Article Text

Abstract
Background: Fas mediated apoptosis may be important in the pathogenesis of primary Sjögren’s syndrome (pSS).
Objective: To examine genetic variation in the promoter region of the Fas gene in pSS.
Methods: Two single nucleotide polymorphisms at positions −1377(G/A) and −670(G/A) in the Fas gene promoter were genotyped by PCRSSP in 101 patients with pSS and 108 Caucasoid controls.
Results: No significant differences in allele or genotype frequencies were detected between the patients with pSS and controls. However, significant associations were observed with Ro/La autoantibody negative patients, who display milder and later onset disease. The −670A allele was more frequent in Ro/La autoantibody negative patients than in Ro/La autoantibody positive patients (p = 0.04).
Conclusion: This study does not confirm an earlier report of an association between pSS and the Fas promoter −670G allele. However, the results suggest that genetically determined variability in Fas expression may modulate Ro/La autoantibody responses in patients with pSS.
- Sjögren’s syndrome
- Fas
- polymorphism
- apoptosis
- CIE, counterimmunoelectrophoresis
- ELISA, enzyme linked immunosorbent assay
- pSS, primary Sjögren’s syndrome
Statistics from Altmetric.com
- CIE, counterimmunoelectrophoresis
- ELISA, enzyme linked immunosorbent assay
- pSS, primary Sjögren’s syndrome
Primary Sjögren’s syndrome (pSS) is a systemic autoimmune disease characterised by lymphocytic infiltration and failure of salivary and lachrymal exocrine glands. The cardinal symptoms of pSS are severe dryness of the eyes and mouth (sicca), and various extraglandular features are also frequently seen. The pathogenesis of pSS is not understood, but genetic, hormonal, and infectious factors have all been implicated. Diagnosis of pSS is aided by the finding in most patients of circulating autoantibodies specific for the intracellular Ro/La ribonucleoproteins, although a pathogenic role for these autoantibodies has not been demonstrated. Ro/La autoantibody subsets in pSS are associated with distinct clinical and genetic profiles.1,2
Apoptosis, or programmed cell death, is an important mechanism used to delete autoreactive lymphocytes and may be a key factor in the development of autoimmunity.3 MRL/lpr mice, characterised by a mutation of the gene encoding Fas, a mediator of apoptosis, exhibit pathological abnormalities in their salivary glands similar to pSS.4 In pSS, observations of increased expression of Fas, Fas ligand (FasL), and increased apoptosis in salivary gland epithelial cells have led to the proposal that abnormal apoptosis in exocrine glands may play a part in the observed exocrine gland destruction,5 although this remains controversial.6 Redistribution of the normally intracellular Ro and La autoantigens to surface membrane blebs on apoptotic cells has recently been demonstrated,7 a process by which these autoantigens may be accessible to the immune system. It is therefore conceivable that apoptosis may underlie the induction and facilitation of Ro/La autoantibody responses in pSS.
Two common single nucleotide polymorphisms in the promoter region of the Fas gene have been identified: −1377 G→A and −670 A→G.8 The biological effects of these polymorphisms have not been fully elucidated, but it is possible that they are of functional significance, as the Fas −1377 polymorphism occurs at the consensus binding sequence of the transcription factor SP-1 in the silencer region, and the −670 polymorphism occurs at the consensus sequence of the nuclear transcription element GAS (gamma interferon activation site) in the enhancer region.
We suggested that genetic variation in the promoter region of the Fas gene might influence apoptosis and thus the pathogenesis of pSS and Ro/La humoral autoimmunity. To examine this hypothesis, the two polymorphisms in the Fas promoter were genotyped in a cohort of patients with pSS and a group of ethnically matched Caucasoid controls.
PATIENTS AND METHODS
Patients and controls
One hundred and one patients fulfilling at least four of the six European classification criteria for pSS were studied.9 HLA-DRB1 typing, and both rheumatoid factor and IgG levels were tested routinely during clinical evaluation. Ro/La autoantibody screening was performed by counterimmunoelectrophoresis (CIE) and enzyme linked immunosorbent assay (ELISA) as previously described.1 The control group comprised 108 healthy South Australian volunteers to the Australian Bone Marrow Donor Registry.
Fas polymorphism genotyping
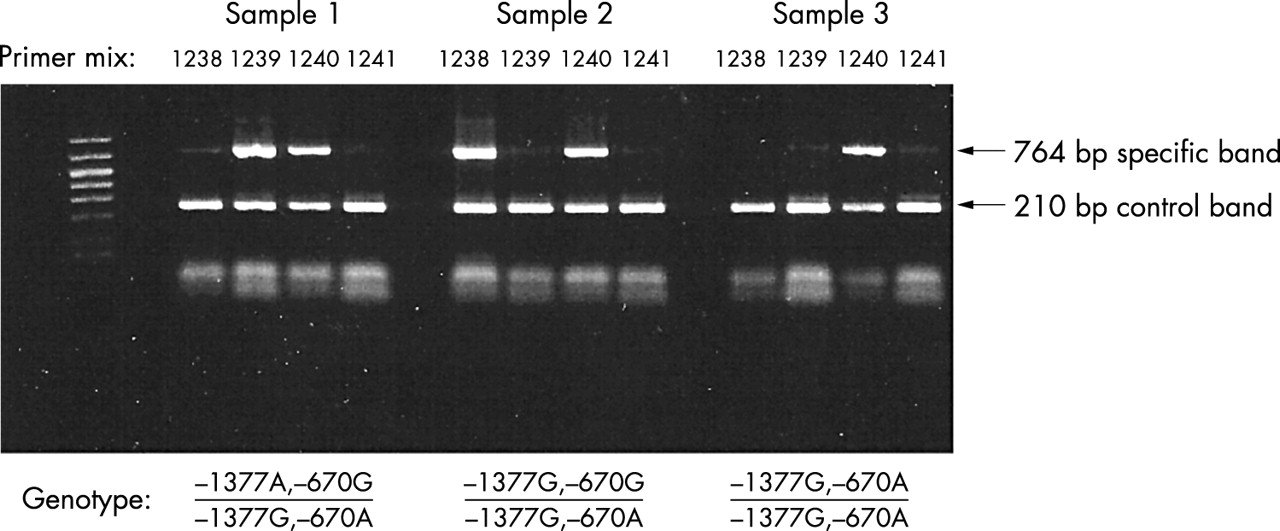
The −1377 G/A and −670 A/G single nucleotide polymorphisms in the promoter of the Fas gene8 were genotyped using the polymerase chain reaction and sequence specific primers. Four combinations of sense primers, specific for −1377 G/A, and antisense primers, specific for −670 G/A, were used to directly amplify cis haplotypic combinations (table 1, fig 1).
Primers and reaction mix composition for Fas promoter genotyping by haplotype specific PCR

{kind=link}
Fas promoter genotyping by haplotype specific polymerase chain reaction (PCR). Four haplotype specific PCR reactions (table 1) were used to amplify cis combinations of the Fas promoter −1377 and −670 polymorphisms. Genomic DNA was amplified in 13 μl reaction mixtures consisting of 67 mM Tris base pH 8.8; 16.6 mM ammonium sulphate; 2 mM magnesium chloride; 0.01% vol/vol Tween 20; 200 mM of each of dATP, dTTP, dGTP, and dCTP; 0.1–0.01 μg DNA; 3.4 mM haplotype-specific primers, 6.8 mM control primers; and 0.1875 units of Taq polymerase. Thermal cycling parameters were: 1 minute at 96°C; 5 cycles of 96°C for 25 seconds, 70°C for 45 seconds and 72°C for 45 seconds, followed by 21 cycles of 96°C for 25 seconds, 65°C for 50 seconds and 72°C for 45 seconds; followed by 4 cycles of 96°C for 25 seconds, 55°C for 60 seconds and 72°C for 120 seconds. PCR products were electrophoresed in 1.0% agarose gels containing 0.5 mg/ml ethidium bromide and visualised under ultraviolet illumination. Direction of electrophoresis is upward.
Statistics
Exact tests for Hardy-Weinberg equilibrium, linkage disequilibrium and comparisons of Fas promoter genotype and allele frequencies were performed using Arlequin version 2.000 (http://anthro.unige.ch/arlequin). Associations between Fas promoter genotypes and IgG levels and rheumatoid factor titres were analysed by Kruskal-Wallis analysis of variance, and interaction between Fas promoter genotypes and HLA by Ro/La autoantibody status was analysed by logistic regression. These analyses were performed using Statistica, version 6.1 (StatSoft, Inc).
RESULTS
Table 2 summarises the Fas promoter −1377 and −670 genotype distributions and allele frequencies. No significant differences were observed between patients with pSS (n = 101) and controls (n = 108).
Fas promoter polymorphism frequencies by Ro/La autoantibody status in patients with pSS v controls
Patients with pSS were stratified into four groups according to increasing Ro/La autoantibody diversification2: negative for anti-Ro/La autoantibodies (n = 23); anti-Ro only (n = 9); anti-Ro and non-precipitating (ppt−) anti-La (CIE negative, ELISA positive, n = 19); and anti-Ro and precipitating (ppt+) anti-La (CIE positive, n = 50). No significant differences were seen in the Fas promoter polymorphisms between the three Ro/La autoantibody positive groups. Further, no associations were observed between Fas promoter polymorphisms and rheumatoid factor titre or serum IgG levels. However, the Fas −670A allele frequency was significantly increased in patients with Ro/La autoantibody negative pSS compared with patients with Ro/La autoantibody positive pSS (p = 0.04, table 2). As expected,2 HLA-DR2 and DR3 frequencies were increased in Ro/La autoantibody positive patients (p = 0.01), but HLA-DR and Fas −670 polymorphism effects were independent (p = 0.68).
DISCUSSION
Apoptosis may be important in the development of autoimmunity3 and the Fas-FasL pathway is one of the mediators of apoptosis. This study examined associations between polymorphisms in the promoter of the Fas gene and pSS, a systemic autoimmune disease.
It has been proposed that abnormal apoptosis in the exocrine glands of patients with pSS may have a role in glandular destruction,5 although this remains controversial.6 We found no associations between Fas promoter −1377 and −670 polymorphisms and pSS. This suggests that modulation of apoptosis by genetic variation in the Fas promoter is unlikely to be important in salivary gland destruction in most patients with pSS, and highlights the uncertainty and controversy about the role of sialoepithelial apoptosis as an initiating event in the pathogenesis of pSS.
Associations between clinical and immunological abnormalities are well recognised features of pSS. Patients with Ro/La autoantibody negative pSS experience later onset, clinically milder disease with less glandular destruction.10 The Ro/La autoantibody categories used in this study represent stable subsets within a spectrum of diversification of Ro/La responses. This diversification appears to be largely under genetic control, and the HLA class II associations and clinical features of these autoantibody subsets have previously been reported.1,2 Because the normally intracellular Ro and La autoantigens are concentrated within surface blebs of apoptotic cells,7 a potential source of autoantigens, we suggested that Fas promoter polymorphisms may influence Ro/La autoantibody status in pSS. We found no differences in Fas −1377 or −670 promoter polymorphisms between the three Ro/La autoantibody positive pSS subgroups (table 2), but the −670A allele frequency was significantly increased in Ro/La autoantibody negative patients compared with Ro/La autoantibody positive patients (p = 0.04), an effect independent of HLA class II.
The Fas −670A allele has been implicated in other rheumatic diseases such as rheumatoid arthritis11 and systemic lupus erythematosus.12 There are two explanations for the observed association between the Fas −670A allele and Ro/La autoantibody negative pSS found in this study. Possibly, the level of activity of the Fas apoptotic pathway influences Ro/La autoantibody positivity independently of factors conferring disease susceptibility to pSS. Alternatively, patients with Ro/La autoantibody negative pSS may be a heterogeneous subgroup with differences in underlying pathogenesis.
Two prior studies have examined polymorphisms in the Fas gene in pSS. Bertolo et al reported no associations with coding polymorphisms, but the promoter was not examined.13 Bolstad et al reported a modest increase in the frequency of the −670G allele in Norwegian patients with pSS (not confirmed in this study of Australian patients with pSS), but associations with Ro/La autoantibody status were not investigated.14 This discrepancy between the two studies may be due to genetic differences between Australian and Norwegian populations, although the control group Fas promoter polymorphism frequencies were comparable. Alternatively, there may be differences between the pSS patient groups. Both studies used the same classification criteria for pSS,9 but only 33% of patients with pSS were positive for Ro/La autoantibodies in the Norwegian study compared with 77% in the current study.
In summary, we found no association between Fas promoter polymorphisms and pSS. Within patients with pSS, the −670A allele frequency was increased in those who were Ro/La autoantibody negative compared with Ro/La autoantibody positive patients, suggesting a possible protective effect of this allele on the development of Ro/La autoantibodies in patients with pSS. Evaluation of associations between Fas promoter polymorphisms and other less well characterised autoantibodies in pSS, such as anti-fodrin and anti-M3 muscarinic receptor, will be of potential interest, as these autoantigens also relocate to surface blebs during apoptosis.15 Other polymorphic genes which influence apoptosis include FasL, bcl-2, bcl-x, tumour necrosis factor receptor, tumour necrosis factor, and several other cytokines, and further study of the genetics of apoptosis in pSS is warranted.
Acknowledgments
Many thanks to the Arthritis Foundation of South Australia Lupus/Scleroderma/Sjögren’s Support Group and the patients with Sjögren’s syndrome who took part in this study. Many thanks to Dr Sara Marshall for provision of primer sequences for Fas genotyping.
REFERENCES
Footnotes
-
Support and financial interests: none.