independent of age, gender, BMI and tears in the other two meniscal segments and persisted in the tibial subregions after further adjustment for meniscal extrusion. In the lateral compartment, meniscal body tear was associated with cartilage loss in the external and adjacent central, anterior and posterior tibial subregions and meniscal posterior horn tear with cartilage loss in the external tibial subregion. These lateral compartment relationships were attenuated by further adjustment for meniscal extrusion. Cartilage loss in the internal subregions, which are not covered by the meniscus, was not associated with any meniscal segment tear. These findings demonstrate the significance of meniscal damage for subsequent subregional cartilage thickness loss and suggest that at least some of the meniscal tear effect is experienced locally.
Our findings are in keeping with previous reports in which meniscal damage was associated with knee osteoarthritis progression at the larger joint surface15,–,18 and some early subregional findings. Lynch et al21 found that, in knees with or at higher risk of developing knee osteoarthritis, medial cartilage score worsening associated with medial meniscal tear appeared to be more frequent in the central subregions. In the BOKS study, Niu et al20 used an M:N matched case–control design including knees with six tibial subregions eligible for cartilage score worsening and with worsening in one subregion at follow-up. In the 37 knees examined, compared with tibial subregions without meniscal damage in identical locations, the OR of cartilage worsening in sites with such damage was significantly increased.
In contrast, we examined quantitative cartilage thickness loss within tibial and femoral subregions and were thereby not vulnerable to potential bias associated with grading menisci and cartilage subregions together in the same session. Crema et al22 also measured cartilage thickness, but studied women with or without knee osteoarthritis. As their goals and analytical methods differed from ours, it is difficult to derive answers to the questions we posed directly from their report. In contrast to all of these previous studies, we adjusted not only for extrusion, but addressed potential confounding from tears in the other two meniscal segments, a key step in the examination of a local effect.
In our study, isolated meniscal tear occurred most frequently in the medial meniscal posterior horn, in agreement with previous reports.29,–,31 The reduced mobility from soft tissue attachments and greatest load transmitted through this region during knee flexion makes this meniscal segment particularly vulnerable.30,–,32 The most common medial pattern, however, was concurrent body and posterior horn tear. The most common lateral meniscal tear pattern (involving all three segments) may relate to its greater mobility and more even between-segment sharing of load.31 32
The finding that baseline medial meniscal body tear had the strongest association with subsequent cartilage loss in the external tibial subregion where the body segment overlies supports some local impact of meniscal damage on cartilage health. Baseline posterior horn tear had an isolated effect in the posterior tibial subregion. The small number of knees with anterior horn tear may have limited our ability to detect relationships involving tears in this segment. The relationship between body tear and anterior tibial cartilage loss may relate to the proximity of anterior and external subregions (figure 1).
The effects of baseline lateral meniscal body tear were less confined to the anatomical mapping proposed in our hypotheses. During knee flexion, the lateral meniscus experiences nearly twice the magnitude of anteroposterior translation as the medial meniscus.32 With this movement, the lateral meniscal body segment may overlie the anterior, external, central and posterior tibial cartilage subregions and the posterior horn may overlie the posterior and external tibial subregions. The associations between lateral meniscal tear and cartilage loss were attenuated by adjustment for meniscal extrusion. In theory, extrusion of the more mobile lateral meniscus could itself contribute to a more diffuse tear pattern, and less matching between tear site and subregion of cartilage loss.
It is important to acknowledge that some knees without longitudinal data came from individuals whose BMI was greater than the individuals we analysed; it is uncertain how this may have affected the results. While the WORMS system is commonly applied to assess meniscal tears in knee osteoarthritis, it does not include tear type or location in relation to vascular supply. Furthermore, efforts to match meniscal segment to cartilage subregion are inherently imperfect: optimal meniscal grading and cartilage segmentation require different sets of magnetic resonance images; knees vary in meniscal and articular cartilage shape; and the match may be altered by meniscal movement and/or extrusion during activity.
In summary, the detrimental effect of meniscal tears is not spatially uniform across the tibial and femoral cartilage surfaces, and at least some of it is experienced locally. These results support a focal protective role of meniscal tissue on articular cartilage integrity in knee osteoarthritis.
References
Footnotes
-
Funding This study was funded by NIH NIAMS R01 AR48216, R01 AR48748, P60 AR48098.
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval Approval was obtained from the Office for the Protection of Research Subjects of Northwestern University and Evanston Northwestern Healthcare.
-
Provenance and peer review Not commissioned; externally peer reviewed.