Article Text

Abstract
OBJECTIVE Raised serum C reactive protein (CRP) and hyaluronate (HA) concentrations predict the progression of knee osteoarthritis (OA) in the long term but the consistency of these relations with time is unknown. The purpose of this work was therefore to determine if raised CRP and HA at entry and three years before entry (−3 years) predict radiological progression of knee OA in a group of patients between entry and five years.
METHODS Knee radiographs from 90 patients with knee OA at entry and five years follow up were assessed for progression of disease over five years. The concentrations of serum CRP and HA were measured at entry (n=90) and also in 40 serum samples available from −3 years. Odds ratios (OR) for predicting progression were calculated by logistic regression.
RESULTS Serum CRP at entry was not predictive of progression between entry and five years (OR 1.12, 95% CI 0.81, 1.55) but serum CRP at −3 years was predictive of progression (OR 1.90, 95% CI 1.01, 3.28). Serum HA concentration at entry predicted progression between entry and five years (OR 2.32, 95% CI 1.16, 4.66).
CONCLUSION These results are consistent with previous reports relating to HA, and suggest that raised serum CRP reflects events that precede a period of later radiographic progression in knee OA. However, because of the large overlap between groups, the serum CRP or HA concentration are not good predictors of individual patient progression and have a poor sensitivity and specificity.
- C reactive protein
- hyaluronate
- cartilage loss
- prediction
Statistics from Altmetric.com
Osteoarthritic diseases affect about 10% of adults over the age of 50 years,1 cause substantial health deficits2 and are the main cause of the demand for hip and knee prostheses.3 Osteoarthritis (OA) of the knee causes significant pain and disability.4 ,5 In many patients knee OA stabilises with time while in other patients it progresses.6 ,7 Previously, it was reported that patients in whom knee OA progressed over the following five years had significantly raised serum concentrations of hyaluronan (HA) at baseline compared with those whose disease did not progress.8 Similarly, patients whose knee OA progressed over four years had higher serum CRP concentrations at baseline compared with those who did not progress.9 However, the temporal relation between raised serum markers and progression of knee OA remains uncertain and can best be elucidated by long term follow up and monitoring of disease progression. We therefore examined the temporal relation between the concentration of CRP and HA (measured by a sensitive ELISA system) in stored serum samples from the entry and three years before entry (−3 year) visits of a cohort of OA patients in which the progression of knee OA between entry and five years had been assessed.10
Methods
PATIENTS
Patients were taken from a cohort of consecutive outpatients with peripheral joint symptoms attributable to radiographic evidence of OA who have been described previously.7 ,11 Of these, 114 had paired knee radiographs at entry and five years and for 90 of these a serum sample was available from the time of the entry radiograph. Serum samples taken three years before entering the study (−3 years) were also available from 40 of these patients. Clinical information available included age, sex, body mass index (BMI), knee pain (none, mild, moderate or severe) and joint examination for swelling (present or absent) and instability (present or absent).
RADIOGRAPHIC PROGRESSION
Standing anteroposterior radiographs were assessed separately by blinded and standardised methods.7 ,12 The Kellgren and Lawrence grade13 was recorded for each patient. In the medial compartment, the interbone distance was measured in millimetres using a ruler at the midpoint. Progression of knee OA was pre-defined as a reduction in interbone distance of 2 mm or more, or total knee joint replacement in either or both knees. This definition of progression has been used previously14 and is substantially greater than the variability inherent in these measurements.15
SERUM SAMPLES
Blood samples were separated and the serum stored at −70°C until subsequent assay. Only 40 samples were available from −3 years, but to our knowledge there was no systematic bias in determining which patients were used.
BIOCHEMICAL MARKERS
Serum CRP concentrations were measured by a sensitive ELISA capture assay using commercially available reagents. Microtitre plates were coated with rabbit antibody to human CRP (DAKO P 0227) in phosphate buffered saline (PBS) pH 7.4 and incubated over night at 4°C. The volume applied to the wells at each step was 100 μl. The plates were washed four times with PBS/0.05% (v/v) Tween 20. A calibration curve ranging from 1.25–25 μg/l using a human CRP reference serum (INCSTAR 84403) was set up and 100 μl/well of standards and appropriately diluted samples were added to the plate in duplicate. The International Reference serum for human CRP measurement (CRM 470-CAP/IFCC (DAKO X 0923)), was also used in each plate to guarantee the accuracy and reproducibility of the assay. The plates were incubated for 90 minutes at room temperature and washed as before. Then a second rabbit antibody to human CRP conjugated with horseradish peroxidase and diluted 1 in 2000 with PBS/Tween was added. The plates were incubated (90 minutes, room temperature), washed and 100 μl of peroxidase substrate added to each well before a further incubation (30 minutes, room temperature). The reaction was stopped by adding 100 μl of 1M sulphuric acid and the optical density at 492 nm measured in a plate reader. The capture assay produced a linear graph at 0–25 μg/l and the results of the unknown sample obtained from this graph by interpolation. The intra-assay and interassay coefficient of variations of the assay were 4% and 3% respectively.
Serum HA was measure by an ELISA inhibition assay modified from the method of Goldberg.16 In the inhibition step proteoglycan monomer, A1D1, extracted from human articular cartilage17was used instead of bovine nasal and tracheal cartilage D1 fraction used in the Goldberg assay. To detect the proteoglycan/HA complex the plate was incubated with the monoclonal antibody, 5D4, (purchased from ICN Biochemicals) which binds to an epitope on the KS GAG chains. After washing the plate an antimouse IgG alkaline phosphatase conjugate (Sigma) was added to the wells. The plate was incubated (one hour, 37°C) and developed with Sigma 104 alkaline phosphatase substrate. The plate was read in a microtitre plate reader at 405 nm and the results calculated using a computer programme (DeltaSoft). The intra-assay and interassay coefficient of variations of the assay were 4% and 6% respectively.
STATISTICAL TESTS
Serum CRP and HA results were either normalised by taking natural logarithms (Ln) before statistical analysis or analysed by the Mann-Whitney U test. The odds ratios (and their 95% confidence intervals) predicting progression were calculated by logistic regression including age, BMI, swelling, instability, Ln CRP and Ln HA as independent variables and progression or non-progression as the dependent variable.
Results
Table 1 shows the demographic and clinical characteristics of the patients. There were 55 women and 35 men, mean age 65 years. Kellgren and Lawrence scores of 1, 2, 3 and 4 were present in 22, 24, 27 and 17 patients respectively. Of the 90 patients, 38 progressed and 52 did not progress. The demographic, clinical and radiographic variables for the subset of 40 patients for whom serum samples were available at −3 years were similar to group as a whole at entry (see table1).
Demographic and clinical characteristics of the patients
Table 2 gives the mean CRP and HA values for the patients and individual values for all 90 patients at entry are illustrated in figure 1. At entry the CRP concentrations of the 40 patients (for whom serum samples were also available at −3 years) was higher than the full set of 90 patients but this was not statistically significant (p=0.162). Serum HA values of the two groups were similar at entry (see table 2).
Serum CRP and HA concentrations at entry

Serum CRP and serum HA concentrations in all patients (n=90) at entry.
Table 3 shows the odds ratios for predicting disease progression. Raised serum CRP measured at entry does not identify those patients who will progress. By contrast, serum CRP at −3 years is predictive of progression in OA from entry to five years (p=0.042). Serum HA is increased at both time points in those who show progression. At −3 years this is of borderline statistical significant (p=0.067) but at entry it is significant (p=0.016). To illustrate these findings, the individual serum concentrations of CRP and HA for the 40 patients in whom measurements at entry and −3 years are available are shown in relation to disease outcome in figures 2 and 3. Because of the large overlap between groups, the serum CRP or HA concentration is not a good predictor of individual patient progression. The sensitivity and specificity for CRP at −3 years (cut off 9.65 mg/l) was 38% and 85%, at enry CRP had no predictive power. Those for HA at −3 years (cut off 117.3 ng/ml) were 46% and 87% and at entry (cut off 150.0 ng/ml) were 38% and 89%.
Odds ratios for predicting progression between entry and five years

Serum CRP concentrations at −3 years and at entry in relation to disease outcome for the 40 patients in whom both samples were available. The horizontal bars indicate the mean in each group, p values are from Mann-Whitney U test.
{kind=link}
{kind=link}
{kind=link}
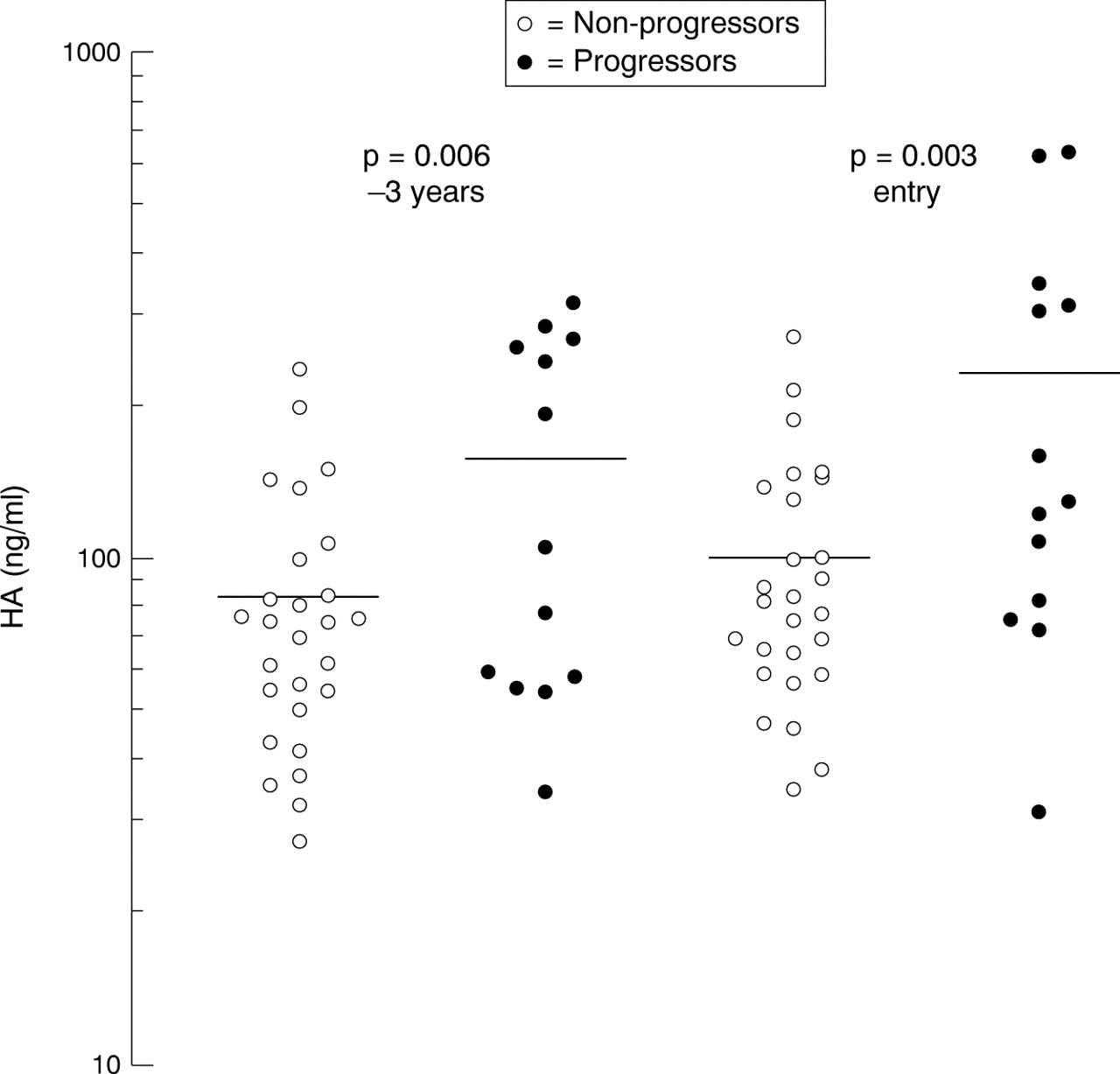
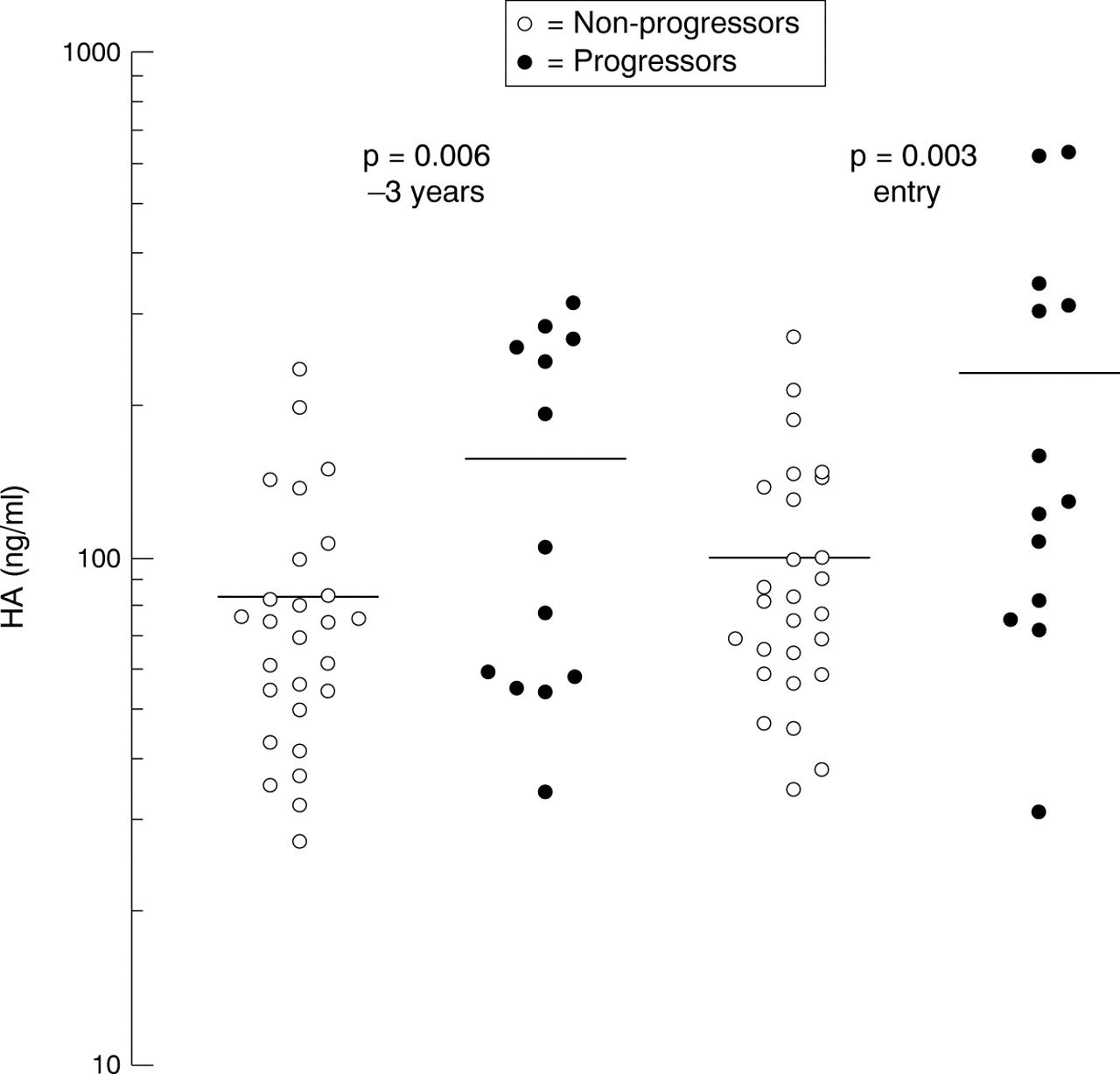
Serum HA concentrations at −3 years and at entry in relation to disease outcome for the 40 patients in whom both samples were available. The horizontal bars indicate the mean in each group, p values are from Mann-Whitney U test.
Discussion
There have been a number of reports demonstrating associations between biochemical markers measured in serum and disease severity and outcome in OA.8 ,9 ,18 Although CRP has traditionally been seen as “normal” in OA, sensitive assays show that it is raised in many patients but is below the level usually detected in hospital chemical pathology departments.9 ,18 ,19Increased serum CRP9 and HA8 have been shown to predict progression of disease in two previous cohort study reports. The results presented here confirm that raised serum HA is predictive of an immediate period of progression of knee OA. They show that serum HA is also predictive of progression if measured three years before. In contrast, serum CRP was not predictive of progression when measured immediately before a five year progressive period, but was predictive of that progression when measured three years in advance. Because of the large overlap between groups, the serum CRP or HA concentration are not good predictors of individual patient progression and have a poor sensitivity and specificity. However, the data provide an insight into potential pathological mechanisms.
This is a convenience sample of patients presenting with knee OA at one time and being assessed at another, raising the possibility that selection bias might be influencing the CRP values and their changes. However, the principal finding of our study is that measurements of CRP at one time point are related to radiographic progression over a distant (three years ahead) and prolonged (the subsequent five years) period. Even if the cause of the raised CRP was also the cause of the presentation to the rheumatologist (for example, it may be related to an inflammatory episode), that does not detract from the conclusion that serum CRP reflects events that precede a subsequent period of cartilage loss.
In this study, progression on radiographs represented principally joint space narrowing and hence loss of articular cartilage in the medial compartment. The results are consistent with previous studies of these markers in OA8 ,9 and were statistically significant when age and BMI were taken into account. This has been the case even though patellofemoral disease has not been assessed in these cohorts of patients. The presence and progression of patellofemoral disease will serve to cloud the link to serum marker measurements. Furthermore, CRP and HA measurements were available in a relatively small number of patients and they may have OA at other sites as well as the knee joint. Nevertheless, our findings are statistically significant and suggest that a raised serum CRP reflects events that precede a subsequent period of cartilage loss. This implies that some events associated with cartilage loss begin before others.
Raised CRP may be related to other patholological findings. For example, increased serum CRP (measured using a similar sensitive method) has been found in patients with cardiovascular diseases.20 However, this group consisted of patients aged between 50 and 59 years, an age group where OA is common. It is therefore conceivable that the raised CRP concentrations in this group is attributable to pre-clinical OA and that an increase of serum CRP (when other intercurrent diseases associated with raised CRP is absent) may identify subjects who will develop OA. Further longitudinal studies of biochemical markers in this type of patients would explore the usefulness of serum CRP and HA as prognostic markers.
Our earlier studies found that abnormal bone scintigraphy correlate with subsequent cartilage loss.14 Bone scans that showed active uptake in the knee identified patients with about a 50% chance of radiological progression (as defined in this study) over the following five years, while a negative scan virtually ruled out such progression. This may suggest that bony reaction is an integral part of the pathological processes related to cartilage loss. Moreover, the results indicate that activation of bone metabolism occurs, like raised serum CRP concentrations, out of phase with the loss of cartilage. These data raise the possibility that a variety of joint tissues are involved in the pathogenesis of tibiofemoral OA, and that they become active in the disease process in a phasic pattern.21