Article Text

Abstract
OBJECTIVE To determine whether there is a relation between disease duration and functional outcome in patients with rheumatoid arthritis (RA) treated with intramuscular sodium aurothiomolate (gold) for five years.
METHODS 440 patients with RA were enrolled in a prospective trial of gold treatment. Initial demographic details were recorded. Disease activity was assessed at yearly intervals using a combination of clinical (pain score, Ritchie articular index, duration of morning stiffness) and laboratory (erythrocyte sedimentation rate, C reactive protein) parameters. Change in functional status was assessed using the health status questionnaire (HAQ). Patients were stratified according to disease duration at outset (group 1= 0–2 years n=106, group 2 = >2–5 years n=93, and group 3= >5 years n=235).
RESULTS There were no significant differences between the groups at outset. A total of 160 patients completed five years of treatment (group 1 n=44 (42%), group 2 n=37 (40%), and group 3 n=79 (34%)). Patients in group 1 had a significantly lower HAQ from year 1 to year 5 with a mean improvement of 30% at the end of the study (p<0.001). Neither group 2 nor group 3 had a significant change in their HAQ at study end. There were significant improvements in all other variables (p<0.05) in each group apart from pain in group 2.
CONCLUSION Patients with early RA have a larger reversible component to their HAQ. Only patients with disease duration of up to two years have a longlasting improvement in their functional ability after starting intramuscular gold treatment.
- gold
- rheumatoid arthritis
- function
- HAQ
Statistics from Altmetric.com
Traditionally the approach to the treatment of rheumatoid arthritis (RA) has entailed a gradual stepwise increase in treatment—the “pyramidal” approach.1 Non-steroidal anti-inflammatory agents have been used initially until it becomes evident that the patient has a persistent inflammatory response associated with joint damage and at this stage a disease modifying anti-rheumatic drug (DMARD) may be introduced. The rationale behind this approach was the belief that many cases of RA may pursue a benign course2 and that non-steroidal agents are less toxic than DMARDs. Both these initial suppositions now seem to be incorrect3 ,4 and there is a tendency towards using DMARDs earlier in the disease process. The expectation is that by reducing the inflammatory response early, less joint damage may occur and disability should be minimised.5
Results from a short-term study of this approach seem promising,6 however there are few long term data. This study reports the outcome of a large cohort of RA patients treated with sodium aurothiomolate (intramuscular gold) over a five year period. Functional ability has been chosen as the primary outcome measure as the major aim of DMARD treatment is to reduce functional loss. In addition functional ability is strongly related to work loss7 and mortality.8 The results in our study have been stratified according to disease duration at outset. Intramuscular gold was chosen as it is widely accepted as an effective DMARD,9 compliance is assured, and there is some evidence it may retard radiological progression,10 particularly when used in early disease.11
Methods
PATIENTS
The study was conducted at two hospitals in Glasgow, Scotland serving as both secondary and tertiary referral centres. Recruitment to the study was between 1986 and 1990.
Patients with an active inflammatory polyarthropathy not controlled with NSAIDs or an alternative DMARD and who fulfilled the American Rheumatism Association12 criteria for RA were enrolled in a prospective study of intramuscular sodium aurothiomolate (gold). None of the subjects was receiving regular oral corticosteroids. Baseline demographic details recorded included: sex, age, disease duration, and seropositivity for rheumatoid factor. The study was divided into three cohorts depending on the duration of disease at inception; group 1 0–2 years, group 2 >2–5 years, and group 3 >5 years. The number of previous DMARD agents was recorded and ranged from 0–3. Although the median for all three groups was zero, those with the shortest disease duration not surprisingly had been exposed to fewer agents (p<0.001, Kruskal-Wallis).
GOLD TREATMENT
Gold (sodium aurothiomolate) was initially given as a test dose of 10 mg intramuscularly (im) and if there were no adverse effects a dose of 50 mg (im) was given weekly until a response was obtained. Thereafter the frequency of injections was reduced and maintenance treatment was usually at four weekly intervals. Blood and urine monitoring was performed by family practitioners.
DISEASE ACTIVITY
Disease activity was monitored by a combination of clinical and laboratory parameters. Clinical parameters included: duration of morning stiffness, Ritchie articular index, and a visual analogue score (VAS) for pain (scale 0–3). Laboratory parameters included erythrocyte sedimentation rate (ESR) and C reactive protein (CRP).
FUNCTIONAL ABILITY
Functional outcome was assessed using the Health Assessment Questionnaire (HAQ).13 This assesses the ability to perform activities of daily living in eight separate categories. Ability is rated from 0 (no difficulty) to 3 (unable to do), the mean value for the eight categories is quoted. All parameters were recorded at baseline and annually thereafter by a trained metrologist (EAT). The study was not designed on an intention to treat basis, however limited data are available for those who failed to complete the five years (by a review of their case records).
STATISTICAL ANALYSIS
Within group analysis over the five years of treatment was performed using Wilcoxon signed rank test. Between group comparisons were analysed using a Mann-Whitney or Kruskal-Wallis test where appropriate. All statistical tests were performed using a Minitab programme (Minitab Inc, 1994).
Results
After five years treatment 160 of the 440 initial patients remained on treatment. Fifty nine patients had died of conditions unrelated to gold treatment.
DISEASE DURATION
Patients were stratified into three groups according to their disease duration at initiation into the study (group 1= 0–2 years (n=106), group 2=>2–5 years (n=93), group 3= >5 years (n=235) data were not available in six cases). The numbers completing five years of treatment were: group 1 n=44 (42%), group 2 n=37 (40%), and group 3 n=79 (34%). Table 1 shows the demographic details and cumulative gold dose for these groups. There were no significant differences between the groups at baseline (Kruskal-Wallis). Table 1 also shows baseline details for those that failed to complete the study (non-completers). The only significant difference was in group 3 where the non-completers tended to be older. In group one the median ESR and CRP appear higher in the non-completers, however the ranges are similar and the differences were not statistically significant.
Baseline demographic, disease activity parameters, and cumulative gold dose according to disease duration
FUNCTIONAL OUTCOME
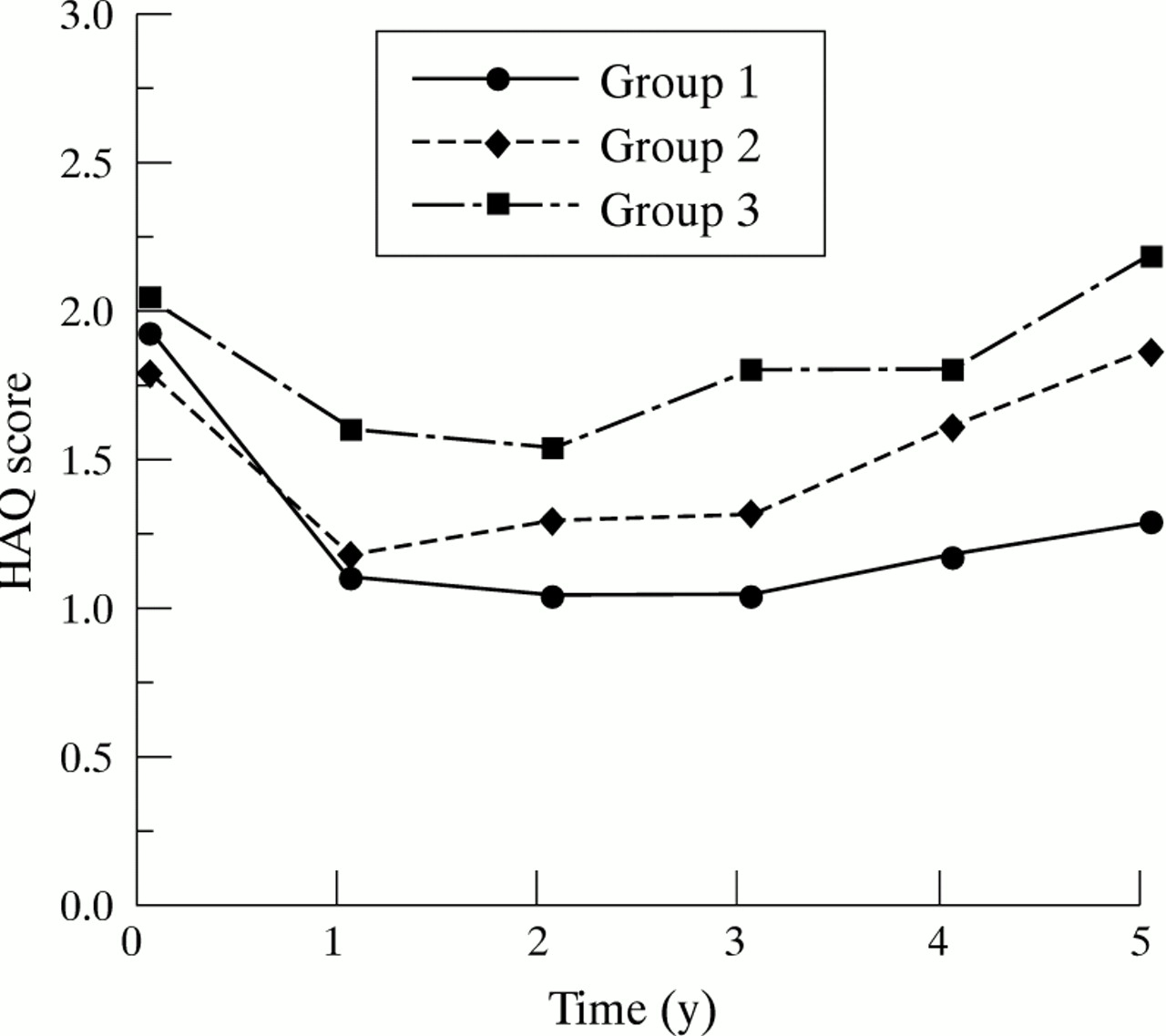
Change in HAQ over the five years is shown in table 2 and figure1. There was a significantly greater improvement in year 1 in those with early disease (group 1) compared with those with later disease (groups 2 and 3) and this difference was maintained throughout the five years. Despite a gradual deterioration in HAQ after the third year, function (HAQ) at the final (5 year) evaluation remained significantly better than the HAQ at outset (p<0.001, Wilcoxon). The patients with longer disease had a smaller initial improvement in HAQ before a gradual decline in function, which meant that by five years their HAQ was not significantly different from before gold treatment.
Change in HAQ score over five years according to initial disease duration

Median change in HAQ over five years stratified according to initial disease duration. Group 1= 0–2 years, group 2= >2–5 years, and group 3= >5 years.
DISEASE ACTIVITY
Figure 2 shows change in markers of disease activity. All parameters improved from 0–5 years (significant at p<0.01 Wilcoxon) apart from pain in group 2 (p=0.313) and group 3 (p=0.039). Change in morning stiffness is not shown but was highly significant for all groups (p<0.001). There were no significant differences for change in disease activity parameters between the groups (Kruskal-Wallis).

Median change in laboratory and clinical markers of disease activity over five years stratified according to initial disease duration. Group 1= 0–2 years, group 2= >2–5 years, and group 3= >5 years.
TREATMENT FAILURES
Figure 3 shows the reasons for withdrawal. In total there were 280 treatment failures, data regarding 243 of these patients were available at five years. One hundred and twenty four were receiving an alternative DMARD, four had re-started im gold, 56 were taking no DMARDs, and 59 had died. Table 3 shows the results of their inflammatory indices at five years compared with the completers. Those still receiving gold treatment had a significantly lower ESR and a non-significant tendency to a lower CRP than the treatment failure groups. Unfortunately no data on functional capacity are available for those withdrawing from the study.

Reasons for withdrawal of gold treatment (n=280).
ESR and CRP values at five years depending on treatment at the end of the study period
There were 59 deaths over the five years, 37 occurred during treatment and 22 after cessation of gold treatment. None of the deaths was attributable to gold treatment. As was to be expected those that died were significantly older at the outset of the study (66 compared with 56 years, p<0.001) and more functionally disabled (2.250 compared with 2.000 HAQ, p<0.001) than the rest of the study subjects at baseline.
Discussion
There has been a fundamental change in emphasis to the treatment of RA over the past 10–15 years. Previously DMARDs were considered unacceptably toxic and were reserved for patients who developed a progressive destructive arthropathy. Sherrer et alreporting from Saskatchewan, Canada on the development of disability in RA in 1986 noted the mean time to initial DMARD use was 12.8 years.14 This approach reflected not only the perceived toxicity of the DMARDs but also the belief that RA was in general a benign disease and that in only a few patients would the potential benefits of these agents outweigh the risk.
Our understanding of the natural history of RA has changed. We now appreciate that for a significant proportion of patients RA is a chronic and relentlessly disabling disease. A community based study from Finland found that a HAQ >1 was found in 36–50% and a HAQ >2 in 11–21% of those with disease >10 years.15 A hospital based study as would be expected found a greater degree of disability existing in their patients; after 10 years of disease approximately 50% of patients had a HAQ score of >2.5 representing severe disability.16 Thus the more aggressive approach to drug treatment that has emerged can certainly be justified. The current recommendations of the American College of Rheumatology are that DMARDs should be considered for any patient with an established diagnosis of RA who have a raised acute phase response or whose symptoms are not adequately controlled with non-steroidal agents.17 The hope is that prompt use of disease modifying agents will slow, or even halt, the rapid functional decline that occurs early in the disease process.
Our study results lend support to the current more aggressive approach to treating RA. We followed up a group of patients who had what may be considered a good response to a single DMARD over a five year period. Analysis of the results, taking into consideration duration of disease at the outset of the study, showed that patients with early disease had a very much more favourable functional outcome at five years despite similar initial disability. The most dramatic difference was seen in the first two years with a much more substantial sustained improvement in HAQ in the early disease group. The fact that the difference is maintained means that at the end of the study this cohort is approximately 30% less disabled than they were initially despite a further five years of disease. This contrasts with the two groups with initial disease duration greater than two years where there was no difference between initial and final HAQ results. The greater reversibility in HAQ may be because of a larger proportion of early disability being caused by active synovitis with little underlying joint damage. In later disease the degree of irreversible joint damage may play a greater part in functional disability and thus leave less scope for improvement with disease modifying agents. Studies showing the appearance of radiographic changes in the first years of RA18 ,19 support our findings that disability becomes much less reversible after only two years of disease. A recent study of radiological progression of joint disease in RA showed that at three years 70% of patients will have erosive disease.20However, as radiological damage continues throughout the course of active RA21 treating even late disease is worthwhile.
One other possible explanation for our results is that not all the patients enrolled in the early group truly had RA. Early synovitis clinics report significant remission rates depending on the population studied. The rates vary from 55% for patients with disease less than six months22 to 15% for those with disease less than two years.23 We examined the nine patients in the early group who were least disabled (HAQ< 0.5) at five years. At presentation seven of nine were rheumatoid factor positive and seven of nine had an ESR >30 mm 1st h, the combination of a positive RF and ESR >30 mm 1st h makes the diagnosis of RA 11-times more likely than a self limiting synovitis.22 Also the early group as a whole had a high prevalence of seropositivity for rheumatoid factor (77%), which was similar to the later disease groups (81%). In the light of these findings it is very unlikely that the study group was significantly contaminated by patients with a self limiting “reactive” inflammatory arthropathy.
Our results suggest that the therapeutic window for improving functional outcome lies within the first two years of disease. This is in keeping with the data of Wolfe et al showing that HAQ improved only in patients seen within two years of disease onset,16 although follow up for this group was relatively short (mean 1.8 years). There is however some evidence to suggest the therapeutic window may exist even earlier in the disease course. In a double blind placebo controlled study of early versus an eight month delay in initiating DMARD treatment there was only a significant improvement in HAQ in the early group at five years.24 The authors also showed that radiological changes were more severe in the delayed group at five years whose Larsen score was almost double that of the early disease group. This confirmed a previously performed study looking at early versus delayed DMARD treatment (im gold).11 They reported that in the early group (2–10 months of disease) the Larsen score deteriorated over five to six years in 38% of joints studied compared with 67% in the late group (21–36 months).
A potential weakness of our study is the possibility that the patients with longer disease may be non-responders to previous DMARDs and therefore a self selected group with potentially a worse outcome. There are three points against this supposition. Firstly, the percentage of patients who had been exposed to a previous DMARD was the same for both completers and non-completers at 27%. Secondly, the baseline characteristics of the groups were well matched. Finally, the percentage of patients in the three groups still receiving treatment at five years are comparable and a review of the clinical and laboratory parameters of disease activity shows the response to gold to be very similar between all three groups. These findings are in keeping with a previous study that showed improvement in clinical and laboratory indices of disease activity was independent of disease duration before commencement of im gold.25 In our study there is a tendency for pain to respond less well in the later disease groups, this may be because of a greater degree of mechanical pain secondary to irreversible joint damage in these groups: here the goal is surgery/rehabilitation.
This study describes a large cohort of RA patients treated with im gold but it is probable that similar results could be achieved with other DMARDs shown to be of equal potency such as sulphasalazine, penicillamine, and methotrexate.26 Our study does however confirm the long term efficacy of gold particularly in those patients who manage to complete the first year of treatment. The survival curve in figure 4 shows this very clearly with relatively few drop outs in years 3–5. This taken in conjunction with figure 2 is in contrast with the belief held by some that gold becomes much less effective over time.27

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Survival curves for remaining on gold treatment. Group 1= 0–2 years, group 2= >2–5 years, and group 3= >5 years.
Another point of note is that ours was a study based in hospitals, which as well as serving their own area also acted as supra-regional tertiary referral centres and therefore the patients had more severe disease than may be encountered in a community-based practice: this is reflected in the high initial HAQ scores for all three groups. However, a recent community study reminds us that polyarthropathy presenting in primary care is not a benign disease with 29% of patients having a HAQ score >1 after one year of disease.28 Thus the results of this study are likely to be widely relevant.
It is important that this information about functional outcome is made available to patients when introduction of DMARD treatment is discussed. A significant minority of patients are deterred from embarking on such treatment because of their perception of the dangers—often exaggerated and ill founded fears. In addition early referral to and availability of advice from a speciality rheumatology service is clearly of importance.
This study shows that gold, a potent DMARD has different effects on the course of RA depending on the duration of disease. In early RA treatment seems to improve functional capacity in addition to controlling symptoms and signs of disease activity. In later disease (after two years) there is a satisfactory symptomatic, clinical, and laboratory response but no sustained improvement in disability. This study adds to the growing body of evidence favouring early institution of disease modifying treatment in RA.
Acknowledgments
Our thanks to Drs J Hunter, D Porter, M Field and Professor R Sturrock for permission to study their patients.