Article Text

Abstract
Objective: To describe the treatment of polymyositis (PM) and dermatomyositis (DM) with prednisone (PRED) and cyclosporin A (CSA) alone or associated with intravenous immunoglobulin (IVIg) and plasmapheresis (PEX).
Methods: Between 1992 and 1999 CSA and PRED were used to treat 20 patients with idiopathic myositis (12 with DM, eight with PM), diagnosed according to the Bohan and Peter criteria. In patients with refractory or relapsed disease, IVIg was added alone (seven cases) or synchronised with PEX (six cases). A standardised protocol was used to evaluate the patients, and assess disease activity and treatment response.
Results: Despite a transient response to PRED and CSA in 16/20 cases, this combination did not induce full remission in 13/20 cases, which led to the IVIg trial with or without PEX. Patients receiving PRED and CSA plus IVIg had a significantly higher probability of maintaining complete remission at the end of the four year follow up period than those treated with PRED and CSA alone (p<0.001). No further benefit was added by the PEX. The presence of arthritis significantly correlated with a poorer response to treatment (p<0.05). Adverse effects were gingival hyperplasia (one patient) and transient renal dysfunction (one).
Conclusions: This open study suggests that combined treatment with PRED, CSA, and IVIg is useful in patients with myositis, even those with refractory or relapsed disease; no increase in the number or type of side effects is seen.
- polymyositis
- dermatomyositis
- cyclosporin A
- intravenous immunoglobulin
- plasmapheresis
- CK, creatine kinase
- CSA, cyclosporin A
- DM, dermatomyositis
- EMG, electromyography
- IVIg, intravenous immunoglobulin
- MRC, Medical Research Council
- PEX, plasmapheresis
- PM, polymyositis
- PRED, prednisone
- Tlco, carbon monoxide transfer factor
Statistics from Altmetric.com
- CK, creatine kinase
- CSA, cyclosporin A
- DM, dermatomyositis
- EMG, electromyography
- IVIg, intravenous immunoglobulin
- MRC, Medical Research Council
- PEX, plasmapheresis
- PM, polymyositis
- PRED, prednisone
- Tlco, carbon monoxide transfer factor
Polymyositis (PM) and dermatomyositis (DM) are systemic autoimmune diseases of unknown cause characterised by the chronic idiopathic inflammation of skeletal muscles. Their poor prognosis, with higher rates of morbidity and mortality, is usually related to the involvement of the pulmonary, cardiac, and gastrointestinal systems.1,2 Corticosteroids are usually considered the mainstay of treatment and represent the first line treatment. Immunosuppressive agents have been adopted in association with, or as an alternative to, steroids in patients with refractory myositis. We here describe our experience of treating PM and DM with prednisone (PRED) and cyclosporin A (CSA) alone or associated with intravenous immunoglobulin (IVIg) and plasmapheresis (PEX).
PATIENTS AND METHODS
Patient group
Between 1992 and 1999, we used three different CSA based regimens to treat 20 patients with primary idiopathic PM or DM according to the Bohan and Peter criteria.3
Entry parameters
The 20 patients had either PM (eight cases) or DM (12 cases). The disease was newly diagnosed in four patients. Nine patients were considered to have refractory disease because of the presence of (a) steroid dependency, as defined by the onset of clinical or laboratory flares when the steroid dose was reduced to less than 0.25 mg/kg/day (four cases); (b) steroid resistance, as indicated by non-responsiveness to high dose steroid treatment (at least 1 mg/kg/day for one month) (five cases). Relapse was defined as the recurrence of a previously quiescent disease despite previous treatment.
Measures of assessment
Muscle evaluation
Muscle evaluation was based on clinical, biochemical, and electromyographic (EMG) data. Changes in skeletal muscle strength were assessed with the Medical Research Council (MRC) scale, in which 0 is the lowest and 5 the highest score. We tested in each side the following muscle groups: deltoid, biceps brachii, triceps brachii, brachioradialis, wrist extensors, wrist flexors, iliopsoas, gluteus maximus, quadriceps femoris, and hamstring muscles, neck, finger and foot extensors and flexors. Among biochemical parameters, serum creatine kinase (CK) (normal values <170 U/l) levels were selected to detect variation in disease activity. Nerve conduction and concentric needle EMG studies were performed according to standard techniques.4 Fibrillation potentials (biphasic spikes or monophasic positive waves) and recruitment abnormalities were rated using commonly described methods.5 Motor unit potentials were evaluated on the basis of their duration, configuration, and amplitude by means of a trigger and delay line using a Nicolet Viking IV. At study entry, active myositis was ascertained on the basis of the MRC grade, CK levels, and EMG myopathic changes. During the study, MRC and CK were detected every three months or at any time they were clinically indicated. EMG was repeated each six months, or when clinically indicated.
Skin and internal organ system evaluation
The type and extent of skin lesions were evaluated. The specific investigations undertaken included in all cases pulmonary function, the diffusion capacity of the lung for carbon monoxide expressed as a percentage of the predicted value (Tlco), and chest radiography. High resolution computed tomography was performed in four patients with reduced Tlco. Other examinations, such as oesophageal motility, were carried out when clinically indicated.
Treatment
All potentially eligible patients were treated with PRED and CSA. Oral PRED was started at 1 mg/kg/day and then slowly tapered to an average of 0.25 mg/kg every other day. CSA was given at an initial oral dose of 3 mg/kg/day for six months, subsequently reduced to a maintenance dose of 2 mg/kg/day.
Seven patients (group I) received only PRED and CSA as first line treatment (four cases) or in the case of steroid refractoriness (three cases).
In group II, IVIg was chosen to treat relapsed or refractory disease in respectively five and two cases. IVIg was infused at 1 g/kg/day (5 g/h) on two consecutive days each month for six months, followed by three further cycles given every other month.
In six other patients (group III), synchronised treatment with PEX-IVIg was added to the CSA/steroid regimen to treat relapsing (two case) or refractory (four cases) disease. The PEX sessions were performed on days 1, 3, and 5, followed by IVIg infusion (as above) on days 6 and 7. The treatment was repeated monthly for six months, followed by three further cycles administered every other month.
In all groups, the first treatment period lasted one year. Thereafter, patients who had improved received no treatment or a minimum steroid dosage to maintain remission. Patients who did not respond to the treatments described above were given other cytotoxic drugs.
Outcome measures
As working definition, the response to treatment was evaluated as follows:
Complete remission: an increase in strength of at least one more MRC point in at least three affected muscles with normal CK levels. In patients with a normal CK level at study entry, besides the MRC value, we decided to use the absence of the pathological EMG spontaneous activity.
Partial remission: when only one of the above criteria was satisfied.
Relapse: disease reactivation after a remission lasting six months or more.
A patient was considered as “improved” in the case of a complete or partial remission, and “not improved” in the case of unchanged, worsened, or reactivated disease.
The type and severity of any adverse events were recorded.
Statistical analyses
The data collected in the clinical charts of the 20 patients were analysed using the NCSS statistical programme.6 Data are expressed as median (SD). For between-group comparison the Mann-Whitney test was used. Comparison between frequencies was performed by χ2 analysis and Fisher's exact test, when indicated. Significance was defined as a p value <0.05.
RESULTS
Baseline characteristics
Table 1 shows that the demographic and clinical characteristics of the patients were similar in the different treatment groups. In all cases the median values of CK levels, MRC grade, and EMG myopathic changes were consistent with a diagnosis of active myositis. The median follow up of the patients as a whole was four years.
Baseline characteristics of 20 patients with PM/DM treated with PRED and CSA alone (group I) or associated with IVIg (group II) or with PEX-IVIg (group III). Data are expressed as median, see “Patients and methods” for details
Response to treatment
From the first months of treatment, the clinical status and the strength gradually recovered, with an improvement of the MRC and CK values between months 3 to 6 in group I and between months 1 and 3 in groups II and III (fig 1) with no differences between DM or PM. At the end of the one year treatment period, five of the patients in group I showed a partial response, one was in complete remission, and one relapsed eight months after the start of treatment. In groups II and III, partial (n=4 and n=4, respectively) and complete remission (n=3 and n=2, respectively) were seen in all patients (fig 2). Subsequent long term evaluation showed that positive results were maintained almost exclusively in groups II and III. In group I, one patient was in clinical and functional remission 19 months after the start of treatment; the other cases maintained a partial remission. All of the patients in group II and 5/6 patients in group III improved; in this latter group only one patient relapsed (fig 2).

Median serum CK levels over time in the 20 patients with PM/DM treated with PRED and CSA with or without IVIg associated or not with PEX.
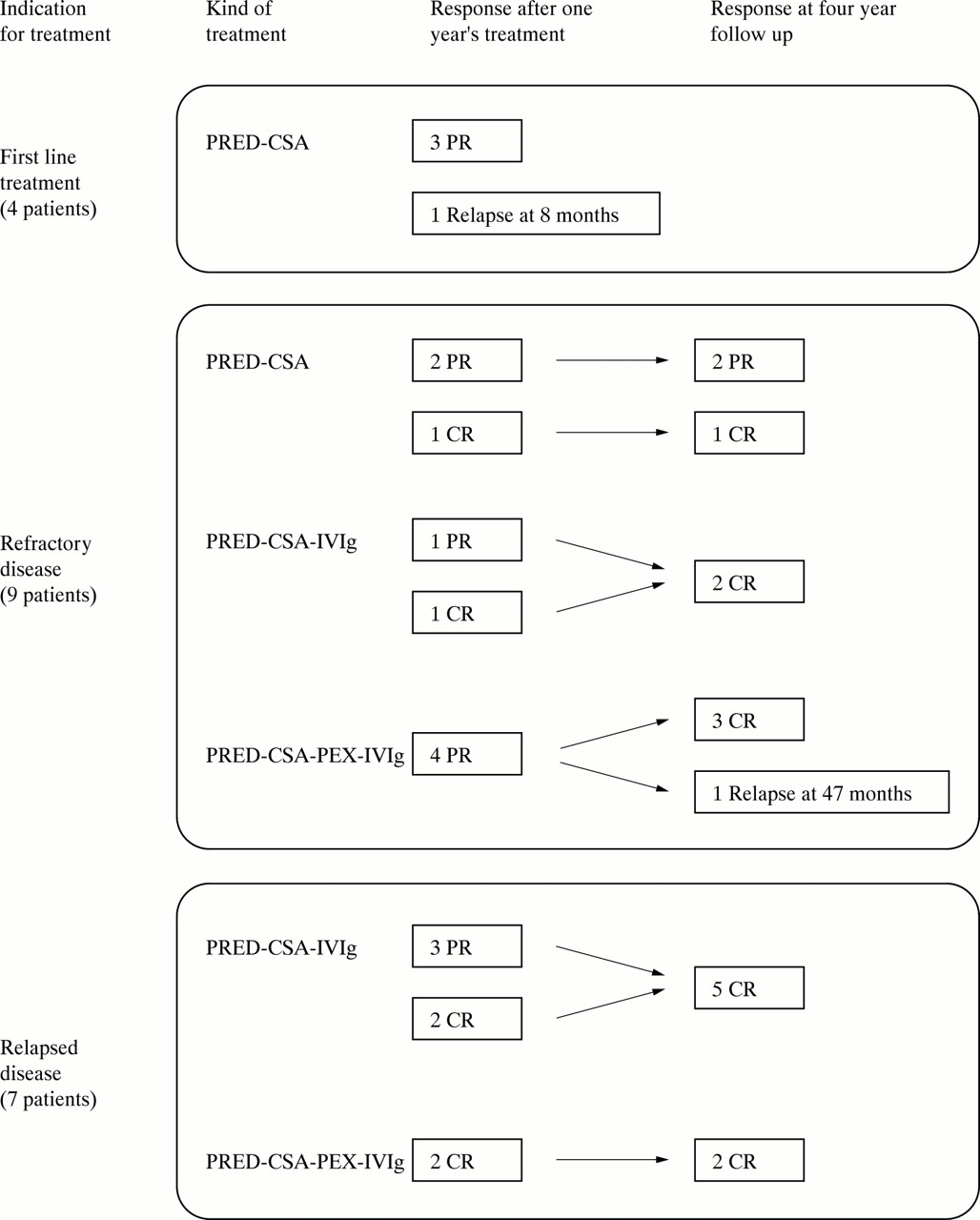
Outcomes of 20 patients with PM/DM treated with PRED and CSA with or without IVIg associated or not with PEX. CR, complete remission; PR, partial remission.
Statistical analyses
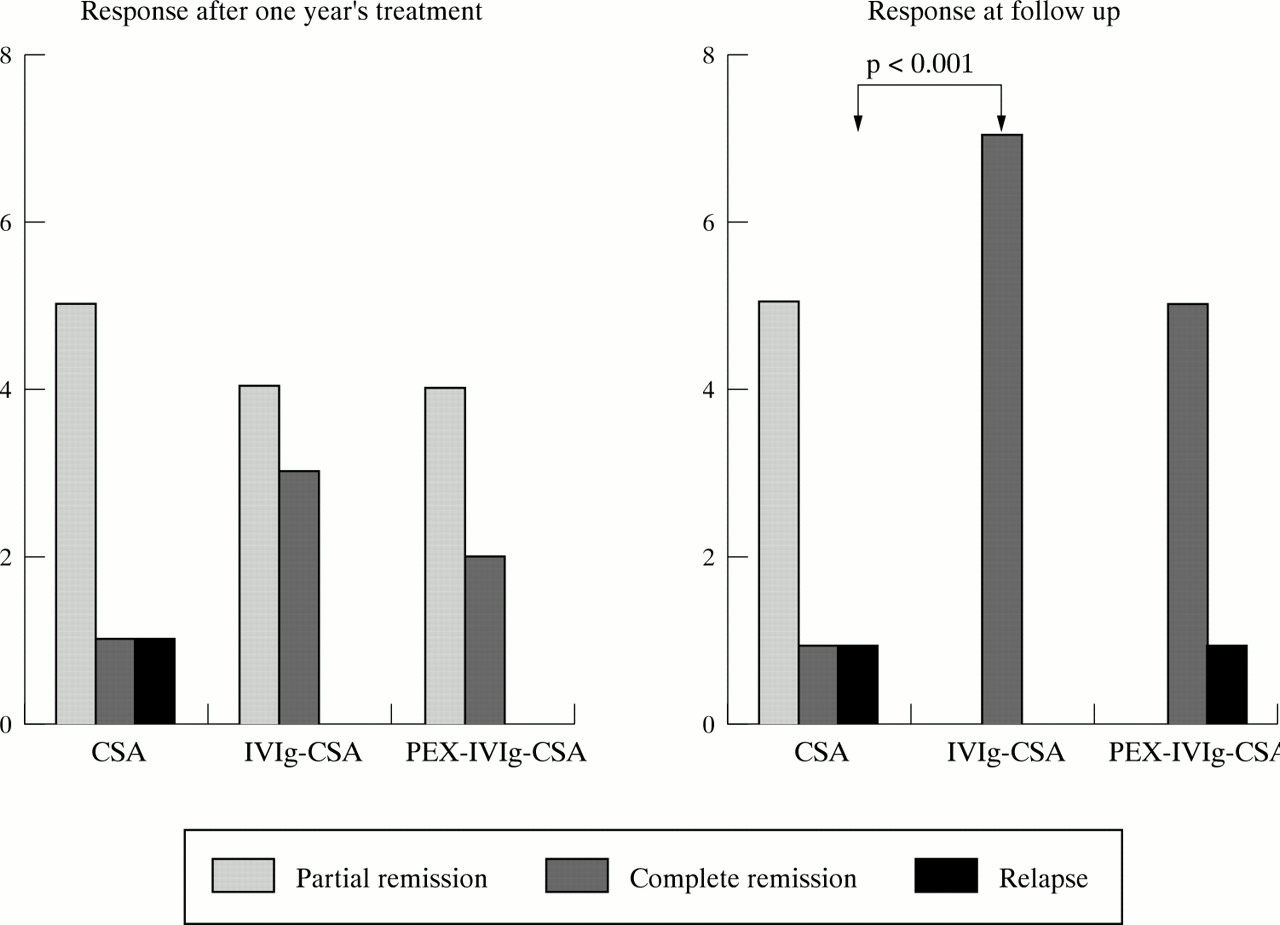
At the end of the one year period of treatment no statistical difference was found between the three treatment groups. A highly significant difference was seen at the end of the follow up period between the steroid-CSA-IVIg regimen, which achieved the best results, and the steroid-CSA protocol (p<0.001, χ2) (fig 3).

{kind=link}
{kind=link}
{kind=link}
Outcomes of 20 patients with DM/PM at the end of the treatment period (one year) and at the end of follow up (median four years). Patients receiving PRED and CSA plus IVIg had a significantly higher probability of maintaining complete remission at the end of the follow up period than those treated with PRED and CSA alone (p<0.001). No further benefit was added by the PEX.
Among six patients with arthritis, four had a poor outcome, whereas among 14 without arthritis only three had a poor outcome (p<0.05), independently from the treatment. We could not detect any other correlation between the response to treatment in the three groups and other variables such as the kind of myositis (DM or PM), the sex of the patient, and the type of other organ affected.
Side effects
No new or major side effects were recorded during the trial. The minor events included mild gastrointestinal intolerance (nausea or vomiting), gingival hyperplasia, transient increase in serum creatinine, and hypotensive episodes during the apheresis sessions (one case each).
DISCUSSION
The treatment of PM and DM is still a matter of debate. Only a few well designed studies have been published and, to the best of our knowledge, only four randomised controlled trials.7–10 There is general agreement about the use of steroids as first line treatment for patients with newly diagnosed disease, but steroids are associated with high rates of recurrence and morbidity.2 The introduction of immunosuppressive agents is usually considered if the disease is refractory to steroids or rapidly progressive, or if a patient develops severe systemic involvement.11
Many studies and case reports have indicated the efficacy of CSA in refractory myositis10,12–19 at doses of between 3 and 10 mg/kg/day, with outcome parameters of clinical improvement, normalisation of serum muscle enzymes, and steroid sparing. No serious side effects are generally described, but 8–15% of patients develop arterial hypertension, hypertrichosis, tremor, and transient renal dysfunction.19 Two retrospective studies of respectively 1015 and 1217 patients have suggested the efficacy of CSA as a valid second line treatment in refractory DM. Two other reports described the efficacy of CSA in treating interstitial lung disease in myositis, particularly when used early.18,20 To the best of our knowledge, only one randomised controlled trial10 has evaluated the use of CSA in the treatment of PM and DM: the comparison between CSA and methotrexate did not show any significant difference between the two drugs in the six month efficacy and toxicity, and confirmed the reliability of both drugs in the treatment of myositis.
We have treated 20 patients with idiopathic myositis. In nine cases, the disease was considered refractory because of the presence of steroid dependency or steroid resistance. Another seven patients experienced a relapse during previous treatment. We used a standardised protocol to evaluate the patients, and assess disease activity and treatment response. The patients in group I received only PRED and CSA; in the other two groups, CSA was associated with IVIg or synchronised PEX with subsequent IVIg. The patients who received high dose IVIg (with or without PEX) were those with more active disease and/or in whom conventional treatment had failed. We recorded a transient response to CSA and PRED in 16/20 (80%) cases, and needed to use an add on treatment with IVIg (with or without PEX). The combination of CSA and IVIg (with or without PEX) seems to assure a longer disease-free period and to be more beneficial than CSA alone, thus confirming the preliminary report of Saadeh et al.16 Our data at long term follow up reinforce these results, with a highly statistically significant difference detected at the end of the follow up period. Moreover, the trend towards normalisation of the MRC and CK values was more evident from the first months of treatment in the group treated with IVIg (with or without PEX), independently of the kind of the myositis. We found no increase in the number or type of side effects.
It is difficult to distinguish the benefits of CSA and IVIg.21 In a double blind, placebo controlled, randomised crossover trial, Dalakas et al found significant but transient results in patients with DM treated with IVIg.8 As for PM, only uncontrolled studies have been reported.22,23 The efficacy of IVIg was demonstrated in 14 patients followed up by Cherin et al24 and in a group of patients by Mastaglia et al.25 In a prospective study, this successful trend has been confirmed by the long term follow up analysis in 70% of 35 patients with chronic refractory PM.26 The same group, however, did not find a clear benefit for IVIg as first line treatment in patients with inflammatory myopathy (PM or DM).27 Despite the difference in the value and in the rationale of the use of IVIg in PM and in DM,22,28 in our group of patients we found no difference between the kind of myositis and the response to treatment. More studies are necessary to confirm the reliability of continuing IVIg treatment, as suggested by our data.
The benefit of PEX is still uncertain and the results of various studies are discordant. In 1981, Dau et al initially reported the efficacy of PEX associated with immunosuppressive drugs in 74% of corticosteroid resistant patients with PM/DM.29 However, a double blind, placebo controlled trial failed to demonstrate the efficacy of PEX and leukapheresis in chronic refractory PM/DM.7
In our series the steroid-CSA-IVIg regimen gave the best and statistically significant results as compared with steroid-CSA based treatment. We acknowledge in our study the retrospective design, the lack of randomisation, and the small number of patients enrolled, all related to the infrequency of the conditions studied. Despite these biases, longitudinal and statistical analysis suggests the long term efficacy of a combination treatment with prednisone, CSA, and IVIg in patients with PM/DM, including those with refractory or relapsed disease.
Acknowledgments
We are deeply grateful to Ornella Della Casa-Alberighi, MD, for helping to review the manuscript.