Article Text

Abstract
Background JAK-inhibitors (JAKi), recently approved in rheumatoid arthritis (RA), have changed the landscape of treatment choices. We aimed to compare the effectiveness of four current second-line therapies of RA with different modes of action, since JAKi approval, in an international collaboration of 19 registers.
Methods In this observational cohort study, patients initiating tumour necrosis factor inhibitors (TNFi), interleukin-6 inhibitors (IL-6i), abatacept (ABA) or JAKi were included. We compared the effectiveness of these treatments in terms of drug discontinuation and Clinical Disease Activity Index (CDAI) response rates at 1 year. Analyses were adjusted for patient, disease and treatment characteristics, including lines of therapy and accounted for competing risk.
Results We included 31 846 treatment courses: 17 522 TNFi, 2775 ABA, 3863 IL-6i and 7686 JAKi. Adjusted analyses of overall discontinuation were similar across all treatments. The main single reason of stopping treatment was ineffectiveness. Compared with TNFi, JAKi were less often discontinued for ineffectiveness (adjusted HR (aHR) 0.75, 95% CI 0.67 to 0.83), as was IL-6i (aHR 0.76, 95% CI 0.67 to 0.85) and more often for adverse events (aHR 1.16, 95% CI 1.03 to 1.33). Adjusted CDAI response rates at 1 year were similar between TNFi, JAKi and IL-6i and slightly lower for ABA.
Conclusion The adjusted overall drug discontinuation and 1 year response rates of JAKi and IL-6i were similar to those observed with TNFi. Compared with TNFi, JAKi were more often discontinued for adverse events and less for ineffectiveness, as were IL-6i.
- Epidemiology
- Biological Therapy
- Tumor Necrosis Factor Inhibitors
- Arthritis, Rheumatoid
- Therapeutics
Data availability statement
Data are available on reasonable request. All the data belong to the registers. Anonymised data can be shared as long as agreements are made with all participating registers.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is already known on this topic
For patients with rheumatoid arthritis with an inadequate response or contraindications for conventional synthetic disease-modifying antirheumatic drugs (DMARDs), several second-line therapy options exist from which rheumatologists and patients can choose.
Only a limited number of small studies have evaluated the effectiveness of targeted-synthetic DMARDs and biological DMARDs in the real world.
What this study adds
This large comparative effectiveness analysis, involving 19 registers and over 30 000 treatment courses, is the first to evaluate real life effectiveness and safety outcomes among four common available treatment alternatives and found similar discontinuation rates and Clinical Disease Activity Index response, although discontinuation reasons tended to differ between treatments, with more discontinuation for safety with JAK-inhibitors, but less for effectiveness.
How this study might affect research, practice or policy
Considering similar effectiveness among these treatments, this study calls for the evaluation of other outcomes that could influence treatment choice, such as patient-reported outcomes, comorbidities, tolerability, safety or cost-effectiveness.
Introduction
Since the development of tumour necrosis factor-inhibitors (TNFi) in the nineties, treatment options for rheumatoid arthritis (RA) have greatly increased with the emergence of other classes of biological disease-modifying antirheumatic drugs (bDMARDs), such as interleukin-6 inhibitors (IL-6i) and abatacept (ABA), and more recently the targeted-synthetic DMARDs (tsDMARDs), with Janus kinase inhibitors (JAKi).1–9 While all bDMARDs and tsDMARDs have demonstrated efficacy in randomised controlled trials,1–9 these results are not always relevant to ‘real-world patients’, because of very restrictive inclusion criteria, numerous exclusion criteria and limited follow-up.10 In addition, bearing in mind the number of current options available, head-to-head trials including several of the alternative treatment options would be impractical to realise. However, considering the number of available treatment options for second-line therapy in RA, a representative estimation of their relative effectiveness in the real world would be useful to help patients and rheumatologists to choose an appropriate treatment. Registers provide a unique opportunity to compare available treatment options and understand the effectiveness of these therapies in clinical situations, which is becoming even more important as we move towards personalised clinical care. The objective of this study was thus to evaluate and compare the real-world effectiveness of four different second-line therapies namely TNFi, ABA, IL-6i and JAKi.
Methods
Patient sample
The JAK-pot collaboration is an investigator-initiated observational study, which aims to evaluate clinical aspects of bDMARDs and tsDMARDs in RA. Patients were included since JAKi were commercially available in each country (earliest being 2013 for Switzerland and Russia) until March 2021. To avoid confounding by time-trends, we excluded patients who initiated treatment of interests (bDMARDs or JAKi) before JAKi were commercially available in each country. Patients with a clinical diagnosis of RA and starting treatment with a JAKi (baricitinib, tofacitinib or upadacitinib at that time), a TNFi, ABA or an IL-6i during the study period, were included from the following registers: ATTRA from the Czech Republic, ARBITER from Russia, BIOBADASER from Spain, BIOREG from Austria, biorx.si from Slovenia, BSRBR-RA from the UK, DANBIO from Denmark, GISEA from Italy, I-RECORD from Israel, METEOR from the Netherlands, NOR-DMARD from Norway, RABBIT from Germany, REUMA.PT from Portugal, RHUMADATA from Canada, ROB-FIN from Finland, RRBR from Romania, SCQM from Switzerland, TARDIS from Belgium, TURKBIO from Turkey. ARBITER, biorx.si, BSRBR-RA and RABBIT did not contribute ABA treatment courses, and RABBIT did not contribute IL-6i treatment courses. All registers contributed individual treatment course-level data (eg, non-aggregated) to this collaborative analysis, except DANBIO and TARDIS that provided only aggregated data and results of analyses. Filgotinib was not included because it was not marketed during most of the study period in participating registers. Rituximab was also not included as discontinuation is often difficult to assess.
Time point definitions and treatment groups
Baseline was defined as the initiation date of each of the treatment courses under investigation. Each treatment course was operationally defined as the period between drug initiation to treatment discontinuation, the switch to another treatment, the end of participation in the register, or the end of the study period (March 2021), whichever came first. Durations between visits depend on the register design and national recommendations on frequency of clinical contact, but most registers usually include at least an annual visit.
Exposure of interest
The exposure of interest was the type of treatment (TNFi, ABA, IL-6i or JAKi).
Study outcomes
The primary outcome of effectiveness was treatment discontinuation, which was evaluated in all registers. As secondary outcomes of effectiveness, we evaluated (1) reasons for discontinuation by treatment and (2) treatment response using the Clinical Disease Activity Index (CDAI) defined as reaching low disease activity (LDA, CDAI ≤10) and remission (CDAI ≤2.8) at 12 months.11 12 We used CDAI as disease activity measure as it does not include acute phase reactants and is less skewed by agents having a strong effect on acute phase reactants, such as IL-6i and probably JAKi.
Covariates of interests
For multivariable adjustments, we chose baseline covariates considered a priori as potential confounding factors according to clinical knowledge and current literature.13 We included gender, age, disease duration, seropositivity, number of previously used bDMARDs/tsDMARDs (0, 1, 2, ≥3), concomitant conventional synthetic DMARDs (csDMARDs) treatment (none; methotrexate; other csDMARDs without methotrexate; methotrexate and at least one other csDMARDs), concomitant glucocorticoids (presence/absence), tobacco smoking, functional status (Health Assessment Questionnaire Disability Index -HAQ-DI), CDAI (or Disease Activity Score on 28 joints - DAS28 - if CDAI was not available), C reactive protein (CRP) and year of treatment initiation. For seropositivity, patients were classified as being seropositive if rheumatoid factor (RF) and/or anticyclic citrullinated peptide antibodies (ACPA) were positive, negative if both were negative, and missing if one was missing and the other was negative, to limit misclassification. In BSRBR-RA, only RF was available and seropositivity was defined as positive if RF was positive, negative if RF was negative, and missing if RF was missing. In the TARDIS register, concomitant csDMARDs treatment, HAQ, CDAI and seropositivity were not available, and DAS28 was used for adjustment for disease activity. Other sporadically missing data by registers are shown in online supplemental table 1.
Supplemental material
Statistical methods
We performed analyses and reported results according to the Strengthening the Reporting of Observational Studies in Epidemiology guidelines and the European Alliance of Associations for Rheumatology points to consider on comparative effectiveness research.14 15
We analysed baseline characteristics using standard descriptive statistics and indicated number of patients with valid values. Since two of the registers could only provide aggregated results due to local regulations with respect to cross border data sharing, all adjusted analyses were performed within each individual register and combined using random-effect meta-analysis methods, which also allowed to account for possible heterogeneity between registers. Heterogeneity was evaluated using I2. Several treatment courses from a single patient could be included if the patient had been treated by more than one second line treatment during the follow-up period. Thus, we added a cluster term for the patient identity, thereby allowing the estimation of robust SEs, in a manner similar to generalised estimating equation models. The investigators of the two registers that did not provide individual treatment course-level data, received a detailed description of the analyses, as well as the code used for the analyses (in R programming language), and replicated these analyses as closely as possible.
Main outcome
For the primary outcome (drug retention), we used Kaplan-Meier and Cox models. The Cox models were adjusted for all the baseline covariates as described above. TNFi was used as the comparison group, comprising the most treatment courses. Missing covariates were imputed using multiple imputations with chained equations (50 samples, predictive mean matching algorithm, see supplementary methods). A cluster term was added for the patient identity, as each patient could provide information for each treatment arm. As a sensitivity analysis, we excluded TARDIS, as some covariates were not available for adjustment in this register.
Secondary outcomes
For the secondary outcomes, only registers with individual treatment course-level data (non-aggregated) were included (17 registers, online supplemental figure 1).
For the analysis of discontinuation reasons, we used a Fine-Gray model for adverse events, considering lack of effectiveness and other reasons of discontinuation as competing risks. To avoid overadjustment, and as this was a secondary analysis, we pooled the registers and adjusted for fewer a priori selected baseline variables than for the main outcome namely: gender, age, disease duration, seropositivity, previous treatment with a b/tsDMARD as a binary variable (presence/absence), CRP, CDAI and presence of a concomitant treatment with csDMARDs as a binary variable (presence/absence) with a strata term for the country and the year of treatment initiation. Missing covariates were imputed using multiple imputations.
For the other secondary outcome (CDAI treatment response at 1 year), we additionally excluded BSRBR-RA, I-RECORD, RRBR and TURKBIO registers, as information on CDAI was not available for follow-up visits (online supplemental figure 1). When no CDAI assessments were present at 1 year at the individual level, the means of their values within a±1.5 months window were used. Values that were still missing for patients on drug after 12 months were imputed using the nearest available neighbour, as advised by a recent simulation study.16 We estimated the proportions of patients reaching remission or LDA by treatment group using a method correcting for attrition (patients lost to follow-up or stopping treatment), and adjusting for confounders (confounder-adjusted response rate with attrition correction).17 Briefly, this method discards values of CDAI at 12 months for treatment courses discontinued before 12 months, due to potential influence of new, subsequent treatments. It then uses multiple imputation with chained equations to estimate the difference of CDAI remission or LDA between treatments, adjusting for covariates. These covariates include those used for the discontinuation model but also the reason for treatment discontinuation (ineffectiveness, adverse events, other reasons). When using this method, the adjusted response rates correspond to the response rates that the whole population would have had if all had been treated with the treatment of interest. We also calculated adjusted difference in response rates using TNFi as comparator.
Results
We included a total of 31 846 treatment courses: 17,522 TNFi, 2775 ABA, 3863 IL6-i and 7,686 JAKi. Two registers provided only aggregated data, while the rest of the 17 registers provided individual treatment course-level data, for a total of 20 837 treatment courses (table 1). In these 17 registers, patients were on average 56.8 years old, with a mean disease duration of 10.2 years, mostly seropositive (80%), female (78%) and with moderate disease activity at treatment initiation. Forty-one per cent of the JAKi treatment-courses were baricitinib and 59% tofacitinib. There were no patients included during the study period with upadacitinib. Overall baseline characteristics were similar between registers (online supplemental table 1). Patients starting TNFi were younger, had a shorter disease duration, less previous b/tsDMARD experience, and were less often on monotherapy. JAKi and IL-6i were more often given as monotherapy, and JAKi were more often prescribed after several treatment failures. Treatment groups were comparable for gender, seropositivity and disease activity.
Characteristics of the patients at the start of their 20 837 treatment courses (17 registers, individual treatment course-level data)
Treatment retention
Crude median drug retention for registers with individual treatment course-level data was 1.68 years (IQR 1.62–1.74) for TNFi, 1.58 years (IQR 1.48–1.73) for ABA, 1.88 years (IQR 1.76 to 2.02) for IL-6i and 1.19 (IQR 1.10–1.26) years for JAKi. Crude HR of discontinuation for ABA compared with TNFi was 1.16 (95% CI 0.97 to 1.39), 1.05 (95% CI 0.91 to 1.21) for IL6-i and 1.48 (95% CI 1.20 to 1.83) for JAKi. When adjusting for confounding factors, we no longer found any significant difference in the adjusted HRs (aHR) for discontinuation for ABA (aHR 0.96, 95% CI 0.86 to 1.07), IL-6i (0.91, 95% CI 0.82 to 1.01) and JAKi (1.00, 95% CI 0.83 to 1.22), compared with TNFi (figure 1). In the sensitivity analysis excluding TARDIS, aHR for discontinuation were not significantly different for ABA (0.94, 95% CI 0.84 to 1.06) and JAKi 0.96 (95% CI 0.82 to 1.12) compared with TNFi but tended to be slightly lower for IL-6i (0.89, 95% CI 0.81 to 0.98). The adjusted hazard of JAKi discontinuation compared with TNFi was heterogeneously distributed across the countries (figure 2, I2=92.7%). We obtained less discrepant results for IL-6i vs TNFi (I2=64.1%) and ABA vs TNFi (I2=58.4%).

Multivariable Cox model of drug discontinuation in patients from 16 registers with individual treatment course-level data. Analysis was adjusted for age, gender, disease duration, seropositivity, number of previous treatments, concomitant treatment with csDMARDs, concomitant treatment with glucocorticoids, CRP, HAQ, CDAI, comorbidities, smoking and BMI, and stratified by country and year of treatment initiation. ABA, abatacept; BMI, body mass index; CDAI, Clinical Disease Activity Index; CRP, C reactive protein; csDMARDs, conventional synthetic disease-modifying anti-rheumatic drugs; HAQ, Health Assessment Questionnaire; JAKi, Janus kinase inhibitors.

HR of discontinuation compared with TNF-inhibitors by country and treatment. Adjusted for age, gender, disease duration, seropositivity, number of previous treatments, concomitant treatment with csDMARDs, concomitant treatment with glucocorticoids, CRP, HAQ, CDAI, comorbidities, smoking and BMI, and stratified by country and year of treatment initiation. All countries HR combined using a meta-analysis with random effect. AU, Austria; BE, Belgium; CA, Canada; CH, Switzerland; CZ, Czech Republic; DE: Germany, DK, Denmark; ES, Spain; FI, Finland; IL, Israel, IT, Italy; NL, Netherlands, NO, Norway, PT, Portugal, RO, Romania; RU, Russia; SI, Slovenia; TR, Turkey. DE, SI, RU and UK do not have or provide data on ABA. DE did not provide data on IL-6i. Due to lack of information on these variables, BE did not adjust for concomitant treatment with csDMARDs, concomitant treatment with glucocorticoids, HAQ, CDAI, smoking, BMI, comorbidities and seropositivity and adjusted for DAS28. HR for RU is out of bound: 5.0 (95% CI 1.0 to 22.9) for IL6-i, 3.7 (1.2 to 11.4) for JAKi. HR for nl is out of bound: 4.0 (95% CI 1.6 to 10.0) for JAKi. ABA, abatacept; BMI, body mass index; CDAI, Clinical Disease Activity Index; CRP, C reactive protein; csDMARDs, conventional synthetic disease-modifying antirheumatic drugs; HAQ, Health Assessment Questionnaire; IL6i, interleukin 6 inhibitors; JAKi, Janus kinase inhibitors.
Discontinuation reasons
In the 17 registers with individual treatment course-level data, the main unique reason of stopping treatment was rather ineffectiveness than adverse events, and the order was similar for all treatments. Sixty-two per cent of treatment-courses specified the reason of discontinuation. When analysing the reason for discontinuation by treatment, no differences existed between ABA and TNFi for any of the discontinuation reason, while IL-6i (aHR 0.76, 95% CI 0.67 to 0.85) and JAKi (aHR 0.75, 95% CI 0.67 to 0.83) were less frequently discontinued for ineffectiveness compared with TNFi (online supplemental figure 2), but tended to be discontinued more often for adverse events (JAKi aHR 1.16, 95% CI 1.03 to 1.33; IL-6i: 1.09, 95% CI 0.85 to 1.03). Female gender (aHR 1.22, 95% CI 1.08 to 1.38) increased the hazard of discontinuation for adverse events, but not for ineffectiveness or for other reasons. Age also increased the hazard of discontinuation for adverse events (aHR 1.01, 95% CI 1.01 to 1.02 per additional year of age), but decreased the hazard of discontinuation for ineffectiveness and other reasons.
Response rates
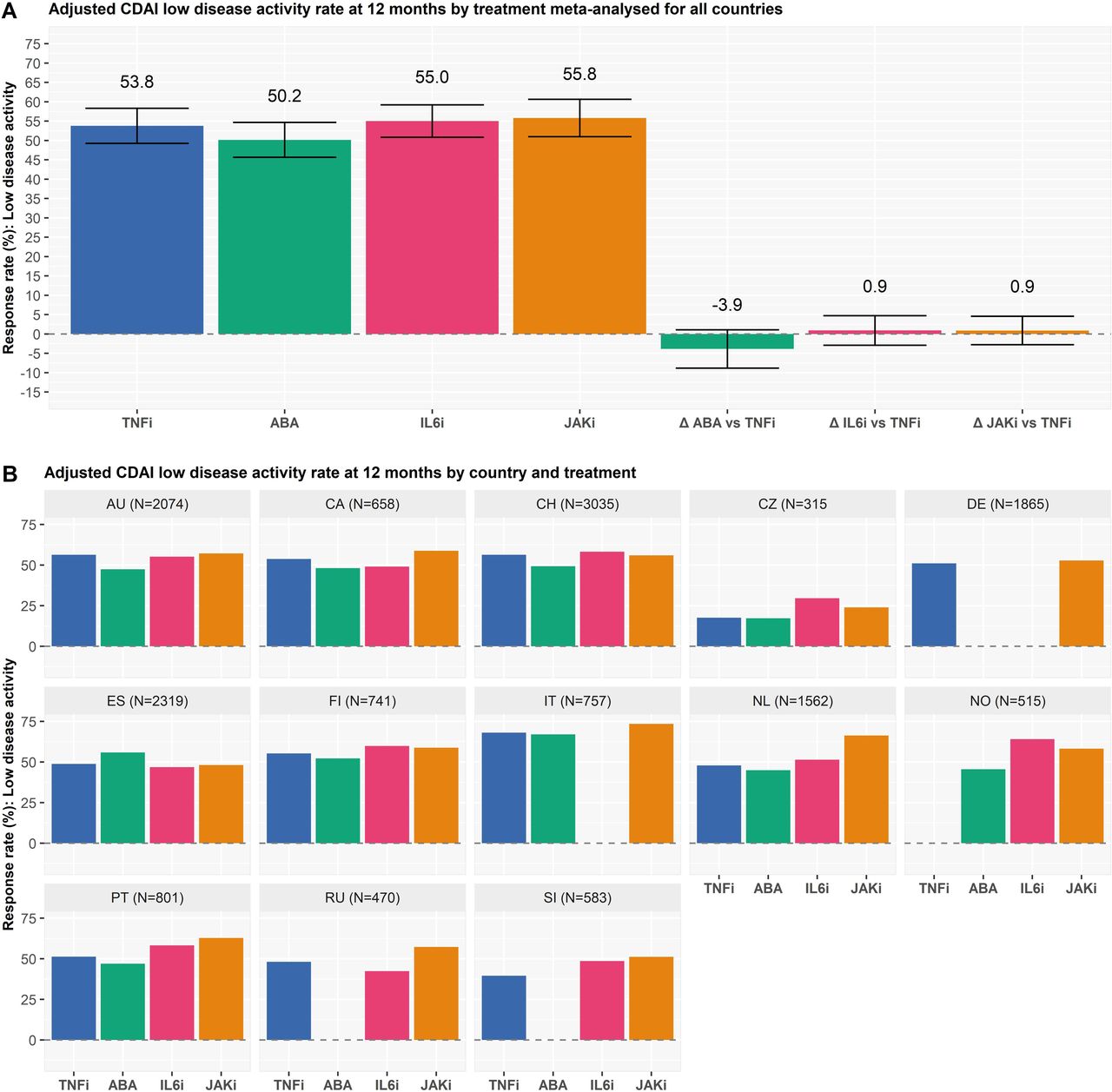
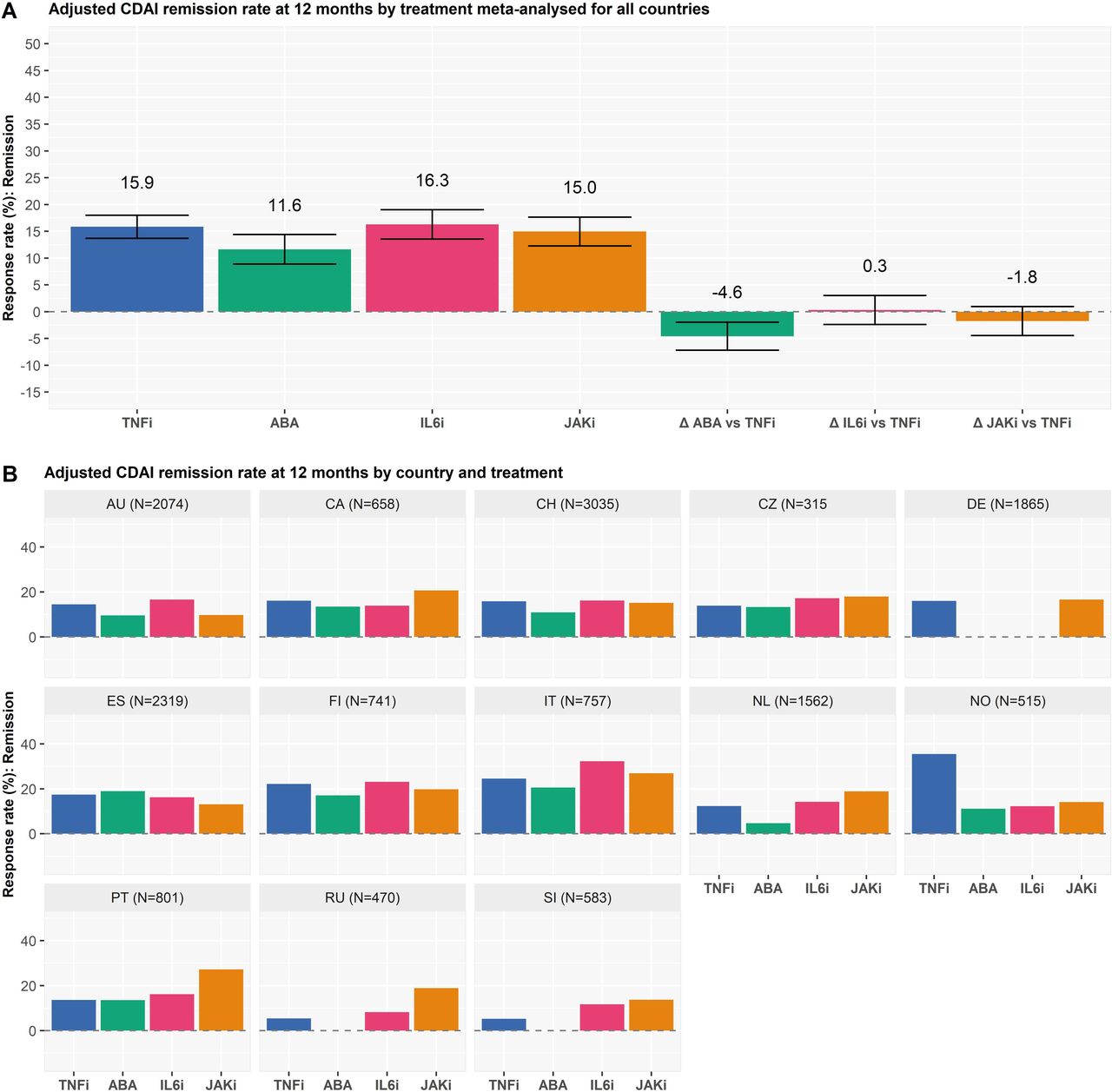
In the 13 registers with individual treatment course-level data and available CDAI information during follow-up (8,404 TNFi, 1523 ABA, 1843 IL-6i, 3,925 JAKi), the overall adjusted 1 year response rates was generally similar (figures 3 and 4). The adjusted response rates were slightly lower for ABA (50% for LDA and 12% for remission, figures 3 and 4) compared with the other groups (54% LDA and 16% remission for TNFi, 55% and 16% for IL-6i and 56% and 15% for JAKi), and the difference reached significance when comparing the proportion of patients on ABA to TNFi for remission (difference in LDA −3.9%, 95% CI −8.9 to −1.1%; difference in remission −4.6%, 95% CI −6.7 to −1.3%). No significant differences existed in response rates at 1 year between JAKi, IL-6i and TNFi (difference in LDA 0.9, 95% CI −2.8 to 4.7% for IL-6i vs TNFi; −0.9%, 95% CI −2.8 to 4.6% for JAKi vs TNFi; difference in remission 0.3%, 95% CI −2.4 to 3.0% and −1.8%, 95% CI −4.4 to 1.0%).

Adjusted CDAI low disease activity rates at 12 months for the 14 registers with individual treatment course-level data and CDAI information during follow-up (A) by treatment meta-analysed for all countries (B) by country and treatment. analysis was adjusted for age, gender, disease duration, seropositivity, number of previous treatments, concomitant treatment with csDMARDs, concomitant treatment with glucocorticoids, CRP, HAQ, CDAI at baseline, comorbidities, smoking and BMI. DE, SI and RU do not have or provide data on ABA. DE did not provide data on IL6i. All countries rates are combined using a meta-analysis with random effect. TNFi: TNF inhibitors, ABA: abatacept, IL6i: IL6 inhibitors, JAKi: Janus kinase inhibitors, ∆ ABA vs TNFi: difference in the response rate between abatacept and TNF inhibitors, ∆ IL6i vs TNFi: difference in the response rate between IL6 inhibitors and TNF inhibitors, ∆ JAKi vs TNFi: difference in the response rate between JAK inhibitors and TNF inhibitors. AU: Austria, CA: Canada, CH: Switzerland, CZ: Czech Republic, DE: Deutschland, ES: Spain, FI: Finland, IT: Italy, NL: Netherlands, no: Norway, Pt: Portugal, Ro: Romania, RU: Russia, SI: Slovenia. BMI, body mass index; CDAI, Clinical Disease Activity Index; CRP, C reactive protein; csDMARDs, conventional synthetic disease-modifying anti-rheumatic drugs; HAQ, Health Assessment Questionnaire.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Adjusted CDAI remission rates at 12 months for the 14 registers with individual treatment course-level data and CDAI information during follow-up (A) by treatment meta-analysed for all countries (B) by country and treatment. analysis was adjusted for age, gender, disease duration, seropositivity, number of previous treatments, concomitant treatment with csDMARDs, concomitant treatment with glucocorticoids, CRP, HAQ, CDAI at baseline, comorbidities, smoking and BMI. All countries rates are combined using a meta-analysis with random effect. DE, SI and RU do not have or provide data on ABA. DE did not provide data on IL6i. TNFi: TNF inhibitors, ABA: abatacept, IL6i: IL6 inhibitors, JAKi: JAK inhibitors, ∆ ABA vs TNFi: difference in the response rate between abatacept and TNF inhibitors, ∆ IL6i vs TNFi: difference in the response rate between IL6 inhibitors and TNF inhibitors, ∆ JAKi vs TNFi: difference in the response rate between JAK inhibitors and TNF inhibitors. AU: Austria, CA: Canada, CH: Switzerland, CZ: Czech Republic, DE: Deutschland, ES: Spain, FI: Finland, IT: Italy, NL: Netherlands, NO: Norway, PT: Portugal, Ro: Romania, RU: Russia, SI: Slovenia. BMI, body mass index; CDAI, Clinical Disease Activity Index; CRP, C reactive protein; csDMARDs, conventional synthetic disease-modifying antirheumatic drugs; HAQ, Health Assessment Questionnaire.
Discussion
In this large international collective of registers, we found similar overall drug retention rates between treatment groups. Compared with TNFi, IL-6i and JAKi were less frequently discontinued for ineffectiveness, while JAKi and IL-6i tend to be more frequently discontinued for adverse events, furthermore, disease activity, adjusted for confounders and treatment discontinuation, was similar. More than half of patients with RA reached LDA state at 1 year and one out of seven, remission.
In this study, we compared the effectiveness of four classes of second-line treatment for RA with different mechanisms of action, including JAKi. JAKi are the latest class of advanced therapies and have the advantage of oral administration. Various randomised controlled trials have demonstrated JAKi being more efficacious than methotrexate, and non-inferior or even better on some outcomes than certain bDMARDs.9 10 18 Beyond their proven efficacy, safety issues have raised questions on the impact these drugs would have on the management of patients with RA in routine care.19 Contrasting with the short duration and the relatively limited number of patients included in randomised controlled trials, our study, conducted on a large sample of patients seen in daily clinical practice, enables to better appraise the persistence of therapy, a composite endpoint incorporating clinical effectiveness and safety, in comparing TNFi vs JAKi, ABA or IL-6i. We found a similar retention rate between these four treatment groups. These results are in line with recent evidence from a couple of smaller observational studies.10 Recently, data from the Swiss RA register found in a real-world setting that the persistence on tofacitinib did not differ from ABA or IL-6i, and was slightly better than TNFi.20 Like in this study, TNFi was discontinued more often for ineffectiveness and less for safety reasons compared with JAKi and treatment with other modes of action (including IL-6i).
The retention rates were heterogeneous among the participating countries, possibly reflecting national differences in physician’s treatment choices and prescribing patterns. An investigation of national treatment guidelines or access to second line therapies, which could explain some of the national discrepancies, did not identify specific differences in access, eligibility criteria or prescription patterns among participating countries.21 Other researchers have described the wide variability of drug retention among countries and found that it is in general not related to disparities in patient or disease characteristics, but to differences in health systems or surrogates thereof, such as national gross domestic product per capita.22 To avoid biasing or wrongly assuming overly precise estimates, all main analyses reported herein were meta-analysed using random effect. The main single reason for discontinuation was ineffectiveness for all treatments, but JAKi tended to be discontinued more frequently for adverse events and less for ineffectiveness compared with TNFi, although the effect size was small. It is possible that less experience in the treatment with JAKis and differences in the perceived or factual utility and safety of JAKi, in particular considering the warnings of medicine agencies, could contribute to this finding. However, most of our observations predate these communications and the publication of the results of the ORAL surveillance study.19 To what extent this phenomenon mirrored a real ‘biological’ behaviour of JAKi remains to be further investigated.
Our study has some limitations. First, treatment was not randomly assigned opening the possibility for confounding. Though we used robust methods and statistical techniques to draw causal inferences from observational data, there is certainly some residual and/or unmeasured confounding, which could change the estimated associations. Nevertheless, only observational studies with large sample size can detect small effect sizes for safety concerns23 24 and the adjustment was relatively comprehensive, except for a low granularity on type of comorbidities. Second, use of meta-analysis to combine national estimates limits the evaluation of the factors associated with effectiveness. Third, we did not fully evaluate safety in this study, though it was one of the reasons for discontinuation, as we do not currently have details on the specific adverse events that led to discontinuation nor their severity in this dataset. Indeed, as for all observational register studies, detailed quality check of the recorded adverse events and careful consideration of potential confounders for each adverse event will be necessary to produce trustworthy results. Moreover, for several treatment courses, discontinuation reasons other than ineffectiveness or adverse events were recorded, without more granularity to explore, as the categories chosen had to match all the registers; for several treatment courses, no reasons of stopping were recorded, and they could not be evaluated for this outcome. Finally, we grouped all JAKi agents into one category and did not explore potential differences in effectiveness among them. It is possible that individual JAKi have different effectiveness and safety profiles.
The strength of our study relies on the availability of the data of the largest collaborative international effort to date aiming at providing information on the real-world management of patients with RA in different countries. The clinical relevance of these results should therefore not be undermined by issues of low generalisability, as occurs in randomised controlled trials. Moreover, we provide an evaluation and a comparison of the effectiveness across different routinely prescribed alternative drugs.
In conclusion, our results support the use of these four treatments for treating patients with RA in ‘real-world’ clinical care, underscoring their similar effectiveness, as assessed by retention and response rates, which were comparable. However, we found an increased discontinuation of JAKi for safety reasons compared with TNFi, which could be due to a combination of real differences in safety profile and heightened concerns from physicians and patients, causing them potentially to be more careful with this newer treatment.
Data availability statement
Data are available on reasonable request. All the data belong to the registers. Anonymised data can be shared as long as agreements are made with all participating registers.
Ethics statements
Patient consent for publication
Ethics approval
Local ethics committees (when required according to local legislation) approved the collection of data in each participating register, and the Geneva Ethics Committee approved this specific study (CCER 2017-02278, amendment 2).
Acknowledgments
The authors thank all the health professionals and patients who participated in the registers.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Josef S Smolen
Twitter @DiederikDeCock, @delcourvoisier
Correction notice This article has been corrected since it published Online First. The second author's name and affiliation number 7 has been corrected and minor errors in the text at the end of the “Response rates” paragraph, where the numbers do not correspond to the images.
Contributors All the authors have provided substantial contributions to the conception or design of the work, the acquisition of the data and the interpretation of data. KL and DSC performed the statistical analysis. KL, ML, DSC and AF wrote the first draft. All the other authors participated in the final drafting of the work or revising it critically for important intellectual content. All authors contributed to the final approval of the version published. KL and AF accepts full responsibility for the finished work and/or the conduct of the study, had access to the data, and controlled the decision to publish.
Funding Clinical work in Czech Republic was partially supported by the project from the Ministry of Health for conceptual development of research organisation MZ00023728023728 (Institute of Rheumatology). BIOBADASER has received funding from Fundacion Española de Reumatología, the Spanish Medicines and Health Products Agency (Agencia Española del Medicamento y Productos Sanitarios) and equal grants from pharmaceutical companies (AbbVie, BMS, Celltrion, Galapagos, Janssen, Lilly, MSD, Novartis, Pfizer, Regeneron, Roche, Samsung, Schering‐Plough and UCB). BioRx.si has received funding for clinical research paid to Društvo za razvoj revmatologije from AbbVie, Roche, Medis, MSD, Biogen, Amgen, Sanofi, Celgene and Pfizer. The British Society for Rheumatology Biologics Register in Rheumatoid Arthritis (BSRBR-RA) is funded by a grant from the British Society for Rheumatology (BSR). The BSR currently receives funding from Abbvie, Amgen, Celltrion HC, Eli Lilly, Pfizer, Samsung Bioepis, Sanofi, Sandoz and in the past Hospira, MSD, Roche, SOBI and UCB. This income finances a wholly separate contract between the BSR and The University of Manchester to host the BSRBR-RA. All decisions concerning study design, data capture, analyses, interpretation and publication are made autonomously of any industrial contribution. The BSRBR-RA would like to gratefully acknowledge the support of the National Institute for Health Research, through the Local Clinical Research Networks in England (and equivalent organisations in the devolved nations) at participating centres and the BSRBR-RA Control Centre Consortium. DANBIO was partially supported by public and private funding (AbbVie, Biogen, Bristol Myers Squibb, Eli Lilly, MSD, Novartis, Pfizer, Roche, Sanofi, UCB). NOR-DMARD was has been supported with research funding to Diakonhjemmet Hospital from AbbVie, Amgen, BMS, MSD, Novartis, Pfizer and UCB. The RABBIT register is currently supported by an unconditional grant with equal parts from AbbVie, Amgen, BMS, Celltrion, Fresenius Kabi, Galapagos, Hexal, Lilly, MSD, Viatris, Pfizer, Roche, Samsung Bioepis, Sanofi-Aventis, and UCB. REUMA. PT is supported by unrestricted grants from Abbvie, Biogen, Celgene, MSD, Roche, Sanofi and Pfizer. ROB-FIN is funded by AbbVie, Hospira, BMS, MSD, Pfizer, Roche and UCB. The Romanian Registry of Rheumatic Diseases (RRBR) uses unrestricted grants from AbbVie, Pfizer, Eli Lilly, Ewopharma, Nopvartis MSD, Roche, UCB, and BMS. Swiss Clinical Quality Management in Rheumatic Diseases (SCQM) database is sponsored by public and industrial support (http://scqm.ch/en/sponsoren/).
Competing interests KL reports personal fees from Gilead-Galapagos, Pfizer, Viatris, Celltrion, outside the submitted work. ML reports speaking fee from Boehringer Inghelheim, outside the submitted work. DM has nothing to disclose. SAB report grants from Pfizer, outside the submitted work. DC report grants, personal fees and non-financial support from Abbvie, grants, personal fees and non-financial support from Amgen, grants, personal fees and non-financial support from BMS, grants, personal fees and non-financial support from Eli Lilly, grants, personal fees and non-financial support from Merck, grants, personal fees and non-financial support from Novartis, grants, personal fees and non-financial support from Pfizer, grants, personal fees and non-financial support from Roche, grants, personal fees and non-financial support from Sanofi-Genzyme, grants, personal fees and non-financial support from UCB, grants, personal fees and non-financial support from Sandoz, outside the submitted work. CC reports personal fees from Abbvie, Amgen, Boehringer Ingelheim, Ewopharma, Lilly, Novartis, Pfizer outside the submitted work. RC has nothing to disclose. DDC has nothing to disclose. LD reports institutional grant from BMS outside the present work and speakers bureau from Eli Lilly and Galderma. OE has nothing to disclose. E-MH reports personal fees from AbbVie, Sanofi, Sobi ; institutional grants from Novo Nordic Foundation, Danish Rheumatism Association, Danish Regions Medicine Grants, Roche, Novartis, AbbVie outside the submitted work. DH has nothing to discloseKLH reports honoraria from Abbvie and grants from Pfizer and BMS outside the submitted work, and is supported by the NIHR Manchester Biomedical Research Centre. FI reports speaking fees from Abbvie, BMS, Eli-Lilly, Roche, MSD, Galapagos, Pfizer, Celltrion, Janssen outside the submitted work. NI reports grants from Roche, Pfizer, personal fees from AbbVie, Roche, Pfizer, UCB, Novartis,Amgen, Lilly, MSD. LK-F has nothing to disclose. EKK has nothing to disclose. TKK reports fees for speaking and/or consulting last 2 years from AbbVie, Amgen, Celltrion, Egis, Evapharma, Ewopharma, Gilead, Hikma, Janssen, Mylan, Novartis, Oktal, Pfizer, Sandoz, UCB. BFL reports personal fees from Abbvie, personal fees from Biogen, personal fees from Celgene, personal fees from Eli Lilly, personal fees from MSD, personal fees from Pfizer, personal fees from Roche, and personal fees from Novartis and Sandoz. GL reports personal fees from Abbvie, personal fees from Eli Lilly, personal fees from MSD, personal fees from Novartis, personal fees from Pfizer, personal fees from Roche, personal fees from Janssen, personal fees from BMS, outside the submitted work. DCN reports grants from Roche, during the conduct of the study; personal fees from Abbvie, personal fees from BMS, grants from Celgene, personal fees from Lilly, grant from MSD, personal fees from Novartis, personal fees from Pfizer, personal fees from UCB, outside the submitted work. KP has received honoraria for lectures and consultations from: AbbVie, BMS, Egis, Roche, Amgen, MSD, Medac, Eli Lilly, Pfizer. MPS reports personal fees from Janssen, MSD, Sanofi, outside the submitted work. ZR honoraria for lectures and consultations from: Abbvie, Pfizer, MSD, Medis, Roche, outside the submitted work. MJS reports personal fees from AbbVie, personal fees from Pfizer, personal fees from Novartis, personal fees from Roche, outside the submitted work. AS reports speaker honoraria from AbbVie, BMS, MSD, Pfizer, and Roche. PV reports speakers bureau for Eli Lilly, MSD, Galapagos, Roularta, consultancy fees from Galapagos, Gilead, Pfizer, Sanofi, Sidekick Health, Eli Lilly, Nordic Pharma, ABBVIE, Celltrion, BMS, UCB and is the grant holder from the Pfizer Chair Management of Early Rheumatoid Arthritis at KU Leuven. DSC has nothing to disclose. AF reports grants from AbbVie, BMS, Eli-Lilly, Galapagos and Pfizer and speaker honoraria (educational events or symposia) from companies producing several of the targeted therapies that are included in this analysis (honoraria < 10’000 USD): AbbVie, BMS, Eli-Lilly, Gilead, MSD, Pfizer. Clinical work in Czech Republic was partially supported by the project from the Ministry of Health for conceptual development of research organisation MZ00023728023728 (Institute of Rheumatology). BIOBADASER has received funding from Fundacion Española de Reumatología, the Spanish Medicines and Health Products Agency (Agencia Española del Medicamento y Productos Sanitarios) and equal grants from pharmaceutical companies (AbbVie, BMS, Celltrion, Galapagos, Janssen, Lilly, MSD, Novartis, Pfizer, Regeneron, Roche, Samsung, Schering‐Plough and UCB). BioRx.si has received funding for clinical research paid to Društvo za razvoj revmatologije from AbbVie, Roche, Medis, MSD, Biogen, Amgen, Sanofi, Celgene and Pfizer. The British Society for Rheumatology Biologics Register in Rheumatoid Arthritis (BSRBR-RA) is funded by a grant from the British Society for Rheumatology (BSR). The BSR currently receives funding from Abbvie, Amgen, Celltrion HC, Eli Lilly, Pfizer, Samsung Bioepis, Sanofi, Sandoz and in the past Hospira, MSD, Roche, SOBI and UCB. This income finances a wholly separate contract between the BSR and The University of Manchester to host the BSRBR-RA. All decisions concerning study design, data capture, analyses, interpretation and publication are made autonomously of any industrial contribution. The BSRBR-RA would like to gratefully acknowledge the support of the National Institute for Health Research, through the Local Clinical Research Networks in England (and equivalent organisations in the devolved nations) at participating centres and the BSRBR-RA Control Centre Consortium. DANBIO was partially supported by public and private funding (AbbVie, Biogen, Bristol Myers Squibb, Eli Lilly, MSD, Novartis, Pfizer, Roche, Sanofi, UCB). NOR-DMARD was has been supported with research funding to Diakonhjemmet Hospital from AbbVie, Amgen, BMS, MSD, Novartis, Pfizer and UCB. The RABBIT register is currently supported by an unconditional grant with equal parts from AbbVie, Amgen, BMS, Celltrion, Fresenius Kabi, Galapagos, Hexal, Lilly, MSD, Viatris, Pfizer, Roche, Samsung Bioepis, Sanofi-Aventis, and UCB. REUMA. PT is supported by unrestricted grants from Abbvie, Biogen, Celgene, MSD, Roche, Sanofi and Pfizer. ROB-FIN is funded by AbbVie, Hospira, BMS, MSD, Pfizer, Roche and UCB. The Romanian Registry of Rheumatic Diseases (RRBR) uses unrestricted grants from AbbVie, Pfizer, Eli Lilly, Ewopharma, Nopvartis MSD, Roche, UCB, and BMS. Swiss Clinical Quality Management in Rheumatic Diseases (SCQM) database is sponsored by public and industrial support (http://scqm.ch/en/sponsoren/).
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.