Article Text

Abstract
Background The registration trials of messenger RNA (mRNA) vaccines against SARS-CoV-2 did not address patients with inflammatory rheumatic diseases (IRD).
Objective To assess the humoral response after two doses of mRNA vaccine against SARS-CoV-2, in patients with IRD treated with immunomodulating drugs and the impact on IRD activity.
Methods Consecutive patients treated at the rheumatology institute, who received their first SARS-CoV-2 (Pfizer) vaccine, were recruited to the study, at their routine visit. They were reassessed 4–6 weeks after receiving the second dose of vaccine, and blood samples were obtained for serology. IRD activity assessment and the vaccine side effects were documented during both visits. IgG antibodies (Abs) against SARS-CoV-2 were detected using the SARS-CoV-2 IgG II Quant (Abbott) assay.
Results Two hundred and sixty-four patients with stable disease, (mean(SD) age 57.6 (13.18) years, disease duration 11.06 (7.42) years), were recruited. The immunomodulatory therapy was not modified before or after the vaccination. After the second vaccination, 227 patients (86%) mounted IgG Ab against SARS-CoV-2 (mean (SD) 5830.8 (8937) AU/mL) and 37 patients (14%) did not, 22/37 were treated with B cell-depleting agents. The reported side effects of the vaccine were minor. The rheumatic disease remained stable in all patients.
Conclusions The vast majority of patients with IRD developed a significant humoral response following the administration of the second dose of the Pfizer mRNA vaccine against SARS-CoV-2 virus. Only minor side effects were reported and no apparent impact on IRD activity was noted.
- COVID-19
- autoimmune diseases
- vaccination
- antirheumatic agents
- biological therapy
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information. All data relevant to the study are included in the article. Data are under embargo by local authorities if not included into the manuscript.
This article is made freely available for use in accordance with BMJ’s website terms and conditions for the duration of the covid-19 pandemic or until otherwise determined by BMJ. You may use, download and print the article for any lawful, non-commercial purpose (including text and data mining) provided that all copyright notices and trade marks are retained.
https://bmj.com/coronavirus/usageStatistics from Altmetric.com
Key messages
What is already known about this subject?
There is very limited data regarding the safety, the humoral immunogenicity and the impact on the rheumatic disease, of two doses of messanger RNA (mRNA) vaccine against SARS-CoV-2, in patients with inflammatory rheumatic diseases (IRD) treated with immunomodulating agents.
What does this study add?
Our study included a diverse, relatively large size cohort (compared with the data published so far) exposed to widely diverse immunomodulatory treatments including the use of B cell-depleting agents.
We showed that despite continuing chronic immunosuppression, patients with IRD mounted significant amounts of protective antibodies.
The humoral response was influenced by the type of the immunomodulatory treatment and not by the type of IRD.
B cell-depleting agents significantly impair antibody production, particularly in older patients.
No IRD flare ups were observed following vaccination of patients with IRD.
How might this impact on clinical practice or future developments?
The two dose Pfizer–BioNTech COVID-19 vaccine is safe in stable patients with IRD.
The antibody titres are influenced by the type of the immunotherapy.
So far there is no proof that the antibody titres correlate with improved protection against COVID-19.
Introduction
The registration trials of messenger RNA (mRNA) vaccines against SARS-CoV-2 did not address patients with inflammatory rheumatic diseases (IRD).1 2 Concerns were raised whether these patients can mount a protective immune response and whether the vaccination may trigger a flare up of the IRD. Previous studies showed that most protein-based vaccines induce protective antibody titres in patients with IRD.3 However, the humoral response was found to be blunted in some patients treated with CD20-depleting antibodies (Abs) or immune suppression.4 Recently, Geisen et al reported on the humoral response induced by mRNA vaccines against SARS-CoV-2 and their safety in 26 patients with IRD, but no patients on B cell-depleting therapy were included.5 Boyarsky et al reported interim immunogenicity data after one dose of mRNA vaccine in 123 patients with IRD who were recruited via social media.6
We wish to report the humoral response after the second dose of mRNA vaccine against SARS-CoV-2, in a well-defined cohort of patients with IRD treated with disease-modifying antirheumatic drugs (DMARDs) under careful rheumatologists’ follow-up and the impact of the vaccine on IRD activity.
Materials and methods
Consecutive patients treated at a single tertiary referral rheumatology centre, who received their first SARS-CoV-2 (Pfizer) vaccine, were recruited during their routine visit. The inclusion criteria were established diagnosis of IRD, receival of the first dose of the BNT162b2 mRNA vaccine and agreement to participate in the study. The visit included IRD activity assessment (disease activity score (DAS)28), patient global assessment (PGA), physician global assessment (PhGA) and questioning regarding the vaccine side effects. All patients received the BNT162b2 mRNA vaccine according to Israeli Ministry of Health regulations. The second dose of vaccine was administrated 3 weeks after the first dose. The vaccination was not part of the study. The patients were invited for serology tests and additional IRD assessment 4–6 weeks after the second dose of vaccine. Patients who did not receive the second dose of vaccine were excluded from the study.
A comparison group of patients with IRD who reported, at their routine visit at the rheumatology clinic of COVID-19 disease (diagnosed by positive SARS-CoV-2 PCR) within the previous 2 months, was recruited to the study. The patients were assessed for IRD activity and neutralising Abs within 4–8 weeks after the recovery (symptomatic recovery and negative SARS-CoV-2 PCR).
Neutralising IgG Abs against SARS-CoV-2 virus were detected using the SARS-CoV-2 IgG II Quant (Abbott) assay based on a chemiluminescent microparticle immunoassay on the ARCHITECT ci8200system from Abbott. This assay measures IgG Abs against the spike receptor-binding domain (RBD) of the virus. IgG Abs against the spike (S) RBD of the virus are defined as neutralising Abs since the spike (S) protein contains an RBD that can specifically bind to angiotensin-converting enzyme 2, the receptor on target cells in the host.7 The test is considered positive above 50 AU/mL. We did not use a neutralising assay.
The study was approved by the local ethical committee (the Ethics Committee of Rambam Health Care—417-20). Informed consent was obtained from all study participants prior to the initiation of any study procedure.
Statistical analysis: we used SPSS software (IBM SPSS Statistics for Windows, V.27, IBM, Armonk, New York, 2020). All statistical tests were two sided, statistical significance was defined as p value below 0.05. Categorical variables were summarised as frequency and percentage. Continuous variables were evaluated for normal distribution using histogram and Q–Q plots and reported as median and IQR. Association between continuous variables was evaluated using Spearman correlation. Association between categorical variables was evaluated using χ2 test or Fisher exact test. Continuous variables were compared using Kruskal-Wallis test or Mann-Whitney test. Multivariate logistic regression was used to compare patients with humoral response versus patients without response, while controlling for potential confounders.
Results
We recruited 264 consecutive patients ((76% women) mean (SD) age 57.6 (13.18) years, disease duration 11.06 (7.42) years), who received their first SARS-CoV-2 (Pfizer) vaccine and 26 COVID-19 recovered patients (73% women), (mean (SD) age 47.3 (16.73) years, disease duration 6.53 (4.76) years).
The IRD diagnoses of the vaccinated patients are described in table 1. The treatment regimens included conventional synthetic (cs)DMARDs only, biological/targeted synthetic (b/ts)DMARDs only or combinations of the two (23%, 23%, 336%, respectively). Corticosteroids were used by 3% (mean dose (range) 5.6 mg (2.5–20 mg) prednisone). None of the patients discontinued immunomodulatory therapy before or after the vaccination. All the patients had stable disease (DAS28 (C-reactive protein (CRP)) mean (SD) 2.9 (1.7), PGA 3.4 (1.5), PhGA 2.6 (1.8).
Clinical characteristics and immunomodulatory therapy of vaccinated and COVID-19 recovered patients
After the second vaccination, 227 patients (86%) mounted a significant humoral response of neutralising IgG Ab against SARS-CoV-2 virus (mean (SD) 6764.27 (9291.61) AU/mL, median 3058 AU/mL, range 58–40000) and 37 patients (14%) did not: 24 out of 47 rituximab-treated patients (1.5–12 months before), 3 out of 8 abatacept-treated patients, 4 out of 21 patients treated with mycophenolate mofetil (MMF) only, 2 out of 11 belimumab-treated patients (one patient also received MMF), 1 out of 5 anti-IL17-treated patients, 1 patient treated with prednisone 20 mg, 1 patient treated with chemotherapy for a lung neoplasm and the only patient treated with obinutuzumab (figure 1). The demographic and clinical data of the patients who did not mount a significant humoral response are shown in the online supplemental table 3. We performed univariate analysis and multivariate logistic regression analysis which included age, disease duration, type of rheumatic disease, type of treatment (methotrexate (MTX), MMF, all csDMARDS, all b/tsDMARDs, anti-tumour necrotising factor (anti-TNF), anti-interleukins, antiCD20, belimumab, abatacept, combination csDMARDs +b/tsDMARDs, prednisone). The type of the immunomodulatory treatment influenced the humoral response and not the IRD diagnosis (table 2A, figure 2). In multivariate logistic regression analysis, only IRD duration, treatment with anti-CD20, abatacept or MMF were associated with the humoral response (table 2B).
Supplemental material
Humoral response—univariate and multivariate analyses
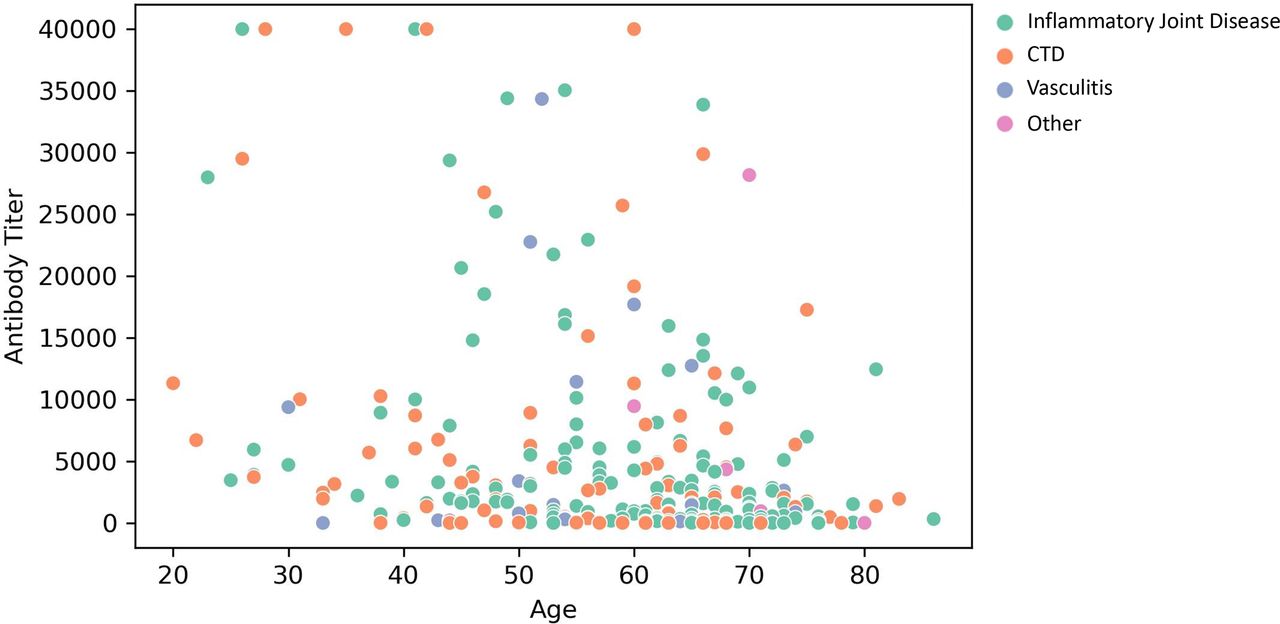
Serology per age, classification by disease Scatter plots of antibody titre level by age. Spearman rank correlation coefficient corresponds to −0.24. Colours represent different disease groups: inflammatory joint disease, connective tissue disease, vasculitis and other diseases. CTD, connective tissue diseases.

{kind=link}
{kind=link}
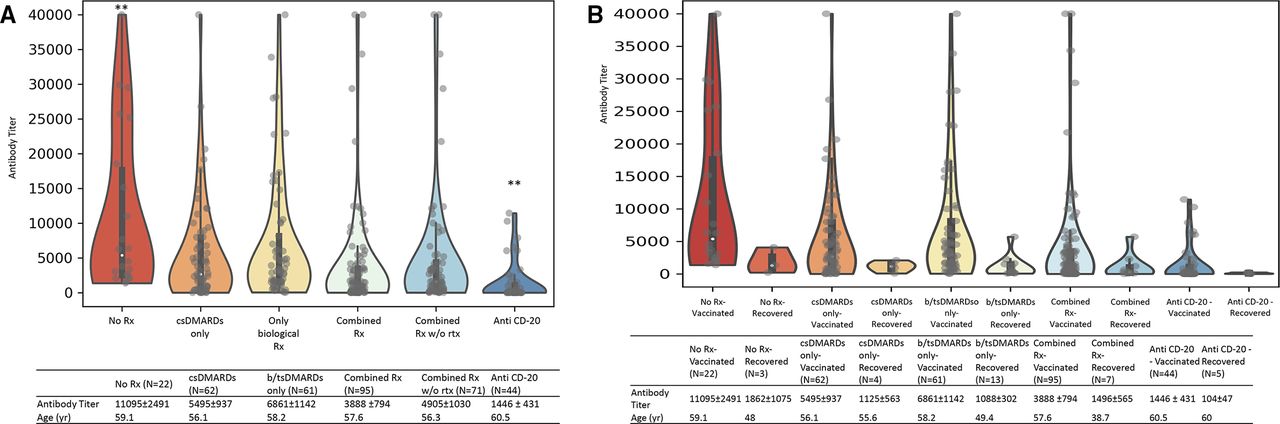
(A) Antibody titres for the different treatments presented as violin plots with included boxplots. The violin illustrates the kernel probability density of antibody titres, and the boxplot indicates the median and quartiles with whiskers up to 1.5 times the IQR. (B) Violin plots of antibody titres for the different treatments in vaccinated and COVID-19 recovered patients. Mean antibody titres±SE per treatment group. **p-value<0.01; Rx- treatment. csDMARDs, conventional synthetic disease-modifying antirheumatic drugs; b/tsDMARDs, biological/targeted synthetic DMARDs; rtx, rituximab; combined Rx, csDMARDs+b/tsDMARDs; combined Rx w/o rtx, combined treatment without rituximab.
Treatment with csDMARDs, MTX, anti-CD20, anti-interleukins and older age was associated with lower levels of neutralising IgG Ab against SARS-CoV-2 (online supplemental table 4). Only
10 out of 78 MTX-treated patients did not mount a significant humoral response (seven patients received concomitant treatment with rituximab, one with abatacept and another with 20 mg prednisone). When we excluded the patients who received MTX and concomitant rituximab treatment, this difference was not significant anymore.
Fifty-two per cent of anti-CD20-treated patients did not develop a significant humoral response. Comparing the anti-CD20 group with humoral response with the one without, it did not reveal any statistically significant difference regarding type of IRD, concomitant treatment, the levels of immunoglobulins prior to rituximab treatment, the number of rituximab courses (mean (SD) 5 (3.19), median five courses vs 5.75 (3.2), 5, p=0.43) or the timing of the last rituximab course related to the vaccination (mean (SD) 9.2 (6.3), median 9 months vs 6.04 (5.5), 5 months, p=0.086). The only significant difference between the groups was the age of the patients (mean (SD) age 64.1 (10.9), median, 66.5 years in the group without humoral response, vs 56.4 (11.1), 55 years in the group with humoral response, p=0.021).
Interestingly, a granulomatosis with polyangiitis (GPA) rituximab-treated patient, who was hospitalised two times for severe COVID-19 disease and reactivation (2 months after rituximab treatment) and who did not have neutralising Abs on recovery, developed a significant humoral response after being vaccinated 4 months after his recovery (11 434 AU/mL—the patient was included in the vaccinated group).
Among the 26 patients with IRD who recovered from COVID-19: 18 patients (70%) received csDMARDs, 10 (38%) received combined treatment with csDMARDs and b/tsDMARDs, 8 (31%) received bDMARDs monotherapy and 13 patients (50%) corticosteroids (mean dose (range) 10.5 mg (2.5–20 mg) prednisone) (table 1). Only two patients, from the recovered COVID-19 group, did not have neutralising Abs: one RA rituximab-treated patient and one systemic sclerosis (SSc) patient treated with MMF and rituximab. Both patients were also on 10 mg prednisone chronic therapy. They both received rituximab treatment 2 months prior to COVID-19 disease; they had a mild viral disease. Only one patient with RA treated with high-dose steroids and immunoglobulins for pyoderma gangrenosum needed hospitalisation for severe COVID-19 disease and received oxygen support, remdesivir and antibiotics for secondary bacterial pneumonia. All the others had very mild COVID-19 disease or were asymptomatic. They did not receive any treatment for COVID-19 19 and the immunomodulatory treatment for the IRD was not discontinued.
The IgG Ab titres were significantly higher in the vaccinated patients compared with the recovered COVID-19 patients with IRD (mean (median) mean (SD) 6764.27 (9291.61) AU/mL, median 3058 AU/mL vs mean (SD) 2044.8 (4944.8), median 480 AU/mL, p<0.05 (figure 1).
The reported side effects of the vaccine were minor (local pain, redness or swelling at injection site—58%, fatigue—30%, muscle sore—12%, headache—20%, low grade fever—3%). One patient with Familial Mediterranean fever, interstitial lung disease and positive rheumatoid factor reported new-onset arthritis 2 weeks after the first dose of vaccine. No flare-up of the underlying IRD occurred within 2 months after vaccination in any other patient (DAS28 (CRP) before and after vaccination mean (SD) 2.9 (1.7) vs 2.8 (1.9), PGA 3.4 (1.5) vs 3.5 (1.6), PhGA 2.6 (1.8) vs 2.5 (1.8)) .
Discussion
The Pfizer mRNA vaccine against SARS-CoV-2 virus appears to be safe in our patients, only minor side effects were reported and no apparent impact on IRD activity was noted. The vast majority of patients with IRD developed a significant humoral response following the administration of the second dose of the vaccine, even though the immunomodulating treatment was not modified, either before or after the vaccination. The type of immunotherapy and the IRD duration influenced the humoral response. There was no statistically significant association between the type of the IRD or the patient’s age and the ability to develop a significant humoral response, although older patients had lower levels of IgG Abs. Previous studies reported a 100% and 97.9% humoral response in the healthy control group they used in their study.8 9 The age groups mean were 44 and 55 years for each study, so that it is very close to the age group of our cohort. Another study compared the humoral response in two age groups (<60 and >80 years) after the first and second Pfizer mRNA vaccine against SARS-CoV-2 virus and found lower IgG neutralising Abs in the elderly group (68.7%).10 Our cohort included only four patients older than 80 years.
Untreated and DMARDs-treated patients mounted Ab titres that were about one log higher than the patients treated with biologics and MMF. The IgG Ab titres were significantly higher in the vaccinated patients compared with the recovered COVID-19 patients with IRD. It is worth to emphasise that our cohort of recovered COVID-19 patients with IRD included mostly patients with very mild viral disease. The humoral response in patients with severe COVID-19 might be higher than the response in patients with mild disease. In a recently published study, Haberman et al found a diminished humoral response in MTX-treated patients.11 In our cohort, MTX did not have a negative impact on the ability to mount a significant humoral response, although the neutralising Ab levels were lower compared with those in patients without MTX (mean (SD) 4757 (8501) vs 6281 (9097) AU/mL). Worth to emphasise that 9 out of 10 MTX-treated patients with negative humoral response, in our cohort, were on concomitant treatment with rituximab, abatacept or high-dose prednisone. When we excluded these patients from the analysis, the difference was not statistically significant anymore. We do believe that the impairment of the humoral response might be attributed to the concomitant treatment (rituximab, abatacept, steroids) and not to the MTX. All the patients treated with anti-TNF agents, anti-interleukin six agents, anti-janus kinase (JAK) agents and most of the patients on belimumab treatment developed significant neutralising Ab levels. Our results are concordant with previous studies.5 6 Three out of eight abatacept-treated patients did not develop a significant humoral response. Due to the small number of abatacept-treated patients in our study, we cannot draw any conclusions regarding the impact of the drug on the humoral response, although the results are quite intriguing. Notably, 67% of the nonresponders were treated with B cell-depleting agents. Except for younger age, all other parameters including disease duration, type of IRD, concomitant immunomodulatory treatment, immunoglobulins levels, the number of previous rituximab treatment courses and the timing of last rituximab treatment were not significantly different between patients with positive humoral response to vaccine versus those with negative response. We do not have results of CD19 counts in these patients. We attribute the impaired response to vaccination in rituximab-treated patients to rituximab itself and not to the premedication with methylprednisolone because the median time between the treatment and vaccination was over a month, and the corticosteroid effect should wither within this time period (the longest interval between therapy and vaccination in a patient who did not develop Abs is 1 year, which is consistent with the long-term immunological effect).
The results regarding MMF are consistent with observed outcome of SARS-CoV-2 mRNA vaccination in the solid organ transplant population.12
The strength of our study is the inclusion of a diverse, relatively large size cohort (compared with the data published so far) exposed to widely diverse immunomodulatory treatments including the use of B cell-depleting agents. The cohort comprised patients with inflammatory joint diseases, vasculitis and connective tissue diseases, including a relatively large number of systemic sclerosis patients (our centre is a tertiary referral centre for systemic sclerosis). Moreover, the assessment of the IRD activity and the evaluation of the adverse events were performed by the treating rheumatologists of the recruited patients, who were all acquainted with the patient’s disease course.
We acknowledge that so far there are no data demonstrating a correlation between neutralising Ab levels and vaccine efficacy, therefore, caution is advised when instructing the patients how to conduct following the vaccine. Though of interest, the evaluation of the cellular immune response to vaccination was beyond the scope of our study. Future studies are awaited to define the best marker of protection against COVID-19. We plan to continue to follow these patients to assess whether the Ab titres correlate with clinical outcomes. Our main aim was to assess whether IRD patients, on immunomodulatory treatment, can mount a positive serologic response to mRNA vaccine against SARS CoV2 virus, therefore, we did not include a healthy control group. We complied with the current policy of vaccination that does not require Ab assessment before vaccination, previous infection was ruled out by history alone.
Our results can provide reassurance to patients with IRD treated with immunomodulatory agents and their physicians, regarding the immunogenicity and short-term safety of mRNA vaccine against SARS-CoV-2 virus. Considering the satisfactory humoral response despite the immunomodulatory treatments versus the increased risk for severe COVID-19 disease and the unknown vaccine efficacy and safety in patients with active IRD, we advise not to withhold immunomodulatory treatment around the vaccination. Further studies should assess whether lower Ab titres are associated with diminished protection against COVID-19-severe disease and whether the timing of anti-CD20 agents’ administration influences the neutralising Ab titre.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information. All data relevant to the study are included in the article. Data are under embargo by local authorities if not included into the manuscript.
Ethics statements
Ethics approval
The study was approved by the local ethical committee (the Ethics Committee of Rambam Health Care - 417-20).
Acknowledgments
We would like to thank Adi Abshalom-Mashiah, Vika Shataylo and Rita Erlich for organisational support.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Josef S Smolen
Contributors Study design: YB-M, AB-G. Sample collection: YB-M, DM, SG, KT, YT, KD, AB-G. Experiments and data analysis: YB-M, MK, MB, AB-G. Tables and figure: YB-M, MB. Data interpretation: YB-M, MK. Writing of the manuscript: YB-M, AB-G. Critical proofreading of the manuscript: all authors.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.