Article Text

Abstract
Background Since the publication of the European League Against Rheumatism (EULAR) recommendations for the management of large vessel vasculitis (LVV) in 2009, several relevant randomised clinical trials and cohort analyses have been published, which have the potential to change clinical care and therefore supporting the need to update the original recommendations.
Methods Using EULAR standardised operating procedures for EULAR-endorsed recommendations, the EULAR task force undertook a systematic literature review and sought opinion from 20 experts from 13 countries. We modified existing recommendations and created new recommendations.
Results Three overarching principles and 10 recommendations were formulated. We recommend that a suspected diagnosis of LVV should be confirmed by imaging or histology. High dose glucocorticoid therapy (40–60 mg/day prednisone-equivalent) should be initiated immediately for induction of remission in active giant cell arteritis (GCA) or Takayasu arteritis (TAK). We recommend adjunctive therapy in selected patients with GCA (refractory or relapsing disease, presence of an increased risk for glucocorticoid-related adverse events or complications) using tocilizumab. Methotrexate may be used as an alternative. Non-biological glucocorticoid-sparing agents should be given in combination with glucocorticoids in all patients with TAK and biological agents may be used in refractory or relapsing patients. We no longer recommend the routine use of antiplatelet or anticoagulant therapy for treatment of LVV unless it is indicated for other reasons.
Conclusions We have updated the recommendations for the management of LVV to facilitate the translation of current scientific evidence and expert opinion into better management and improved outcome of patients in clinical practice.
- large vessel vasculitis
- giant cell arteritis
- Takayasu arteritis
- management
- Eular recommendations
Statistics from Altmetric.com
Background
Rapid diagnosis and effective treatment are required in large vessel vasculitis (LVV) in order to treat symptoms, but more importantly, to reduce the risk of complications such as blindness in giant cell arteritis (GCA) and aortic aneurysm or vascular stenosis in GCA and Takayasu arteritis (TAK). In April 2008, the first recommendations of the European League against Rheumatism (EULAR) for managing LVV were published.1 These recommendations have provided guidance to clinicians and researchers and have been widely cited. Since then, the results of several randomised clinical trials and cohort analyses have become available and the EULAR recommendations on imaging in LVV have been published recently.2
In light of these and other fundamental developments affecting key areas of management, the goal of the current project was to re-evaluate the literature in order to update the EULAR recommendations for the management of LVV.
Methods
The recommendations were drafted according to the 2014 update of the EULAR standardised operating procedures (SOPs) for the development of EULAR-endorsed recommendations and the updated version of the Appraisal of Guidelines for Research & Evaluation (AGREE II) recommendations, where applicable (see online supplementary file 1 for a full description of methods).3 4 The task force consisted of 20 clinical experts (including rheumatologists, internists, immunologists, a neurologist, a neuro-ophthalmologist and an epidemiologist), from 11 European countries, India and China, two fellows (AA, SM), one health professional and two patients affected by the diseases under study.
Supplemental material
Based on results of a Delphi survey among the task force, we defined eight key research questions addressing the management and treatment of LVV. As the original systematic literature review (SLR) for the 2008 recommendations dated back 10 years ago with different methodology, it was decided to conduct two completely new SLRs without time limits, focusing on general management and treatment, respectively (table 1).
Topics for the systematic literature search
The following databases were used: MEDLINE, EMBASE and Cochrane CENTRAL. Each article was assigned a level of evidence (LoE) according to the standards of the Oxford Centre for Evidence-Based Medicine and was systematically assessed for bias.3 The methods and results of the two SLRs are published separately.5 6
During a face-to-face meeting, task force members independently voted on each recommendation. Agreement on each recommendation and on the overarching principles on a scale of 0–10 (10 meaning full agreement) was given anonymously after the meeting by e-mail. A research agenda was formulated based on controversial issues and gaps in the evidence. The final manuscript was approved by the EULAR Executive Committee.
Results
General aspects
The objective of the updated recommendations is to give advice on the management of LVV to rheumatologists and other health professions involved in the care of these patients. Because EULAR recommendations on imaging in LVV have been published recently,2 the task force agreed to refer to these recommendations removing topics regarding imaging from the update of the management recommendations.
To reduce confusion currently existing in the literature we propose new consensus definitions for disease activity states in LVV (table 2), based on the concept of activity states developed for the EULAR recommendations for small vessel vasculitides (SVV).7
EULAR consensus definitions for disease activity states in GCA and other types of LVV
Key symptoms and clinical findings suggestive of active large vessel vasculitis
The new definitions are consensus based and do not derive from the SLR. They differ in some details from definitions used in recent clinical trials (for comparison see online supplementary file 2). By analogy to the EULAR definitions for SVV,7 we suggest using the term ‘relapse’ consistently, but avoiding the term ‘flare’. We propose a distinction between major and minor relapses because the prognosis and treatment of relapses in LVV depends on the presence of ischaemia and/or development or progression of vascular damage. In contrast to SVV, true refractory disease in LVV is very rare because patients usually respond well to high dose glucocorticoids (GCs). However, in the past, the term ‘refractory’ was sometimes used for patients with LVV and GC-dependent disease that relapsed when GCs were tapered. We propose that the activity state ‘refractory’ should be used to reflect the difficulty in achieving disease control despite the patient remaining on an appropriate treatment schedule (which would include tapering of the GC dose).
Supplemental material
In 2012, IgG4-related (peri-)aortitis and isolated aortitis, either primary or secondary to infection (eg, syphilis) or other systemic diseases were recognised as separate entities by the Chapel Hill consensus conference.8 The SLR revealed only very low evidence on management of these rare entities, which did not allow us to generate separate recommendations. Therefore, we encourage further research on these subtypes, as outlined in the research agenda below.
Overarching principles
The task force identified general principles that were deemed fundamental for the management of patients with LVV (table 3). These principles were consensus based and did not directly result from the SLR. The overarching principles and the specific recommendations are listed in table 3.
EULAR recommendations for the management of LVV—2018 update
Recommendations
All patients presenting with signs and symptoms suggestive of GCA should be urgently referred to a specialist team for further multidisciplinary diagnostic work-up and management
Untreated active GCA is an emergency and carries a substantial risk of permanent visual loss and other ischaemic complications. Therefore, we recommend that all patients ≥50 years of age presenting with acute or subacute onset of signs and symptoms suggestive of GCA (table 4) and raised inflammatory markers without explanation (eg, infection) should be referred urgently to a specialist team/experienced centre for further diagnostic work-up. This team or centre should have expertise in the disease, have rapid access to up-to-date imaging2 and temporal artery biopsy (TAB) and should offer fast referral. Patients with new onset of visual symptoms should be seen as soon as possible by an ophthalmological team to exclude other causes of sudden visual disturbance. In case of signs of cerebral ischaemia, rapid review by a neurologist is recommended.
Results from two retrospective cohort studies have shown that immediate treatment of GCA patients and rapid referral to a specialised centre (‘fast-track clinic’) for diagnostic work-up, including imaging, within 24 hours after presenting with signs and symptoms of GCA can reduce the rate of permanent visual impairment compared with historical cohorts with routine non-urgent referral.9 10 Although these studies were retrospective and therefore subject to bias, the available limited evidence supports rapid referral in order to confirm the diagnosis of GCA.11
Patients with both typical symptoms and increased C-reactive protein (CRP)/erythrocyte sedimentation rate (ESR) who present with acute visual disturbance should be treated before the appointment, as delaying GC therapy when visual loss is present is the strongest risk factor for permanent blindness.12 For patients without visual symptoms, there was no consensus among the task force members as to whether pre-emptive treatment with GCS should be started in all cases of suspected GCA in addition to fast referral to a specialised centre. In any case, pre-emptive therapy should only be given for a short period of time and should not delay early referral because the sensitivity of diagnostic tests decreases following treatment with GCs and to avoid unnecessary exposure to GCs of cases for whom the diagnosis of GCA is eventually not maintained. Although, the sensitivity of diagnostic tests decreases following treatment, imaging and biopsy may show features of GCA even weeks after GC therapy.13–16 Therefore, diagnostic tests to confirm a suspected diagnosis of GCA should be performed in all patients irrespective of the duration of pre-emptive therapy.
All patients presenting with signs and symptoms suggestive of TAK should be referred to a specialist team for multidisciplinary diagnostic work-up and management
The majority of symptoms of TAK (table 4) are non-specific, but should prompt a thorough examination of the arterial tree. Because there is no gold standard for the diagnosis of TAK, we recommend referral to an experienced centre for further work-up including large-vessel imaging. Studies on fast-track referral are lacking for patients with TAK. Patients with individual presentations suggesting an increased risk of ischaemic complications need a more urgent referral.
A suspected diagnosis of LVV should be confirmed by imaging (ultrasound or MRI for temporal or other cranial arteries, ultrasound, CT, positron-emission-tomgraphy (PET)T-CT or MRI for the aorta/extracranial arteries) or histology (TAB)
Every effort should be made to confirm a suspected diagnosis of LVV. In rare cases, both imaging and biopsy are negative. If the clinical probability in such cases is high, a provisional diagnosis of GCA may be made, which needs to be confirmed or revised during follow-up.
The original recommendations advised TAB in every case of suspected GCA.1 Since then, a large amount of good-quality data demonstrated that imaging and biopsy have similar diagnostic value if assessors are proficient in these techniques.2 13 The recently published EULAR recommendations for the use of imaging in LVV in clinical practice contain comprehensive advice regarding when and how the different imaging modalities should best be used in different subsets of LVV.2 Several studies have shown that neither imaging nor TAB are 100% sensitive.2 13 17–19 Imaging of the temporal arteries by ultrasound or MRI identifies only 77% and 73% of cases, respectively, with clinical diagnosis as reference standard for GCA.14 20 21 Thus, performing a second test can be considered if the first was negative but the clinical suspicion of GCA persists.
Ultrasound guidance appears not to improve the diagnostic yield of TAB.22 Biopsies should be at least 1 cm in length, which corresponds to a postfixation length of at least 0.7 cm.17 Biopsy of the contralateral artery does not add significantly to the diagnostic yield and is therefore not routinely recommended. Overall, available data do not provide convincing evidence that any individual characteristics of the biopsy findings (eg, composition or intensity of the inflammatory infiltrate) are sufficiently predictive for subsequent clinical events to allow guidance of treatment decisions or follow-up in clinical practice.23–35
ESR and CRP are typically elevated in GCA, and it is highly infrequent (<3%) that both are normal.36 37 While several other serological biomarkers have been evaluated, none is sufficiently sensitive and specific for detection and assessment of disease activity or prediction of prognosis to recommend its use in clinical practice.
In patients with atypical clinical presentations not compatible with current disease definitions,8 an alternative diagnosis or overlapping associated diseases should be considered, in the diagnostic work up, such as for example aortitis related to IgG4-related disease, LVV in anti-neutrophil-cytoplasm (ANCA)-associated vasculitis (AAV) or other vasculitides (eg, Behçet’s syndrome), or LVV secondary to spondyloarthropathies, relapsing polychondritis or infections.
High dose GC therapy (40–60 mg/day prednisone-equivalent) should be initiated immediately for induction of remission in active GCA or TAK. Once disease is controlled, we recommend tapering the GC dose to a target dose of 15–20 mg/day within 2–3 months and after 1 year to ≤5 mg/day (for GCA) and to ≤10 mg/day (for TAK)
Induction treatment with a starting GC dose of 40–60 mg per day (all GC doses discussed in this article are prednis(ol)one equivalent) leads to remission in the majority of patients with LVV.38–43 Although the maximum genomic effect of GCs is around 100 mg of prednisone-equivalent,44 there is no clear evidence that starting doses of above 60 mg per day are more effective than 60 mg per day in the prevention of ischaemic events or other relevant endpoints. It should be noted that the genomic effects of glucocorticoids depend on certain patient-specific pharmacokinetic and pharmacodynamic factors. These include for example total cell number (indirectly quantified by weight), numbers of glucocorticoid receptors per cell, and glucocorticoid receptor binding affinity.45 46 The relatively high variability of these factors explains why neither the dose-dependent efficacy of a glucocorticoid therapy can be predicted absolutely correctly, nor a weight-adapted therapy with glucocorticoids is recommended. As a consequence, and since differences between certain dosages or weight-adapted glucocorticoid dosages have not been rigourosly tested in clinical trials, the current recommendations provide dose ranges.
In patients with GCA with acute visual loss or amaurosis fugax, the administration of 0.25–1 g intravenous methylprednisolone for up to 3 days should be considered, because these high doses have both genomic and rapid non-genomic effects.44 45 However, there are only low-quality retrospective clinical data supporting this recommendation.47 48 Referral for intravenous GC therapy should not delay treatment with oral GC. The SLR revealed quality issues in both randomised controlled clinical trials (RCTs) of high dose pulse intravenous GC therapy in patients without visual symptoms.40 41 In view of the limited quality of evidence, the task force recommends limiting the use of intravenous pulse GC therapy to patients with complicated GCA such as those with GCA-related visual symptoms.
We recommend tapering the GC dose, once remission has been achieved. A GC taper regimen must weigh the risk of relapse against the risk of GC-related adverse events. In GCA, relapses are common once the GC dose is tapered. Several large observational cohort studies have shown relapse rates of 34%–75% in patients with GCA treated with GC therapy.33 49–58 The large variation of relapse risk in those studies was most likely due to different definitions for relapse (eg, symptoms plus CRP increase vs symptoms or CRP increase) and different tapering protocols. Each relapse requires a reinstitution or a dose-increase of GCs resulting in high cumulative GC exposure in a substantial proportion of patients which then leads to an increased risk of GC-related adverse events.43 49 52 54 59–64
A RCT of tocilizumab (TCZ) for treatment of GCA contained two placebo arms, one with a 26-week GC taper protocol and the other with a 52-week taper protocol.38 65 Prednisone doses were identical in both arms until 20 mg/day with similar numbers of relapses in both groups; from week 15 onwards the arm with the faster dose reduction appeared to be associated with a higher relapse risk.38 Data from an earlier open label prospective observational study comparing two different GC taper protocols also showed a rapid taper protocol to be less effective than a standard taper in maintaining remission.42 For patients who are not eligible for GC sparing therapy, we advise against the use of these rapid taper regimens in standard clinical practice; they reflect clinical trial designs with the intention to test the GC sparing property of experimental adjunctive agents.
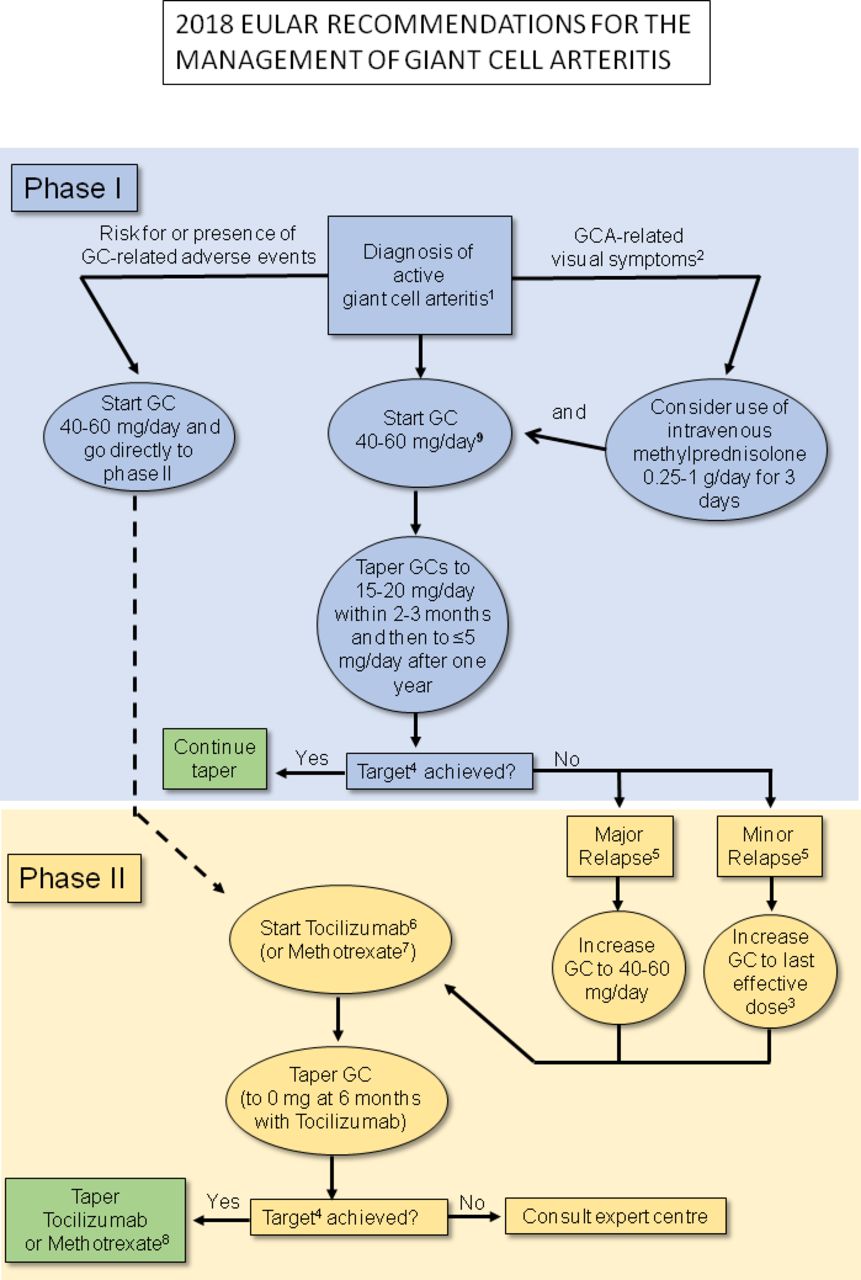
In summary, considering the increased relapse risk after early taper and/or reduction of the GC dose below 5 mg/day, we recommend tapering the GC dose in GCA to a target of 15–20 mg/day within 2–3 months and then to ≤5 mg/day after 1 year (figure 1). Despite the lack of data regarding the optimal length of GC therapy, the majority of panel members reported that it usually takes about 2 years or more before GCs can be stopped. In patients receiving GC-sparing therapy, faster GC taper and earlier withdrawal of GCs should be considered on an individual basis, given the lack of data. In patients treated with TCZ, the published rapid 26-week GC taper may be attempted in order to significantly reduce the cumulative dose. It is not known if even faster or conversely more prolonged GC withdrawal during TCZ therapy may lead to improved outcomes.
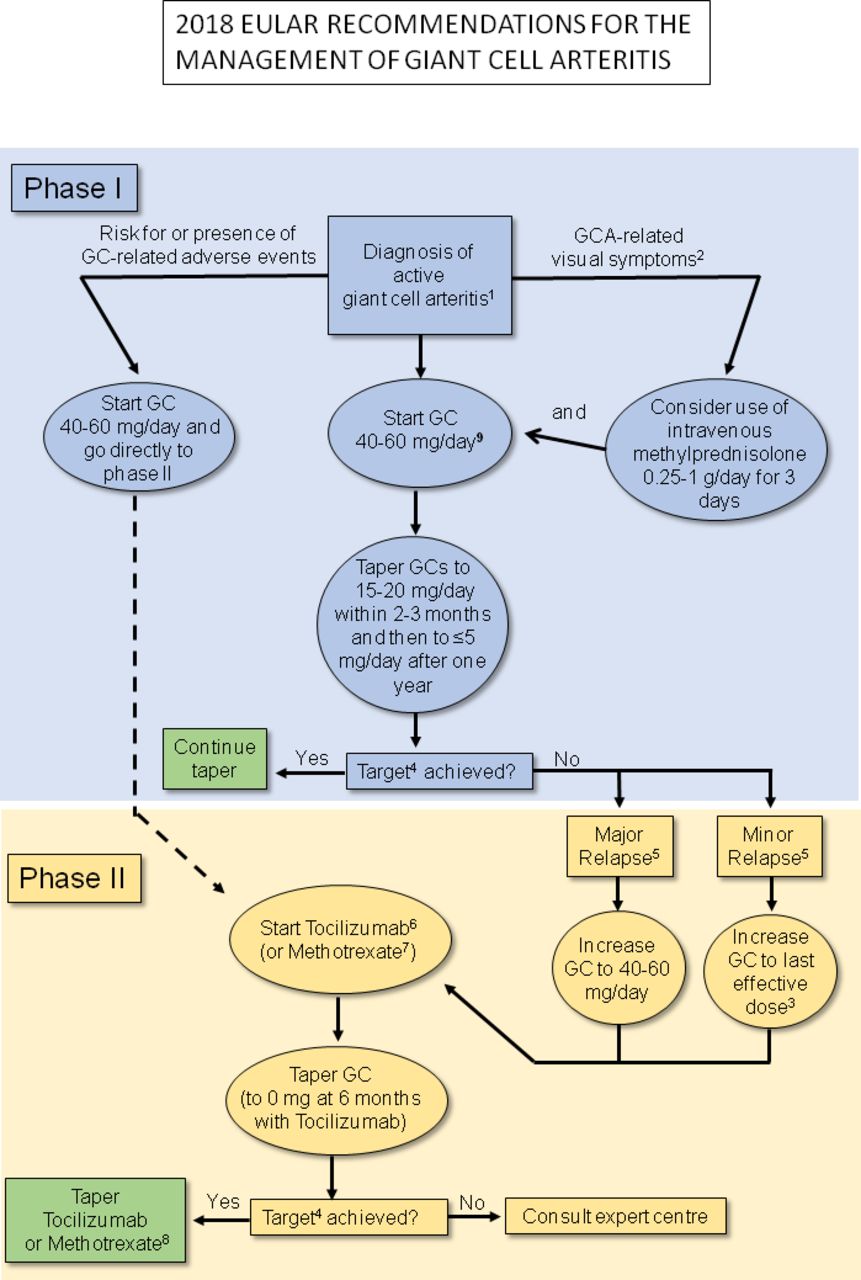
The 2018 EULAR algorithm for pharmacological treatment of giant cell arteritis (GCA). GC, glucocorticoids. 1A clinical diagnosis of GCA should be confirmed by either imaging or biopsy2; acute loss of vision, amaurosis fugax3 ;or 5–15 mg/day above the last effective dose4;the treatment target is sustained remission (absence of clinical signs and symptoms of active GCA+normal acute phase reactants) plus ability to taper GCs to the specified target without relapse5;see table 2 for definitions6;recommended dose is 162 mg7; minimum recommended dose is 15 mg 8;to be decided on an individual basis (lack of evidence)9 ;in patients with GCA-related visual symptoms consider a starting dose of 60 mg prednisone per day after GC administration.
For TAK, there are no studies comparing different GC taper protocols. Clinical experience suggests that a starting dose of 40–60 mg per day is appropriate for the majority of patients, while patients with more localised disease may respond to lower initial GC doses of 25–30 mg per day. In a recent small RCT of TCZ in TAK, a taper of GC in the placebo group by 10% per week after week four resulted in a high relapse rate (around 80% during weeks 8–16).66 A similar relapse rate in TAK patients treated with GC monotherapy was observed in a recent RCT of abatacept.67 We therefore recommend that in patients who have reached a GC dose of 15–20 mg/day after 2–3 months, GC doses should subsequently be reduced more slowly as compared with GCA, targeting a dose of ≤10 mg/day after 1 year (figure 2).

{kind=link}
{kind=link}
The 2018 EULAR algorithm for pharmacological treatment of Takayasu arteritis (TAK). csDMARD, conventional synthetic disease modifying anti-rheumatic drug; GC, glucocorticoids; TNF, tumour necrosis factor; 1A clinical diagnosis of TAK should be confirmed by imaging2; in patients with more localised disease consider lower initial dose of 25–30 mg/day3; methotrexate or mycophenolate mofetil, leflunomide or azathioprine (when a patient does not tolerate the first choice drug switching is an option) or cyclophosphamide (only if other treatments have failed or have not been tolerated) can be used as an alternative4; or 5–15 mg above the last effective dose5; see table 2 for definitions6; the treatment target is sustained remission (absence of clinical signs and symptoms of active Tak associated with normal acute phase reactants) plus ability to taper GCs to the specified target without relapse7; tocilzumab is not formally licensed for use in TAK in the European Union (EU), the recommended dose is 162 mg one time per week s.c.8; Tumor necrosis factor (TNF)-inhibitors are not formally licensed for use in TAK (when a patient does not tolerate the first choice biological switching is an option).
Adjunctive therapy should be used in selected patients with GCA (refractory or relapsing disease, the presence or an increased risk of GC related adverse effects or complications) using TCZ. Methotrexate may be used as an alternative
The original recommendations suggested adjunctive immunosuppressive therapy in all patients with LVV. However, although the risk of relapse in GCA is high, a substantial number of patients with GCA treated with GC monotherapy do not relapse and are able to taper the GC dose according to a target of ≤5 mg/day after 1 year,49 50 52 a dose which the EULAR task force considered to be acceptably safe.68 Therefore, we recommend limiting the use of adjunctive therapy to patients who have already developed, or have either an increased risk of developing GC-related side effects or complications, such as osteoporosis, diabetes, cardiovascular disease or glaucoma, or for relapsing patients irrespective of other risk factors. Given the high prevalence of comorbidities in the elderly population affected by GCA, the decision to use adjunctive immunosuppressive therapy in the individual patient should be balanced against potential risks for treatment-related complications, such as the increased risk of lower intestinal perforations reported in patients with rheumatoid arthritis receiving TCZ.69So far, no consistent factors have been identified at the time of diagnosis to predict an increased relapse risk and risk for subsequent high GC exposure in LVV.49–55 Therefore, the identification of reliable predictive factors for relapse and prolonged GC requirement in LVV remains an important topic for future research.
Two high-quality randomised controlled clinical trials in patients with GCA have shown that adjunctive administration of TCZ reduces the risk of relapse and cumulative GC exposure compared with GC monotherapy.38 70 Because TCZ suppresses CRP synthesis in the liver, the presence of a normal CRP or ESR may be falsely reassuring, although sensitivity analyses in the GiACTA trial suggest that this problem did not affect the primary outcome.38 However, with the limited reliability of acute phase reactants for activity assessment in patients receiving TCZ, follow-up is largely symptom-based, which can make monitoring disease activity difficult. Thus, further studies on the role of imaging and other biomarkers for disease monitoring are needed. As high-quality long-term data are missing, it is not known if TCZ can reduce the risk of aneurysms or vascular stenosis. Hypothetically, the development of vascular long-term damage may occur despite TCZ therapy.71
Of three RCTs on the use of methotrexate (MTX) in newly diagnosed GCA,72–74 only one74 met its primary endpoint. As outlined in our SLR analysis in more detail, all of these trials were conducted more than 20 years ago, had differences in the study design and sample size which could have all accounted for the divergent outcomes. Importantly, the maximum weekly MTX doses of 7.5, 10 and 15 mg p.o. used in all three studies were lower than those used in clinical practice today. Despite methodological limitations of the individual studies, a high quality meta-analysis using pooled individual patient data from these trials demonstrated a reduced risk of first relapse (HR 0.65, 95% CI 0.44 to 0.98, p=0.04) and second relapse (HR 0.49, 95% CI 0.27 to 0.89, p=0.02), a higher probability of GC-free remission for ≥24 weeks (HR 2.84, 95% CI 1.52 to 5.28, p<0.001) and a lower cumulative GC dose of –842 mg at week 48 in patients treated with MTX versus controls.75 Of note, adverse events and early withdrawals were not different between MTX and placebo groups in the metaanalysis.75
There are no trials comparing TCZ and MTX in GCA and the differing study designs preclude strong conclusions about the potential superiority of one agent over the other. However, compared with MTX, the effect size of TCZ in terms of relapse risk reduction and GC sparing seems larger and the meta-analysis on MTX revealed hetereogeneity of results between the individual studies. Therefore, TCZ provides a higher confidence in achieving a clinically relevant treatment effect as compared with MTX. Further studies are needed to define the optimal length of treatment, GC taper regimens, cost effectiveness and monitoring. At present, there are few and only low-quality data on long-term treatment with MTX or TCZ in GCA.76 77 Therefore, the duration of treatment and potential dose reductions must be decided on an individual basis. As current evidence does not suggest an excessive risk of treatment-related complications of TCZ or MTX as compared with other indications,38 75 patients should be monitored for treatment-related side effects according to existing guidelines for other diseases.78
Data for other adjunctive therapies are either sparse (abatacept), derived from low-quality studies (ustekinumab, azathioprine, leflunomide, cyclophosphamide, dapsone, etanercept) or negative (adalimumab, infliximab, cyclosporine).79–90
Non-biological disease modifying agents should be given in combination with GC in all patients with TAK. TCZ or tumour necrosis factor-inhibitors can be considered in case of relapsing or refractory disease despite conventional disease modifying anti-rheumatic drug therapy
In view of the high relapse rates of up to 70%, the development of new vascular lesions and the inability of many patients to achieve low GC doses,91 92 we advise that early administration of a GC-sparing agent in TAK is justified and reflects current treatment practice in more recent cohorts.93 94 However, we acknowledge that the LoE supporting this recommendations is low.
Only two RCTs, both on biological agents, have been published, neither of which met its primary endpoint for efficacy.66 67 The evidence for a use of TCZ in TAK comes largely from one small RCT showing a statistically borderline signal (p=0.0596) towards reduced HR for the time to the first relapse and similar non-significant improvement in some secondary endpoints in the TCZ-treated patients.66 Additional experience with TCZ treatment in TAK was reported from one prospective and four retrospective case series including a total of 89 patients of which the majority had refractory or relapsing disease despite treatment with GC or other agents.95–100 Efficacy of tumour necrosis factor (TNF)-inhibitors in TAK has been reported in one prospective and several retrospective open-label uncontrolled studies/case series.101–111 Overall, the reported reductions in disease activity in all these case series need to be interpreted with caution, because disease activity in TAK may decrease as a result of continued GC therapy over time. In contrast to the positive trends observed in GCA, the RCT of abatacept did not show any signs of efficacy in TAK.67 Lower quality evidence from uncontrolled prospective and retrospective case series exists for the use of conventional immunosuppressive agents such as MTX, leflunomide, mycophenolate mofetil, azathioprine and cyclophosphamide in TAK.112–117 Since TAK targets primarily women with childbearing potential and is a chronic and usually not acutely life threatening disease (unlike AAV), the use of cyclophosphamide should be limited to patients where other treatments have failed or are not tolerated. There is no high-quality evidence showing superiority of biologicals over conventional disease modifying anti-rheumatic drugs (DMARDs) in TAK.
Despite this overall low LoE, we recommend considering adjunctive treatment with conventional immunosuppressive drugs at diagnosis of TAK. A TNF-inhibitor or TCZ can be used as second line agents in case of relapsing disease. The choice of a specific immunosuppressive agent should be based on patient comorbidities or contraindications. GCs should be tapered to the lowest possible dose during treatment with immunosuppressive agents. Because good-quality data on long-term treatment of TAK are lacking, the duration of treatment must be decided on an individual basis. One study indicated that relapse risk is particularly high during the first 5 years following diagnosis.92
In case of major relapse (either with signs or symptoms of ischaemia or progressive vascular inflammation) we recommend reinstitution or dose escalation of GC therapy as recommended for new onset disease. For minor relapses we recommend an increase in GC dose to at least the last effective dose. Initiation or modification of adjunctive therapy should be considered particularly after recurrent disease relapses
There are no studies specifically addressing the treatment of relapse in LVV. Even larger cohort studies on relapses in GCA often lack detailed information on treatment of the relapse (GC dose, tapering, initiation of adjunctive treatment, etc).50 51 Protocols for relapse treatment differ among RCTs and the heterogeneous study designs and adjunctive therapies do not allow for robust conclusions regarding which of the different strategies is the best.
Major relapses impose the risk of subsequent organ damage due to ischaemia and/or progressive vascular inflammation (eg, progressive large vessel stenosis) and should therefore be treated like new-onset disease with high dose GC (initial dose 40–60 mg/day) as outlined above (recommendations 3 and 4). In case of a minor relapse (eg, recurring isolated polymyalgia rheumatica (PMR) symptoms), we recommend an increase of the daily GCs dose either to the last effective dose or to 5–15 mg above this dose, the latter being common practice in many centres.
Disease relapses in LVV are most commonly but not always accompanied by an increase of ESR and CRP.49 51 52 118 In the absence of symptoms of LVV, a rise of ESR or CRP should not automatically prompt an immediate escalation of immunosuppressive therapy. Infections should be ruled out first. If repeated measurements confirm a substantial elevation of ESR and CRP and if there is no evidence for another cause of the inflammatory response, large vessel imaging should be considered. In the presence of less specific symptoms (eg, diffuse headache) in patients with normal inflammatory markers, imaging (ultrasound, MRI or PET-CT) may be helpful.2 However, signals of vessel wall inflammation on imaging may persist even in complete clinical remission.16 119 At present, it is unknown if such residual activity represents true active disease or remodelling. Therefore, such imaging findings observed during follow-up have to be interpreted with caution considering the disease course of the individual patient and by comparing them to imaging findings previously obtained.2
As outlined in recommendation 5, we recommend adjunctive GC sparing therapy (if not already begun at disease onset) or a modification (dose escalation or switch to another agent) of an already existing GC-sparing therapy in relapsing patients in order to improve long-term disease control. So far, there are no RCTs that have specifically focused on the adjunctive treatment of relapses. However, the GiACTA trial included 132 relapsing patients and TCZ was superior to GC monotherapy in this situation.38 All three RCTs of MTX in GCA included patients with new onset disease only. However, patients who received MTX had a 50% lower risk (p=0.02) of developing a second relapse in a meta-analysis, thus providing evidence for the efficacy of MTX after a first relapse. Other agents have either not been studied prospectively or showed no signs of efficacy in relapsing GCA.
In relapsing TAK despite treatment with GC plus a conventional immunosuppressive agent, a TNF-inhibitor or TCZ can be used as second line agent (see also recommendation 6).
Antiplatelet or anticoagulant therapy should not be routinely used for treatment of LVV unless it is indicated for other reasons (eg, coronary heart disease, cerebrovascular disease, etc). In special situations such as vascular ischaemic complications or high risk of cardiovascular disease, these might be considered on an individual basis
Patients with GCA are at an increased risk of developing cardiovascular and cerebrovascular events.120 121 The original EULAR recommendation to use aspirin prophylactically in GCA was based on data from two retrospective studies showing that patients who received low-dose aspirin before or at the time of diagnosis of GCA may have reduced rates of vision loss or stroke, although the number of events was low in these cohorts.122 123 However, two more recent cohort studies and a meta-analysis did not confirm a protective effect of aspirin in GCA.124–126 Balancing the potential protective effect (which is unknown) of aspirin against its potential harm (such as bleeding),127 we decided to change the original statement and now recommend that antiplatelet or anticoagulant therapy should not be routinely prescribed unless they are indicated for other reasons (eg, coronary heart disease, cerebrovascular disease, etc).
A significantly decreased risk of ischaemic events was reported from a single cohort of 41 TAK patients using anti-platelet therapy.128 In view of the low LoE, a vascular team should decide on the use of anti-platelet therapy in TAK on an individual basis taking the degree of vessel stenosis and other risk factors into account.
In LVV, elective endovascular interventions or reconstructive surgery should be performed during stable remission. However, arterial vessel dissection or critical vascular ischaemia requires urgent referral to a vascular team
Interventional or surgical therapy is indicated if a vascular lesion that persists despite medical therapy is either symptomatic (such as a peripheral artery limb stenosis causing claudication) or is associated with an increased risk of future complications (such as rapid progression of an aortic aneurysm). The method of choice for vascular interventions in patients with LVV depends on the anatomic location of the vascular damage, timing (elective vs emergency) and other factors.
Undertaking surgical interventions in patients with active disease is associated with an increased risk of complications and lower patency rates.129–132 Procedures should preferably be performed only during stable control of inflammation, except for emergency indications such as critical ischaemia, neurological complications such as stroke or aneurysm dissection. Otherwise, interventional and surgical vascular therapy follows the same principles as in patients without vasculitis.133 134 Given the complexity of LVV, patients selected for interventional or surgical therapy should be managed in collaboration with a multidisciplinary team (the exact constituency will vary, but could include vascular radiologists, vascular surgeons, neurologists and rheumatologists).
Regular follow-up and monitoring of disease activity is recommended in patients with LVV, primarily based on symptoms, clinical findings and ESR/CRP levels
There are no data available to guide long-term follow-up of patients with GCA or TAK. In view of the high frequency of relapses and the potential harm resulting from relapse-related vessel and organ damage, routine follow-up visits could be scheduled every 1–3 months during the first year and in 3–6 months intervals afterwards. In patients with relapse-free remission, annual follow-up under shared care between rheumatologists and primary care can be considered. As late relapses can occur and the incidence of structural vascular lesions in GCA increases after 5 years from diagnosis,49 50 135 long-term follow-up of patients with GCA that remain asymptomatic can be scheduled on an individual patient basis.
Visits should include clinical monitoring and measurement of ESR and CRP. Routine imaging for activity assessment is not recommended for patients in clinical and biochemical remission, but may be used for long-term monitoring of structural damage, particularly vessel stenosis, dilatation and/or aneurysms.2 Methods and frequency of imaging should be decided on an individual basis.2 LVV-specific patient-reported outcome instruments for use in clinical practice are not available,38 136–138 and should be the subject of future research.
Discussion
Since the first EULAR recommendations on the management of LVV were published, high-quality diagnostic studies and several RCTs have expanded our knowledge about these complex diseases and allowed a significant update of the original recommendations. In view of new research questions to be addressed, improvements in SOPs and methodology for the development of EULAR recommendations,3 we undertook two completely new SLRs without time limits. Therefore, this update represents a new set of recommendations rather than a simple revision. While the majority of the original recommendations addressed LVV in general, new data allowed us to offer separate recommendations for GCA and TAK at least for some key areas of management. In GCA, disease subsets with only cranial, only extracranial or cranial plus extracranial arteritis have been described. High-quality evidence to guide differential management of these subtypes is yet lacking. Therefore, all recommendations on GCA management inhere refer to all subtypes of GCA.
For this update, we have made substantial alterations, including the introduction of overarching principles and new recommendations on early diagnosis, multidisciplinary management and relapse treatment.
Research agenda
A. Diagnosis and classification
Develop data-driven classification criteria for large vessel vasculitis (LVV).
Develop data-driven diagnostic criteria for LVV.
Develop data-driven definitions for disease activity states (remission, response, relapse) and standardisation of outcome measures used in trials for LVV.
Develop data-driven definitions of disease subtypes of importance in giant cell arteritis (GCA).
Identify reliable biomarkers and risk factors for relapsing disease and future vascular complications.
Identify reliable biomarkers to assess subclinical disease activity and monitor treatment response.
Investigate the use of the different imaging techniques for vascular activity and damage assessment and follow-up of patients with LVV, as outlined in the EULAR recommendations on imaging in LVV2.
Investigate the role of ultrasound for guiding temporal artery biopsy.
B. Treatment
Evaluate the effects of a mechanism-based approach to therapy (eg, IL-12/Interferon-gamma inhibition vs IL-6 inhibition).
Identify how rapidly glucocorticoids (GCs) can be tapered in LVV.
Identify if GC dosing based on body-weight or body surface area is superior to standard dosing.
Investigate the effect of MTX, tocilizumab, or other adjunctive therapies and combination therapy on the development of future vascular complications in LVV.
Investigate the optimal duration of treatment including tapering strategies and dosing (eg, higher MTX doses).
Investigate the value of conventional (eg, leflunomide), biological and other targeted DMARDs for treatment of all forms of LVV.
Investigate the role of anti-platelet therapy in LVV.
Investigate predictors of response to therapy in LVV.
C. Long-term outcome and biomarkers
Identify biomarkers which are independent of IL-6 (which could reflect response to anti-IL6 therapy).
Identify biomarkers to predict drug toxicity.
Identify predictors for good response, remission or relapse.
Investigate the value of screening for aortic dilatation regarding the prevention of complications (ie, aortic dissection or aortic ruptures).
Define and validate patient-reported outcomes in LVV.
Investigate the role of immunosuppressive agents in other forms of LVV such as isolated aortitis or IgG4 related periaortitis.
In conclusion, we substantially revised the original recommendations for the management of LVV. Despite progress over the past 10 years, we acknowledge that many recommendations are still consensus-based. However, despite the low-LoE, the level of agreement for each recommendation was consistently high among the task force members. We encourage clinicians to implement these recommendations into their clinical practice in order to effectively manage LVV and to improve the patients’ quality of care.
Acknowledgments
The authors wish to thank the librarians Chiara Rebuffi, Grant Office and Scientific Documentation centre, Fondazione IRCCS Policlinico San Matteo, Pavia, Italy and Helena Donato, Documentation Unit, Centro Hospitalar e Universitário de Coimbra, Coimbra, Portugal, for advice and assistance during the SLR.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Josef S Smolen
Correction notice This article has been corrected since it published Online First. The third affiliations has been updated and the author's names for Maria C Cid and Wolfgang Schmidt have been corrected.
Contributors AA and SM conducted the SLR. RL provided substantial methodological advice. BH drafted the first version of the manuscript and subsequent revisions. All authors were involved in the formulation and discussion of the recommendations, reviewed the manuscript and made extensive comments and changes to it. The final version of the manuscript was approved by all authors.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests EB received consultancies from Roche (payed to the University Medical Center Groningen). FB received grants from Horizon and Mundipharma and speaker fees and/or consultancies from Horizon, Mundipharma, Roche and Sanofi. HB received a grant and speaker fees from Roche. BD received consultancies and/or speaker fees from BMS, Chugai, GSK and Roche. CD received and grant from Celgene and speaker fees and/or consultancies from Abbvie, BMS, Lilly, MSD, Pfizer, Novartis, UCB, Roche and Sanofi. BH received speaker fees and/or consultancies from Abbvie, Boehringer, Chugai, Celgene, MSD, Pfizer, Novartis and Roche. SM received speaker fees and consultancies from Roche and Chugai. WS received a grant from Roche and speaker fees and consultancies from Chugai, GSG, Novartis, Roche and Sanofi. CT received a grant from BMS and speaker fees and/or consultancies from Abbvie, BMS, Pfizer and Roche. PV received a grant for conducting an RCT in GCA from Roche. All other authors have no competing interests.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.