Article Text

Abstract
Objective: To analyse the performance of a new M tuberculosis-specific interferon γ (IFNγ) assay in patients with chronic inflammatory diseases who receive immunosuppressive drugs, including tumour necrosis factor α (TNFα) inhibitors.
Methods: Cellular immune responses to the M tuberculosis-specific antigens ESAT-6, CFP-10, TB7.7 were prospectively studied in 142 consecutive patients treated for inflammatory rheumatic conditions. Results were compared with tuberculin skin tests (TSTs). Association of both tests with risk factors for latent M tuberculosis infection (LTBI) and BCG vaccination were determined and the influence of TNFα inhibitors, corticosteroids, and disease modifying antirheumatic drugs (DMARDs) on antigen-specific and mitogen-induced IFNγ secretion was analysed.
Results: 126/142 (89%) patients received immunosuppressive therapy. The IFNγ assay was more closely associated with the presence of risk factors (odds ratio (OR) = 23.8 (95% CI 5.14 to 110) vs OR = 2.77 (1.22 to 6.27), respectively; p = 0.009), but less associated with BCG vaccination than the TST (OR = 0.47 (95% CI 0.15 to 1.47) vs OR = 2.44 (0.74 to (8.01), respectively; p = 0.025). Agreement between the IFNγ assay and TST results was low (κ = 0.17; 95% CI 0.02 to 0.32). The odds for a positive IFNγ assay strongly increased with increasing prognostic relevance of LTBI risk factors. Neither corticosteroids nor conventional DMARDs significantly affected IFNγ responses, but the odds for a positive IFNγ assay were decreased in patients treated with TNFα inhibitors (OR = 0.21 (95% CI 0.07 to 0.63), respectively; p = 0.006).
Conclusions: These results demonstrate that the performance of the M tuberculosis antigen-specific IFNγ ELISA is better than the classic TST for detection of LTBI in patients receiving immunosuppressive therapy for treatment of systemic autoimmune disorders.
Statistics from Altmetric.com
Therapeutic blockade of tumour necrosis factor α (TNFα) has emerged as an effective treatment in chronic inflammatory diseases such as rheumatoid arthritis, ankylosing spondylitis, or Crohn’s disease. However, patients undergoing TNFα inhibition are at increased risk of developing serious infections.1–4 In particular, the incidence of life-threatening extrapulmonary and disseminated tuberculosis, resulting from reactivation of latent Mycobacterium tuberculosis infection (LTBI), is increased in patients treated with anti-TNFα antibodies.5–7 Therefore, screening of patients for LTBI before the start of TNFα inhibition has become essential. However, diagnosis of LTBI is problematic, especially in the presence of immunosuppressive therapy, since neither targeted imaging techniques nor tuberculin skin tests (TSTs) are sufficiently accurate.8–10 The TST, which aims at eliciting an antigen-induced intradermal cellular immune response makes use of common mycobacterial cell components. This test therefore lacks specificity for pathogenic M tuberculosis complex strains such as M tuberculosis. Either prior exposure to environmental mycobacteria and prior vaccination with Bacille Calmette-Guérin (BCG) can both lead to false-positive TST results.11
The discovery of the immunogenic mycobacterial proteins ESAT-6, CFP-10, and TB-7.7, all of which are specifically expressed by pathogenic M tuberculosis complex strains, has paved the way for the development of more specific diagnostic assays for LTBI.12 Recently, two such tests, an enzyme linked immunosorbent assay (ELISA), QuantiFeron, and an enzyme linked immunospot (ELISPOT) assay, T-SPOT, have been approved by the Food and Drugs Administration. Both assay systems measure antigen-specific interferon γ (IFNγ?) secretion by peripheral blood CD4+ T lymphocytes in response to in vitro stimulation with ESAT-6, CFP-10, and TB7.7 peptides. A number of studies carried out in non-immunosuppressed subjects have already demonstrated that compared with the TST the new IFNγ assays are not affected by cross-reactivity with BCG or environmental mycobacteria, and correlate better with exposure to M tuberculosis.12–17
The objective of this prospective study was to compare an M tuberculosis-specific IFNγ ELISA (QuantiFeron TB-Gold In Tube, Cellestis Limited, Carnegie, Australia) with a classic TST for detection of LTBI in patients with chronic inflammatory conditions, who receive immunosuppressive drugs, including TNFα inhibitors.
PATIENTS AND METHODS
Patients
Consecutive patients treated for chronic inflammatory conditions at our rheumatological outpatient clinic at the University Hospital of Berne, Switzerland were prospectively enrolled. The study was approved by the local research ethics committee. All patients gave their written informed consent. Demographic information and data on BCG vaccination status, treatment regimens and risk factors for latent tuberculosis were collected on a standardised electronic form from vaccination cards, medical records, chest x ray results and standardised patient interviews, without knowledge of results of the TST or ELISA test. We distinguished between systemic corticosteroids, conventional disease modifying antirheumatic drugs (DMARDs) (including methotrexate, azathioprine, ciclosporin, leflunomide, cyclophosphamide, hydroxychloroquine, sulfasalazine, mycophenolate mofetil or sirolimus) and TNFα inhibitors (infliximab, etanercept or adalimumab). The following characteristics were considered risk factors for latent tuberculosis18 and ranked a priori according to their prognostic relevance from least to most relevant: born or resident for ⩾6 months in a country with a tuberculosis prevalence >20 cases per 100 000 inhabitants; a history of household tuberculosis contact; chest x ray findings suggestive of a history of tuberculosis (eg, calcified granuloma or apical densities); or a medically confirmed history of active tuberculosis. Ranking of risk factors for LTBI was prespecified before the start of patient recruitment and was based on clinical expertise and the estimated probability that a risk factor is associated with latent M tuberculosis infection.
Interferon γ ELISA and TST
Technicians, who were unaware of the patient characteristics and results of the TST, performed a whole blood IFNγ ELISA, which is based on the M tuberculosis-specific peptides ESAT-6, CFP-10 and TB7.7 antigens (QuantiFeron TB-Gold In Tube, Cellestis Limited, Carnegie, Australia) at our rheumatology laboratory, according to the manufacturer’s instructions.
The assay involves two stages, the incubation of whole blood with antigens, and the measurement of the IFNγ production in harvested plasma by ELISA. We directly collected peripheral venous blood into each of three 1 ml heparin-containing tubes. One tube contained only heparin as negative control, the second also contained the T-cell mitogen phytohaemagglutinin (PHA) as positive control and the third contained overlapping peptides representing the entire sequences of ESAT-6 and CFP-10, and another peptide representing a portion of TB7.7. Test tubes were vigorously shaken for 5–10 seconds, and incubated at 37°C within 2 hours in a cell culture incubator with 5% CO2 atmosphere. After 24 hours of incubation, sample tubes were centrifuged and plasma was snap frozen in liquid nitrogen, harvested and stored at –80°C until ELISA for IFNγ measurement was performed. The IFNγ values for tuberculosis-specific antigens and positive control were corrected for background by subtracting the value obtained for the respective negative control. In accordance with the manufacturer’s recommendations and previous studies,14 15 19 the test was considered positive if the concentration of IFNγ for tuberculosis-specific antigens was ⩾0.35 IU/ml, irrespective of the result of the positive control; negative, if the concentration of IFNγ for tuberculosis-specific antigens was <0.35 IU/ml and the concentration for the positive control was ⩾0.5 IU/ml; and indeterminate, if the concentration of IFNγ was <0.35 IU/ml for tuberculosis-specific antigens and <0.5 IU/ml for the positive control.
At our outpatient clinic, patients with chronic inflammatory conditions routinely undergo a TST according to the Mantoux method by trained nurses. Nurses were unaware of the patient characteristics and results of the IFNγ assay. A 2 TU dose (0.1 ml) of tuberculin purified protein derivative (PPD RT23; Staten Serum Institut, Copenhagen, Denmark) was injected intracutaneously and the main diameter of the skin induration was recorded 48–72 hours after inoculation. In accordance with current guidelines for immunosuppressed patients,18 a diameter of >5 mm was considered positive. The local research ethics committee allowed tuberculin skin testing only as part of routine clinical procedures. Therefore, we were unable to ascertain results, if a TST had not been performed as part of clinical routine within 6 months before the inclusion of patients into the study.
Statistical analysis
In the absence of a “gold standard” for the diagnosis of LTBI, we were unable to determine directly the sensitivity and specificity of the IFNγ assay.20 Instead, we compared the performance of the IFNγ assay and the TST in relation to the presence of risk factors for latent tuberculosis and BCG vaccination status. If the IFNγ assay were more sensitive and specific than the TST, it should be associated more closely with the presence of risk factors than the TST.17 In addition, if the IFNγ assay were less influenced by BCG vaccination status than the TST it should be associated less with BCG vaccination than the TST.17 To determine the strength of associations, we calculated odds ratios, which are a function of both, sensitivity and specificity.21 The odds ratio increases as one or both of sensitivity and specificity increase.
In the primary analysis, we determined the association of IFNγ assay and TST results with the presence of any risk factor and BCG vaccination status separately in univariable logistic regression models. In a secondary analysis, we included the presence of any risk factor and BCG vaccination status simultaneously as independent variables in a multivariable model. Then, we performed tests for trend across individual risk factors for latent tuberculosis ranked a priori according to their prognostic relevance, using the χ2 statistic. If a contingency table had a cell with no events, we calculated odds ratios and 95% CIs by adding 0.5 to all cells. To calculate p values for differences in performance between tests, we used matched-pairs logistic regression, which accounted for the correlation between IFNγ assay and TST results within patients.17 Then we used κ statistics to determine agreement between the IFNγ assay and TST results greater than that expected by chance.22
To determine whether the type of treatment was associated with a decreased probability of positive results of TST and IFNγ assay, we used univariable and multivariable linear or logistic regression models, with corticosteroids, conventional DMARDs and TNFα inhibitors as independent variables. In sensitivity analyses specified post hoc, we included the type of diagnosis in the models, considered birth or residence in a high-prevalence country not to be risk factor for latent tuberculosis, adjusted tests for trend for the presence or absence of TNFα inhibitors and stratified the analysis of the association between the presence of risk factors for latent tuberculosis or BCG vaccination status and test results by the presence or absence of TNFα inhibitors. Finally, we used multivariable linear regression models to determine the association of the type of treatment with the concentration of IFNγ for the positive control. All reported p values are two sided. All analyses were performed with STATA, version 9.2 (Stata, College Station, TX, USA).
RESULTS
One hundred and forty two consecutive patients with chronic inflammatory rheumatic conditions were included in the study (fig 1). Table 1 shows their characteristics.

TST results were obtained for 115 patients, data on BCG vaccination status and risk factors were available for all patients. Forty-four patients (31%) had risk factors for latent tuberculosis, 118 patients were BCG vaccinated (83%) and 126 patients received TNFα inhibitors, conventional DMARDs, or corticosteroids (89%). Eighty-four patients (59%) received TNFα inhibitors. Of these, 64 additionally received at least one DMARD, and 25 additionally received corticosteroids. Among TNFα inhibitors, infliximab was used in 78, etanercept in four and adalimumab in two patients. The most commonly used conventional DMARD was methotrexate (70 patients, 49%), in combination with TNFα inhibitors (46 patients), in combination with corticosteroids (17 patients), another DMARD (three patients) or as a single agent (four patients). Chemoprophylaxis for tuberculosis was given to 17 patients. The median time between performing the TST and the IFNγ assay was 102 days (range 7–184). Characteristics of patients remained unchanged over this time. However, TNFα inhibition was initiated after results of TST became available and before the IFNγ assay was performed.
Low rate of indeterminate results for the IFNγ ELISA in immunosuppressed patients
The IFNγ assay was indeterminate in 8/142 tested patients (6%)—7/126 immunosuppressed patients (6%), and 1/16 patients (6%) who received no immunosuppressive drugs. Only one patient was treated with a TNFα inhibitor. Accordingly, we found no evidence for an increased risk of indeterminate results associated with the use of TNFα inhibitors; rather, the odds ratio (OR) from multivariable logistic regression was below one (OR = 0.07, 95% CI 0.01 to 0.69, p = 0.022). However, in multivariable linear regression we found that treatment with TNFα inhibitors was associated with a decreased concentration of IFNγ for positive control (−8. IU/ml, 95% CI –12.1 to –4.5 IU/ml, p<0.001). No clear trends emerged for conventional DMARDs or corticosteroids, either in logistic or in linear regression (p⩾0.20).
Comparative performance of IFNγ assay and TST
Among the 109 patients for whom results for both tests were available, there was a 64% concordance between the two tests (see fig 1 for a breakdown of test positive and negative results according to the type of the test), while the agreement expected by chance alone was 57%. Accordingly, the κ statistic for the agreement between the two tests was low (κ = 0.17, 95% CI 0.02 to 0.32).
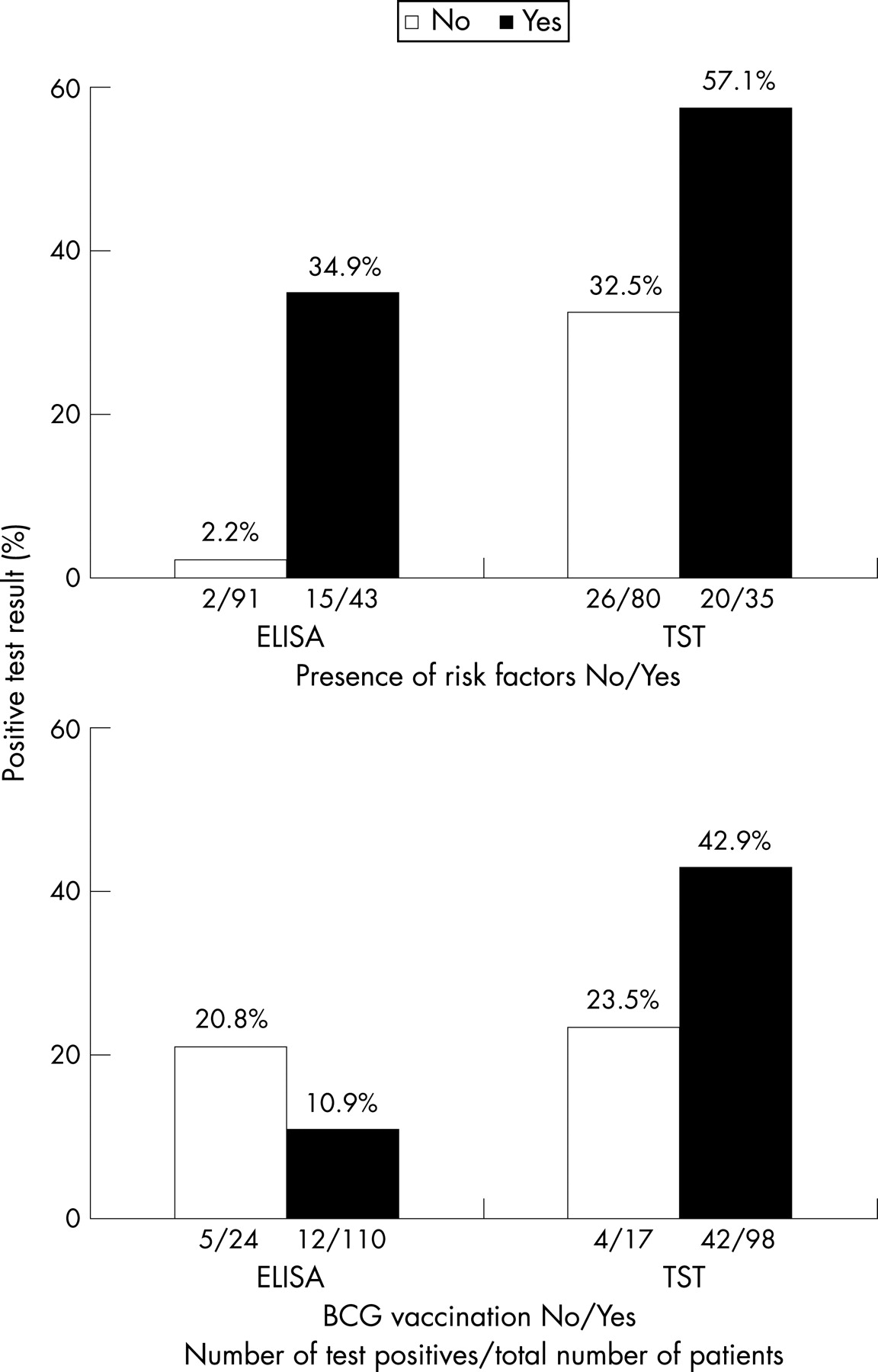
Figure 2 presents results of the IFNγ ELISA test and TST according to the presence or absence of risk factors for LTBI and BCG vaccination status. Table 2 shows the association between the presence of risk factors for LTBI or BCG vaccination and results of ELISA and TST from logistic regression analyses.
{kind=link}
{kind=link}
In patients with risk factors for latent tuberculosis, compared with patients without a risk factor, the odds of a positive IFNγ assay from univariable logistic regression was increased by a factor of 23.8. In comparison, the odds for a positive TST was increased by a factor of 2.8. The IFNγ assay was associated more closely with the presence of risk factors than the TST (p for difference in performance between tests = 0.009). Conversely, the IFNγ ELISA was associated less with previous BCG vaccination than the TST (p for difference in performance between tests = 0.025).
Results from multivariable analysis (table 2) were similar to univariable analysis. However, differences in performance between the two tests reached conventional levels of statistical significance only for the presence of risk factors, and not for BCG vaccination status. We found similar results when including the type of diagnosis in the models (data available on request). When birth or residence in high-prevalence country were not considered to be risk factors for latent tuberculosis, the association between IFNγ assay and risk factors was slightly attenuated ORs of 17.1 and 16.3 with p<0.0001 in uni- and multivariable analysis, respectively), while remaining results were unchanged (data available on request).
Table 3 presents the increase in odds for a positive test for individual risk factors ranked according to their prognostic relevance compared with the presence of no risk factors.
There was a clear-cut trend for an increase in odds with increasing relevance of risk factors for the IFNγ ELISA (p value for trend <0.001), but not for TST (p value for trend = 0.13). The difference in performance between the IFNγ assay and the TST across ordered groups was significant (p<0.001). When adjusting for the presence or absence of TNFα inhibitors, the test for trend remained unaffected (p value for trend <0.001).
Association between results of tests and drug regimen
Table 4 presents the association between results of the tests and the drug regimen from univariable and multivariable analysis. For the TST, the odds for a positive test were increased in patients with risk factors and in patients with BCG vaccination. For the IFNγ test, uni- and multivariable analyses indicated that the odds for a positive test were significantly increased in patients with risk factors (p<0.001), and significantly decreased in patients undergoing treatment with TNFα inhibitors (p = 0.006 and 0.019, respectively).
Supplementary Table 1 (available at http://ard.bmj.com/supplemental) presents the association between the presence of risk factors for latent tuberculosis or BCG vaccination status and results of the two tests in patients with and without TNFα inhibitors. Even though TSTs were performed when none of the patients had undergone treatment with TNFα inhibitors, associations between TST and risk factors or BCG vaccination status tended to be less pronounced in those who subsequently underwent treatment with TNFα inhibitors, but confidence intervals overlapped widely. Associations between the results of the IFNγ test and risk factors tended to be more pronounced in patients who had not received treatment with TNFα inhibitors, but, again, confidence intervals overlapped widely.
DISCUSSION
Reliable tests to detect LTBI are needed by rheumatologists treating patients with TNFα-blocking drugs as such patients are at increased risk of reactivation of LTBI and development of disseminated and extrapulmonary tuberculosis.5–7
In the absence of a “gold standard” for the diagnosis of LTBI, it is impossible to directly determine the sensitivity and specificity of any new diagnostic test for LTBI.21 Therefore we determined the comparative performance of the IFNγ ELISA and the TST in relation to the presence or absence of risk factors for LTBI, and in relation to the BCG vaccination status. Our study shows that, in contrast to the TST, results of the IFNγ ELISA are significantly associated with the presence of LTBI risk factors. Furthermore, BCG vaccination affects the TST but not the IFNγ ELISA. Therefore our study shows that the IFNγ ELISA has a better diagnostic performance than the TST in immunosuppressed rheumatic patients.
Although we found no consistent pattern indicating that any of the immunosuppressive drugs used in the patients were associated with an increased risk of indeterminate results, patients receiving TNFα inhibitors were less likely to have a positive IFNγ assay. True negative testing as a result of appropriate evaluation and treatment of these patients before initiation of TNFα inhibitors may explain this association. However, the relevant decrease in the mitogen-induced IFNγ response in patients treated with TNFα inhibitors makes false negative testing a more plausible explanation. Consistent with this notion, TNFα inhibitors were recently shown to inhibit the activation of CD4+ T lymphocytes by mycobacterial antigens.23
We prospectively enrolled consecutive patients treated for chronic inflammatory conditions at our rheumatological outpatient clinic and used blinding of those interpreting test results. These measures should decrease biases that might result in an overestimation of test performance.24 We carefully determined risk factors for latent tuberculosis and BCG vaccination status and used appropriate statistical methods to compare the performance of the IFNγ assay with TST in the absence of a “gold standard”.17 The major limitation of the study is that results of the TST were available in about 80% of patients only. In addition, the relatively small number of patients meant that we were unable to explore the association between type and dosage of drug regimens and IFNγ secretion in more detail.
The agreement between the IFNγ assay and TST was lower than in previous studies.13–15 17 25 26 This discrepancy may be partially explained by differences in performance between the ELISA test used in our study and the ELISPOT test used in some other studies.17 26 It is also possible that the IFNγ assay and the TST perform differently in patients with chronic inflammatory conditions undergoing treatment with TNFα inhibitors, conventional DMARDs or corticosteroids as compared with healthier people included in other studies.14 17 In addition, the high BCG vaccination rate of 83% in our patients will have led to an increase in false-positive TST results. Two methodological aspects deserve additional attention: first, TST tests were not performed simultaneously with the IFNγ assay. Changes in drug regimens over time might therefore have contributed to the observed discrepancies between the two tests. However, when distinguishing between those who had received a TNFα inhibitor after the TST, but before the IFNγ assay, and those who had continued to follow a stable drug regimen in a stratified analysis, we found our results confirmed. Second, we followed current guidelines for immunosuppressed patients18 and considered a diameter of the skin induration of >5 mm to indicate a positive TST. This might have increased the rate of false-positive TST results.
Another group using the same IFNγ assay25 26 found higher rates of indeterminate results than we did, particularly in patients with cancer undergoing chemotherapy.25 The lower rate of indeterminate results in our study might be explained by immunomodulation rather than immunosuppression achieved by the low to moderate doses of the drug regimens used in our rheumatic patients. Another reason may be that vigorous shaking of test tubes and careful incubation resulted in more reliable exposition to antigens and lower rates of indeterminate results.
The decrease in the IFNγ response for the positive control associated with TNFα inhibitors is in accordance with a recent study in HIV patients, which found a reduced IFNγ release in the positive control in patients with low CD4 T-cell counts.27 Compared with the ELISA test used in our study, the IFNγ ELISPOT test was previously reported to have lower rates of indeterminate results.26 These differences may, among other reasons, be explained by differences in the concentrations of the mitogen PHA between the two test systems. The PHA concentration used in the positive control of the ELISA test is titrated by the manufacturer to yield 25% of the maximal IFNγ response in healthy donors. Higher PHA concentrations are expected to result in stronger stimulation and hence a decrease in the rate of indeterminate results. However, since unspecific PHA stimulation of T lymphocytes differs both qualitatively and quantitatively from stimulation by M tuberculosis-specific peptides, the increase in PHA concentrations to lower the rates of indeterminate results will not itself lead to a more accurate test: T lymphocytes may respond to the strong unspecific stimulus, but not to tuberculosis-specific peptides. The performance of IFNγ assays using higher PHA concentrations in the positive control of the test may therefore be overestimated.
Current guidelines for the diagnosis of latent tuberculosis recommend M tuberculosis-specific IFNγ assays, which are targeted at diagnosing patients with latent tuberculosis who are likely to benefit from treatment.28 They emphasise, however, that results should be interpreted with caution in patients with an impaired immune system as the performance of these new assays has not been sufficiently evaluated. Our results indicate that the tuberculosis-specific IFNγ ELISA test has a better performance than the TST for the diagnosis of latent tuberculosis in this group of patients. Antigen-specific IFNγ assays such as the ELISA employed in our study may therefore be considered in addition to, or instead of, the TST for diagnostic screening of LTBI in immunosuppressed rheumatic patients. Prospective long-term studies are required to determine whether it is safe to withhold chemoprophylaxis for tuberculosis in patients undergoing TNFα inhibition if they had a positive TST but a negative IFNγ assay.
Acknowledgments
This study was funded by the Swiss Federal Commission for Rheumatic Diseases (EKR) and the Swiss National Science Foundation (grants Nos 3200-068070 and 3200-069338 to SDG); Dr Gadola is a Max Cloëtta research fellow, Dr Jüni is a PROSPER senior research fellow funded by the Swiss National Science Foundation (grants Nos 3233-066377 and 3200-066378).
REFERENCES
Footnotes
-
Competing interests: None.